Introduction
Up until recently, lymphedema has largely remained on the sidelines of microsurgery. For many years, most microsurgeons avoided lymphatic reconstruction because of inconsistent results, lack of published data, and concerns regarding safety in a poorly understood disease process. Fortunately, the anecdotal era in lymphatic surgery is giving way to prospective studies and greater integration of our expanding knowledge of pathophysiology, imaging, and patient selection, into clinical practice. Advances in basic science, lymphatic imaging, and more sophisticated surgical techniques have resulted in a swell of interest in lymphatic surgery, which is now common in many academic centers. While there are currently still more questions than answers in lymphedema, we explore here some of the most popular techniques in lymphatic surgery as well as the latest insights into patient selection and operative approach.
Lymphatic Anatomy and Physiology
Revisiting the anatomy and physiology of the lymphatic system is useful, not only for lymphatic surgery, but also for other cosmetic and reconstructive procedures where increased awareness of this vast organ system may reduce the risk of injury to it. The lymphatic system is present throughout most of the body, although interestingly, it is not found in certain areas such as the central nervous system, or cartilage and bones. The lymphatic system as a whole serves three functions: fluid balance; transporting fats and fat-soluble vitamins from the gut to the circulation; and defending against microorganisms as well as tumor cells. As blood is pumped through the tissues and passes through the capillary network, most of the fluid that enters the interstitium returns through the venous system. The fluid waste that remains is removed by the lymphatics that can accommodate macromolecules that are too large to enter capillary venules, which have limited pore size. This is the basis for such studies as lymphoscintigraphy, that depend on preferential uptake of technetium sulfur colloid into the lymphatics because this agent is too large to fit through the limited pore size of a venule.
Lymphatic vessels also transport antigen and inorganic matter (such as silicone, noted in ruptured implants), via afferent vessels that enter the lymph node on its convex surface. Both B-cell and T-cell populations are located within the lymph node, where a coordinated adaptive immune response occurs following exposure to antigen via antigen presenting cells. Naive lymphocytes become activated and mature lymphocytes subsequently circulate through both the blood and lymph seeking out target antigen, re-entering the lymph node via high endothelial venules. The interconnections between the lymphatic sinuses and venules are the basis for Cheng’s proposed mechanism for lymph node transfer. After percolating through the lymph node, lymph exits through the efferent duct at the hilum where the feeding artery and vein perfuse the node.
The transport of lymph through this system of vessels and nodes is interesting, as there is no heart to pump fluid through this one-way street, which parallels the circulation of blood. Lymph is propelled independently by intrinsic smooth muscle contraction within the wall of the lymphatic vessels that is aided by unidirectional valves. Extrinsic skeletal muscle contraction also squeezes the lymphatic vessels, further facilitating lymph transit. This phenomenon is the underlying mechanism of action for short-stretch compression wraps that provide a firm surface against which muscle flexion augments lymph transport.
