(1)
Klinik für Plastische Gesichtschirurgie, Marienhospital Stuttgart, Stuttgart, Germany
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-662-49706-7_13) contains supplementary material, which is available to authorized users.
Keywords
Tip deformityDisfigurement of the LLCsConcavity of the lateral cruraBucklingLLC malformationFold-over flap techniqueFold-under flap techniqueHorizontal mattress sutureUpside-down technique13.1 Surgical Principles
Naturally occurring malformations of the lower lateral cartilages (LLCs) are common, and the use of the open rhinoplasty approach makes the recognition and characterization of tip malformations far more reliable and precise. Likewise, many unsuccessful rhinoplasties result from the inability to properly recognize and treat congenital LLC malformations because of poor surgical exposure using the closed approach. Malformations of the nasal tip may occur unilaterally or bilaterally with variations in both type and magnitude. Virtually any segment of the LLC can be affected by congenital anomalies, including the medial crural footpods, the medial crura themselves, or the nasal domes. However, the most common site for naturally occurring tip malformations is the lateral crus, with crural concavity being the most commonly seen anomaly. Although most malformations of the LLC are associated with cosmetic disturbances, concave malformations of the lateral crura are also commonly associated with functional impairment, particularly in noses with weak lateral crura that are prone to inspiratory collapse or in noses with an adjacent septal deformity that exacerbates nasal valve obstruction. In the thin-skinned nose, concavities of the lateral crus are often visible externally, but overlying soft tissues may conceal smaller concavities, underscoring the importance of a careful endonasal examination as part of the preoperative evaluation process. While some LLC deformities are hidden by the overlying soft tissues, we prefer not to rely solely on soft-tissue camouflage for treatment. Instead, correction of all skeletal deformities is preferred in order to optimize both the functional and cosmetic results. Although Daniel feels that a slight crural concavity (coupled with convexity of the intermediate crura) will yield the best tip contour, we believe that flat and sturdy lateral crura yield not only a pleasant tip contour but also provide the structural rigidity necessary for reliable function of the nasal airway.
Many LLC deformities lend themselves to straightforward surgical correction. For example, asymmetrical or overly protrusive medial crural footpods can be corrected by transecting the medial crus just above the footpod and then coapting the footpods with intercrural sutures or transcutaneous mattress (transfixion) sutures. Alternatively, the footpods can be completely excised, and the columellar pedestal can be contoured with only transfixion sutures. Another common deformity is buckling of the intermediate crura within the infratip lobule. This can be corrected by suturing the intermediate crura to a columellar strut graft or, if unilateral, by performing a unilateral medial crural overlap procedure.
The most common LLC deformities are concavities of the lateral crura, which can be oriented longitudinally or transversely and which may be unilateral or bilateral. For transverse concave deformities of the lateral crus, excising and flipping the concave segment (upside-down technique (Fig. 13.1) is recommended, whereas we prefer leaving a narrow caudal rim strip to facilitate suture reattachment as recommended by Aiach (Fig. 13.2). Occasionally in bilateral deformities, the flipped segment is returned to the contralateral side (contralateral upside-down technique) to enhance bilateral symmetry.

Fig. 13.1
Upside-down technique
Fig. 13.2
(a, b) Modified Upside-down technique
In a longitudinally oriented concavity, a variety of techniques are possible. If the lateral crus is overly weak and the defect is small to intermediate in size, we prefer placement of horizontal mattress sutures to simultaneously flatten and stiffen the lateral crus (Fig. 13.3). As the mattress suture is slowly tightened, the concavity is gradually eliminated, and a knot is tied while the suture is held with forceps to prevent slippage. Typically, multiple sutures are placed in series to completely flatten and strengthen the affected crural segment. And unlike excisional techniques, the horizontal mattress suture technique is potentially reversible.
Fig. 13.3
(a, b) Horizontal mattress suture
Another option for treatment of a longitudinal crural concavity is the fold-over flap technique. In this technique, the cephalic margin is incised during a cephalic trim and is partially undermined so that it remains pedicled to the perichondrium just above the incision line. The flap is then rotated superiorly and inverted so that it rests on top of the crural concavity. When sutured to the underlying cartilage, the fold-over flap serves to fill the concavity as well as to strengthen and flatten the lateral crus (Fig. 13.4). Alternatively, the flap can be rotated in the opposite direction to fill a pocket created beneath the crural concavity. Again, suture fixation serves to flatten and strengthen the lateral crural remnant (Fig. 13.5). Although the fold-under flap is more effective at strengthening weak lateral crura, wide dissection of vestibular skin from beneath the lateral crus is more difficult and more time-consuming.
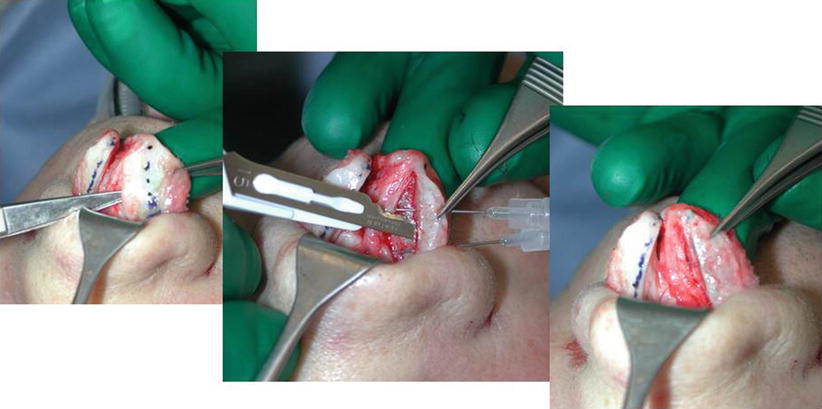

