CHAPTER 12 MACS facelift
Introduction/key points
• Modern facelifting techniques involve facial sculpturing combined with tension-free skin redraping. Sculpturing is achieved by suturing, judicious liposculpture, volume addition with microfat grafts, or a combination of these techniques.
• Our favored technique for minimally invasive facial rejuvenation is the MACS-lift (minimal access cranial suspension lift).
• A short-scar facelift is not the same as a traditional facelift with a short scar.
• A vertical vector in the face and neck is the rejuvenating one.
• Vertical facelifting techniques involve a temporal hairline incision to prevent sideburn elevation.
• Poor skin quality may require lengthening of the incision in the postauricular region to facilitate correct skin redraping.
Indications
 hours, under local anesthesia as an outpatient. In comparison to a traditional facelift, the MACS-lift involves a shorter scar, lower morbidity and a quicker recovery time.
hours, under local anesthesia as an outpatient. In comparison to a traditional facelift, the MACS-lift involves a shorter scar, lower morbidity and a quicker recovery time.Two variations of the procedure are described:
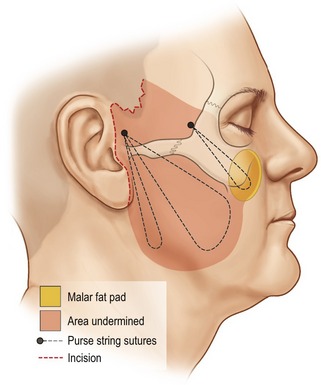
1. The simple MACS-lift (S-MACS), where two purse string sutures are placed to correct the lower third of the face and neck (the jowls, marionette grooves and the cervicomental angle).
2. The extended MACS-lift (X-MACS), where a supplementary third purse string suture is used to suspend the malar fat pad. This suture has an additional effect on the lower eyelid, the midface and the nasolabial groove.
Simple MACS-lift
Two purse string sutures are used to correct the jowls, the marionette grooves and the neck. They are anchored to the deep temporal fascia above the zygomatic arch, 1 cm in front of the auricular helix. The first suture runs as a narrow vertical U-shaped purse string towards the mandibular angle, incorporating the posterior border of the platysma muscle. Following liposuction of the neck, tying this suture under maximum tension produces a strong vertical lift on the lateral part of the platysma, correcting the cervicomental angle. The second purse string suture starts from the same anchoring point above the zygomatic arch and runs obliquely in the direction of the jowls as a wider O-shaped loop. Tying this suture corrects the jowls, the marionette grooves and downward slanting corners of the mouth (Fig. 12.1).
Extended MACS-lift
An additional point 2 cm below the lateral canthus is marked preoperatively with the patient sitting. This is the inferior limit of the third purse string suture and is included in the skin undermining. This suture also originates from the deep temporal fascia, but at its anterior aspect, lateral to the orbital rim. It provides strong correction of the nasolabial fold, enhancement of the malar region, lifting of the midface and shortening of the vertical height of the lower eyelid (Fig. 12.1).
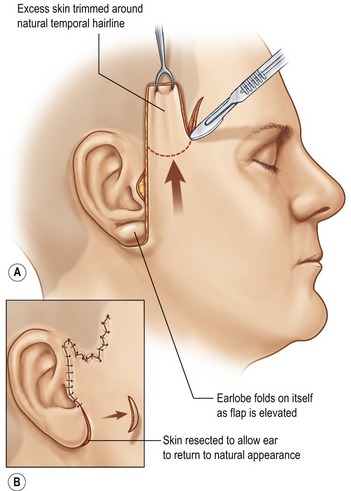
In both the S-MACS and X-MACS the skin is redraped in a completely vertical direction and skin excess above the temporal hairline incision is resected. As there is no lateral traction on the skin, there is no dog ear at the level of the earlobe, eliminating the need for a post-auricular extension of the incision (Fig. 12.2).
In classical teaching, smoking is considered an absolute contraindication to facelift surgery. As a result of the limited subcutaneous undermining and the absence of multiplanar dissection, we only consider smoking a relative contraindication to performing a MACS-lift.
Technical steps
Infiltration
Infiltration follows the sequence of procedures: first the upper eyelids, followed by the submental area, and finally the cheeks. (For the anesthetic solution see Table 12.1.)
Table 12.1 Anesthetic solution for MACS-lift
| 100 mL NaCl 0.9% |
| 20 mL lidocaine 2% |
| 10 mL ropivacaine 10 mg/mL |
| 2 mL sodium bicarbonate 8.4% |
| 0.2 mL levorenin 1 mg/mL |
| 10 mg triamcinolone |
Preoperative marking: incision
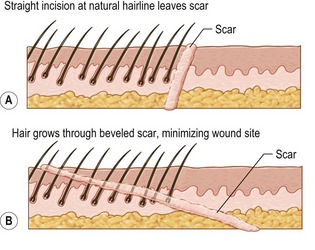
It continues forwards in a zigzag pattern, 2 mm within the lower and anterior aspect of the sideburn. In this part of the incision the knife is beveled at an angle almost tangential with the skin, cutting hair shafts perpendicularly (Fig. 12.3). This maneuver allows hairs to grow through the scar. After hair regrowth the scar will be hidden within the hairline and becomes virtually invisible. The purpose of the zigzag is to increase the length of the temporal incision making it a similar length to the cheek flap, reducing potential dog ear formation.
Suction lipectomy
In cases where microfat grafting is planned, the submental fat can be harvested with a special grating cannula (Fig. 12.4: “ToVer cannula,” Wells-Johnson, Tucson, AZ) which delivers fine-particle fat (1 mm diameter). If insufficient donor fat is present in the submental area, further fat can be harvested from the abdomen or love handles, using other cannulas (Fig. 12.5: “Becker Grater Round” cannula with 1 mm holes, Wells-Johnson, Tucson AZ).


Microfat grafting
Fat is prepared and injected as soon as possible after harvesting. We sieve it through a fine-meshed sterile cloth, rinsing away blood and oil with normal saline. The fat is injected with 18 G fat grafting cannulas (Fig. 12.6: Wells-Johnson, Tulip).

The skin puncture is made with a 16 G pink needle, and does not require closure after the procedure.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