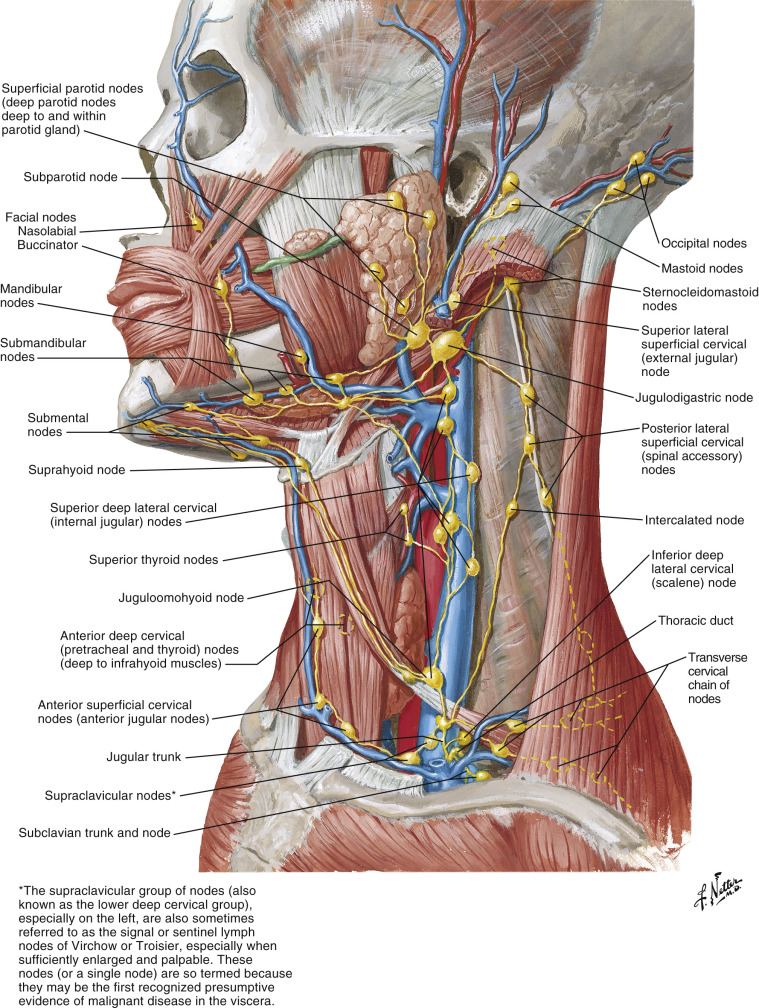
While intestinal lymph is not typically a focus in plastic surgery, it plays a role in certain types of primary lymphedema and is a significant component of lymphatic physiology. Lymphatics in the small intestine are referred to as lacteals, which absorb fats from the intestinal lumen that accumulate to produce the milky-appearing chyle. This lymphatic efflux of fats empties into the cisterna chyli, which is a dilated lymphatic sac that is situated in front of the L1–L2 vertebral bodies. This structure gives rise to the thoracic duct, which drains the majority of the body with the exception of the right upper limb, chest, and head and neck regions, which are drained by the right lymphatic duct. The thoracic duct and right lymphatic duct both terminate in large lymphovenous connections at the junction of the internal jugular vein and subclavian veins ( Fig. 8.1 ). There is, however, significant variability in this anatomy, and major lymphatic ducts can coalesce more superiorly on the internal jugular vein in the region of the supraclavicular lymph nodes. This point is important to note when harvesting a supraclavicular lymph node flap where these structures may be encountered. One might ask, “What would happen if the thoracic duct were ligated?” It is interesting to note that ligation of the thoracic duct is the treatment of choice for refractory chylothorax complicating esophagectomy or other thoracic intervention, yet lymphedema is typically not observed following this procedure. There has only been one report in the literature of lymphedema from the chest to the toes following thoracic duct ligation for idiopathic chylothorax. However, it is unclear whether or not there was a component of preexisting primary lymphedema.
Detailed lymphatic anatomy and drainage of the upper and lower limbs is still an area of continued exploration. However, both cadaveric dissections and indocyanine green lymphangiography (IGL) are providing a more complete picture of the lymphatic system. In the extremities there is a horizontal latticework of lymphatic capillaries in the dermis that drain into “pre-collectors,” which dive deep and empty into superficial lymphatic “collectors” located in the subcutaneous layer. These collectors are easily visualized on IGL and are long vessels mostly along the medial limb, which empty into the local lymph node basin. There are also less numerous lymphatic vessels that are located deep to the deep muscle fascia that travel alongside arteries. The existence of connections between the superficial and deep lymphatic system is still the subject of further investigation. The interaction between the superficial and deep system is a matter of great interest and affects our conceptual framework regarding the role of lymphovenous bypass.