Fig. 13.4
Cephalic turn-over flap
Fig. 13.5
Cephalic fold-under flap
If the lateral crus is too narrow to permit a fold-over or fold-under technique, a batten graft fashioned from septal cartilage will simultaneously correct the crural concavity and eliminate the strength deficiency. Batten grafts are a valuable technique in both cosmetic and functional rhinoplasty (Fig. 13.6). For optimal cosmetic results, batten grafts should be carefully beveled along their outer edges for concealment. Batten grafts are sometimes positioned beyond the caudal border of the lateral crura to stabilize the alar rim against cephalic retraction and to simultaneously strengthen the alar rim against alar collapse. Similarly, batten grafts can also be extended laterally to prevent inward collapse of the lateral crura near the piriform aperture. Finally, if lateral crural concavity is combined with an overprojected tip, a lateral crural overlap technique is preferred, since both tip deprojection and crural flattening are accomplished simultaneously (Fig. 13.7).
Fig. 13.6
Batten graft technique
Fig. 13.7
(a, b) Lateral crural overlay technique
13.2 Case Studies
13.2.1 Primary Cases
13.2.1.1 Case 1: Horizontal Mattress Sutures
A 19-year-old female presented complaining of a peculiar-looking nasal tip. Examination revealed prominent concavities of both lateral crura and a tilted columella from caudal septal dislocation. Using the open approach, the caudal septum was repositioned and secured to a transverse drill hole created within the nasal spine. Fading (oblique) medial osteotomies, combined with percutaneous low-to-high lateral osteotomies, were then used to narrow the bony pyramid. For correction of the crural concavity, a cephalic trim was performed, and the excised cartilage was retained. After elevating the vestibular skin from the residual lateral crus, horizontal mattress sutures were used to flatten the concavity, and the previously excised cephalic specimen was used as an onlay batten graft for additional stability. The procedure was performed bilaterally. Owing to the additional crural rigidity obtained through the aforementioned procedures, spanning sutures could be used to control flaring without fear of recurrent crural collapse. A columellar strut graft was also placed to enhance tip support (Fig. 13.8).
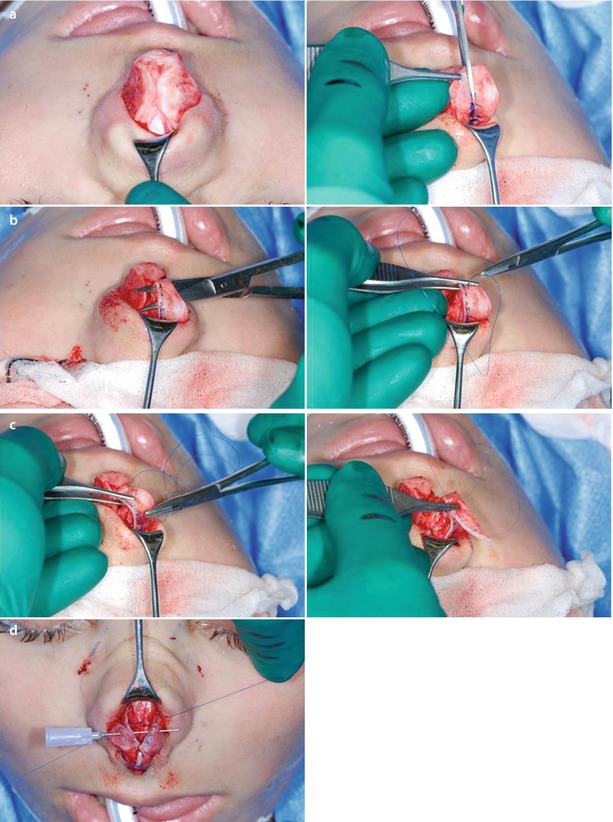

Fig. 13.8
(a) Cephalic resection. (b) Horizontal mattress sutures. (c) Batten graft from the excised cephalic portion. (d) Applying spanning sutures. (e) Placing a columellar strut. (f–h) Front view, profile view, base view pre-op/post-op
13.2.1.2 Case 2: Upside-Down Technique
A 31-year-old male presented after previous septoplasty complaining of persistent bilateral nasal obstruction that had failed to improve with septal surgery. Examination revealed bilateral lateral crural concavities, a persistent septal deviation, and bilateral synechiae. After opening the nose, deep transverse concavities were observed involving both lateral crura. After dividing the synechiae, the L-strut was straightened using spreader grafts. The concavities were corrected by excising the involved cartilage segments, turning the specimens 90°, and suturing each specimen to the contralateral defect to produce a modest bilateral crural convexity. Transdomal sutures and a tip graft were then used for further tip refinement, correcting both the crural concavities and the alar rounding simultaneously (Fig. 13.9).
Fig. 13.9
(a–b) Upside-down technique. (c–e) Front view, profile view, base view pre-op/post-op
13.2.1.3 Case 3: Upside-Down Technique
A 44-year-old male presented with nasal airway obstruction. Examination revealed pronounced concave collapse involving the central aspect of both lateral crura. Dynamic valve collapse was observed upon gentle nasal inspiration. Surgical exploration with the open approach revealed deep lateral crural concavities immediately adjacent to both nasal domes. After columellar strut placement, a left unilateral upside-down procedure was used to correct the left concavity and a septal onlay batten graft was used to fill the right concavity. Small onlay cartilage grafts were also used to fill concavities of the intermediate crura. Improved contour and nasal function were achieved (Fig. 13.10).

Fig. 13.10




(a–b) Upside-down technique. (c–e) Front view, profile view, base view pre-op/post-op
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