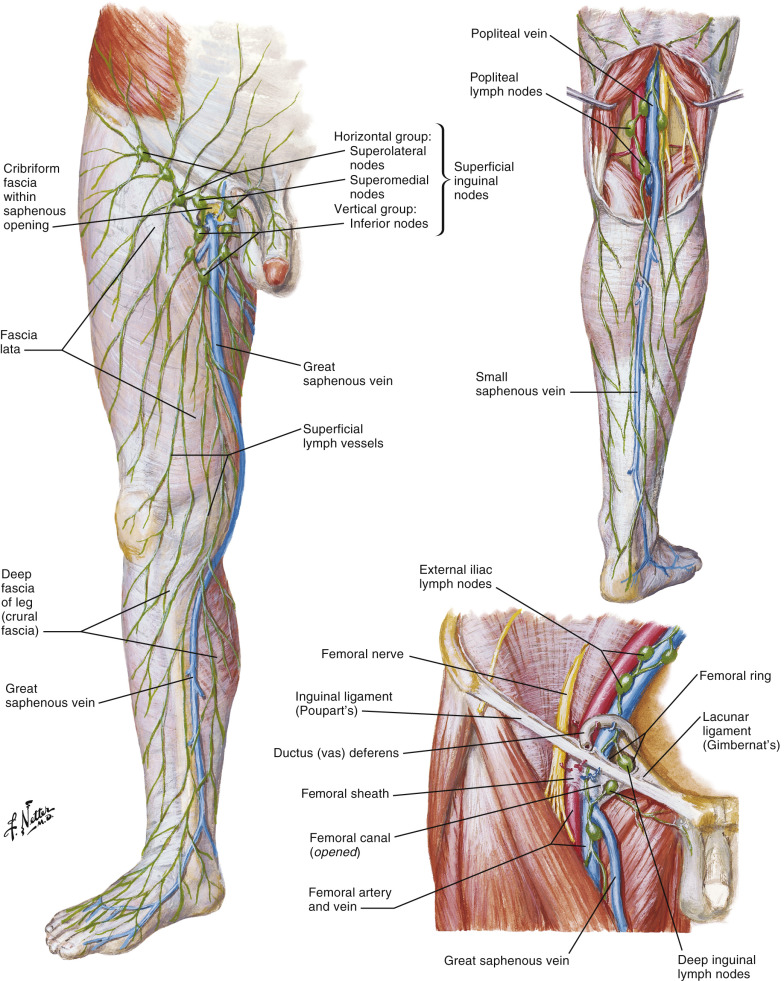
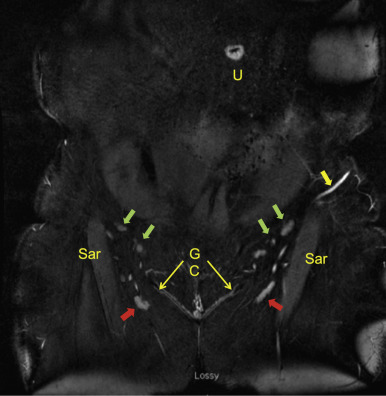
In the lower limb there are lymphatic vessels that travel along the lesser saphenous vein in the posterior leg, which enter the popliteal nodes, but the majority of lymphatic vessels gather around the vicinity of the greater saphenous vein. These collectors continue up the medial thigh, where they encounter one or two sentinel lymph nodes located deep, along the femoral vessels typically several centimeters below the groin crease ( Fig. 8.2 ). These lymph nodes also receive efferent lymphatic vessels from superolaterally oriented lymph nodes that drain the lower abdomen and hips, as well as medially from the superficial layers of the genitalia. Lymphatic traffic then continues medially (medial to the superficial inferior epigastric vein) and deep, along the iliac vessels and ultimately into the thoracic duct. One question previously posed by Tourani and colleagues, was How deep are the superficial collectors? In the medial thigh, where the greater saphenous vein is located deep to the superficial fascial system (analogous to Scarpa’s fascia), the lymphatic collectors were found both superficial and deep to this fascia. This may suggest that even superficial excision of fat in the medial thigh could potentially compromise lymphatic drainage although this has not been formally studied.
Lymphatic drainage of the upper extremity follows a similar motif: most of the superficial lymphatic flow follows the course of the superficial veins and is ultimately funneled into a single large sentinel lymph node in the axilla ( Fig. 8.3 ). Lymphatic drainage then proceeds more proximally into several other smaller lymph nodes. Based on intraoperative study using reverse lymphatic mapping, lymph nodes draining the upper limb are consistently located high in the axilla in proximity to the axillary vein, deep to the pectoralis major muscle, and can also contribute to drainage of the chest. These critical lymph nodes can be supplied by the thoracodorsal artery, lateral thoracic artery, or direct branches from the axillary artery ( Fig. 12.2 ). Alternate lymphatic pathways also exist in the upper limb as lymphatics along the cephalic vein can bypass the axillary nodes and pass through the supraclavicular lymph nodes. An interesting cadaveric study by Suami et al., of a patient who underwent axillary node dissection without clinical lymphedema, illustrates some key differences in normal and abnormal lymphatic drainage. On the affected side, there were incompetent lymphatic valves in the pre-collectors with dermal reflux, and hypertrophy of epitrochlear nodes around the elbow. The superficial lymphatics were obliterated above the elbow but there was a connection between the superficial and deep system that allowed drainage to a few remaining axillary nodes. These detailed anatomic studies and reports are steadily accumulating into a critical body of knowledge for further refinement of lymphatic techniques in the future.
Pathophysiology
Lymphedema has traditionally been thought of as swelling resulting from lymphatic obstruction, but we have come a long way from this concept. Lymphedema most commonly has a delayed presentation following lymphadenectomy, and exhibits behavior of a proliferative disease, as opposed to a simple surgically induced obstruction to lymphatic flow. While the initial insult to the lymphatic system does cause lymphatic impairment and edema, an immune response may ensue, leading not only to destruction of lymphatic vessels but also fat hypertrophy and fibrosis. Central to understanding the progression of lymphedema is the concept that an initially fluid-filled limb progresses into a fibrofatty limb that directly affects surgical decision making and managing patient expectations. This cascade of events is also the subject of investigation into medical therapies that may blunt or reverse this process and could potentially be used as adjuvant therapies to surgery in the future.
Indications for Lymphatic Surgery
Awareness of the spectrum of disease in lymphedema from a fluid-dominant limb to a fibrofatty-dominant limb is important in selecting an appropriate operation for the individual patient. There are two general types of surgery for lymphedema: debulking and physiologic procedures. Debulking techniques do not treat the underlying cause of lymphedema, but are aimed solely at reducing limb volume, essentially treating the fat hypertrophy component of lymphedema. On the other hand, physiologic procedures such as lymphovenous anastomosis (LVA) or vascularized lymph node transfer (VLNT) are aimed at addressing the underlying lymphatic disease process. While these modalities have been effective at reducing the fluid component of lymphedema, the effect on fat hypertrophy has yet to be determined. It also seems that the very best candidates for physiologic procedures are thin patients that have earlier forms of lymphedema with some lymphatic function still intact.
There is a role for all of these procedures, but to provide some context, the goals of the patient and stage of disease become important. A patient with elephantiasis and irreversible skin changes facing potential amputation may be a candidate for a more radical excisional procedure such as the Charles procedure, or one of its more recent iterations. Liposuction is most appropriate for a patient with late-stage lymphedema and a mostly fatty limb confirmed by Brorson’s guidelines: less than a few millimeters of pitting edema after pressing the thumb into the patient’s limb for 1 min at maximal pressure. If this patient is 100% compliant and is willing to wear lifelong compression, sustained volume reduction has been demonstrated over the long term. However, many patients are unable or unwilling to wear constant compression, and do not present with an advanced fibrofatty limb. These fluid-dominant patients may not be good candidates for debulking procedures and this is where physiologic procedures such as LVA and VLNT have played a significant role. There is a host of different microsurgical procedures that have had reported successes, including lympholymphatic anastomosis and lymph node-venous anastomosis. Two approaches that have gained most traction in the microsurgical community have been lymphaticovenular anastomosis and vascularized lymph node transplantation, which will be the focus of this review. This brief passage is in no way meant to exclude other viable procedures, only to highlight a handful of techniques that have become of recent interest and have demonstrated promising results.
Contraindications to Physiologic Procedures
There are many patients who will call the office for lymphedema or swelling of the limbs from one cause or another and it is worthwhile knowing in advance which patients will not be candidates for surgery, particularly physiologic procedures. The two main contraindications we encounter is significant venous disease and obesity. Because a lymph node transfer or LVA relies on lymphovenous shunting, any venous hypertension may compromise this pressure gradient and result in a failed operation. Venous insufficiency is also a very common cause of lower extremity swelling, and treating the venous disease may alleviate some of the swelling. A history of deep vein thrombosis in the affected limb, varicosities, and prior vein surgery are relative contraindications to VLNT or LVA in our practice.
Obesity is another relative contraindication for physiologic lymphatic procedures. Elevated BMI has been shown to impair lymphatic clearance and worsen lymphedema, and is reported to be a risk factor in developing post-mastectomy lymphedema. If a patient were to consider VLNT, obesity may not only compromise efficacy but may also increase the risk for donor site lymphedema and thromboembolic complications. For these reasons, we recommend weight loss to all patients until their BMI is ≤30 before offering physiologic lymphatic surgery.
The Initial Patient Visit
The initial visit focuses on evaluating the patient’s type of lymphedema, their goals, and determining whether a physiologic, debulking, or excisional procedure is appropriate. A focused history includes the status of the venous system, history of deep vein thrombosis or pulmonary embolus, duration of lymphedema, current compression regimen (as a baseline for postoperative comparison), history of cellulitis, radiation, and cancer history. Physical exam includes inspection of the site of the previous cancer to assess for recurrence, and inspection of groin, axillary, and cervical lymph nodes to ensure these potential donor sites do not have pathology. Exam of the affected limb for fibrosis and the presence of pitting quickly provides information about whether the limb is mostly fluid-filled or is already in the advanced stages of fat hypertrophy and fibrosis. Evidence of varicosities, and hemosiderin staining suggest venous disease and may exclude the patient from LVA or VLNT.
On a typical visit, the patient is first evaluated for the possibility of being a candidate for a physiologic procedure such as VLNT or LVA. If the patient has a significant fluid component to their lymphedema evidenced by pitting edema and a good response to compression and elevation, they may be considered for a physiologic procedure. If they have more advanced lymphedema with a mostly fatty limb with no pitting, and are 100% compliant with compression, liposuction may be the best option. Of course there are gray areas with a mixed picture that may benefit from a combination of liposuction and either LVA or VLNT, although the timing of these procedures is still a matter of debate.
On the first visit, every patient should be informed of the risks of VLNT including no improvement, worsening lymphedema, or donor site lymphedema. Donor site lymphedema has been reported, but the quantitative risk of this serious morbidity is unclear because these reports were of VLNT without reverse lymphatic mapping, which has improved the safety of this technique. In our current series of 70 lymph node transfers over the past 5 years, we have not observed donor site lymphedema using the reverse lymphatic mapping (RLM) technique, although we need another 5 years and many more cases to better quantify this risk.
Finally, while VLNT has a clearly established role in secondary lymphedema following oncologic treatment, its use in primary lymphedema is less clear-cut. This is because there is a spectrum of disease within the category of primary lymphedema, with a variety of congenital abnormalities that may all lead to swelling. In our early experience, results were mixed. Becker has suggested that patients with abundant hyperplasic lymphatic vessels seen on magnetic resonance lymphangiography (MRL) could potentially benefit from VLNT, while those with lymphatic vessel hypoplasia are generally avoided, although this is anecdotal observation (Corinne Becker, pers. comm., December 2014). When starting a lymphatic surgery program, there is a greater comfort zone in focusing on cancer-related lymphedema. If a lymph node transfer is considered in primary lymphedema, both four-limb lymphoscintigraphy and IGL are performed to rule out occult impaired lymphatic function near potential donor sites to minimize the risk of causing lymphedema in a patient with an already abnormal lymphatic system.
After discussing risks and benefits, the patient often decides if the risk of surgery outweighs the risk of natural progression of disease. This rules out patients who are on the fence; the best patient is one that is highly motivated for surgery and is not second-guessing their decision. If a patient is interested in surgery, the next step is referral to a certified lymphedema therapist and performing a thorough imaging work-up. Preoperative coordination with a lymphedema therapist is important in ensuring the limb is in optimal condition to promote lymphangiogenesis and to have a seamless postoperative physiotherapy regimen.
Because we are dealing with a poorly understood disease and the role of lymphatic surgery is still evolving, our inclination is to study the patient with as many tools at our disposal as possible, in order to see patterns in disease and hopefully some day predict which of these patterns best responds to a given treatment. This work-up includes magnetic resonance angiography (MRA) of potential donor sites and recipient site; magnetic resonance lymphangiography (MRL) of the affected limb; four-limb lymphoscintigraphy and IGL; perometer for limb volume or an equivalent method; limb impedance measurements; elastometer measurements; and standardized photographs. This list of studies is generally not feasible in many centers, but the most important ones involve some form of MR imaging, and physiologic evaluation of the lymphatic system using lymphoscintigraphy and/or IGL. Interpretation of this work-up involves its own learning curve and close collaboration with nuclear medicine and radiology.
Anatomic Imaging
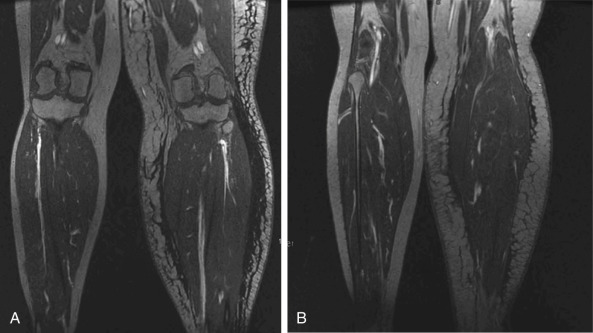
Radiographic imaging includes magnetic resonance angiography (MRA) of both the recipient and potential donor sites. Ablavar contrast, as opposed to gadolinium, is used and stays in the blood for a longer period of time yielding higher resolution. The thin-cut venous phase is used for review. For the recipient site , the fluid versus fat component as well as limb volume can be calculated ( Fig. 8.4 ). Occult recurrence and severe stenosis of the axillary, femoral, or iliac veins following surgery and radiotherapy can also be visualized. If present, venography can better characterize the nature of vein stenosis. We have seen a number of patients with axillary node dissection and radiation with severe axillary vein stenosis requiring extensive lysis to dilate the vein and one patient who required axillary vein reconstruction. As stated earlier, venous hypertension can be a component of limb swelling and could compromise the VLNT or LVA. MRA of the recipient site is performed 1 year postoperatively to confirm viability and quantity of lymph nodes successfully transferred.
MRA of the donor sites allows the surgeon to select the side with the most favorable lymph nodes and vascular anatomy ( Fig. 8.5 ). This is the side with the largest number and size of lymph nodes, positioned farthest away from the lymph nodes that drain the adjacent extremity. For example, if performing an axillary lymph node transfer, the side with the most abundant lymph nodes located farthest from the axillary vein and its adjacent lymph nodes would likely be a safer and more effective choice. If both sides are equivalent, then the side contralateral to the limb with lymphedema is selected, as this is the preference of most lymphedema therapists. This theoretically allows for clearance of the lymph from the affected limb to adjacent lymph node basins, which would preferably not be harvested.
Magnetic resonance lymphangiography (MRL), though not yet widely available, is being increasingly explored, as it can reveal a more complete picture of the lymphatic system and has become Becker’s central mode of work-up. Neligan uses MRL to detect the presence of discreet lymphatic vessels. If there are identifiable lymphatic vessels present, he will perform an LVA, if not, the patient is offered a lymph node transfer.
Functional Imaging
Lymphoscintigraphy
We routinely perform a standardized four-limb lymphoscintigraphy to provide a baseline for both donor and recipient sites. This allows us to determine whether or not the patient has a complete versus partial obstruction, and if complete, what level of obstruction. Ming-Huei Cheng will go straight to performing a VLNT if a complete obstruction is visualized on lymphoscintigraphy. If partial obstruction is visualized, the patient is referred to lymphedema therapy for a trial of conservative treatment (Ming-Huei Cheng, pers. comm., January 2015). This may also determine where to place the lymph nodes in the future, although this is currently under study. One question we are asking is, if the patient has a complete obstruction at the level of the elbow, should we be placing the lymph nodes distally in the wrist or forearm as opposed to the axilla? Comprehensive imaging evaluation and prospective study will answer many of the questions this chapter may prompt. One-year postoperative four-limb lymphoscintigraphy is used to assess both the recipient site and determine if there is any subclinical impaired lymphatic transport at the donor site.
Indocyanine Green Lymphangiography
Indocyanine green lymphangiography (IGL) provides the most detailed view of the superficial lymphatics and allows the surgeon to evaluate lymphatic pumping function. The only limitation is that lymphatics deeper than 5 or 10 mm cannot be visualized with current technology, in comparison with lymphoscintigraphy, which provides a view of the entire lymphatic system but at a much lower resolution, limited to only major lymphatic collectors. All of our patients receive a four-limb IGL preoperatively and at 1 year postoperatively for comparison and evaluation of the recipient and donor sites. IGL appears to be more sensitive at detecting impaired lymphatic function compared with lymphoscintigraphy.
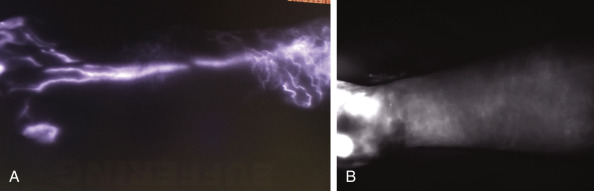
In Koshima’s group, preoperative IGL is used to determine if a patient is likely to respond to LVA (and may also relate to their response with a VLNT). On a histologic level, early-stage lymphedema begins with dilation of obstructed lymphatic vessels, followed by vessel contraction, and ultimately sclerosis. Koshima et al. observed that preoperative IGL findings demonstrating a “linear” pattern with functioning lymphatic vessels correlate with dilated lymphatics intraoperatively, while more advanced findings of dermal reflux on IGL correlate with sclerosed lymphatics. The best outcomes in their experience were in patients with early stage lymphedema, while those with the most advanced level of dermal reflux (“diffuse” pattern) are now seen as poor candidates ( Fig. 8.6 ). Lymph node transplantation is considered in this subset of patients.
Masia contends that sclerosed lymphatics have long lost their smooth muscle peristaltic function, which may render both LVA and VLNT ineffective. There is still discussion as to whether or not passive forces may allow these physiologic procedures to work in LVA and VLNT in the more advanced stages of lymphedema. It seems to be a trend now that earlier intervention, even with VLNT, may lead to a more favorable result. Finally, Chang’s experience with LVA has shown best success with upper extremity lymphedema as opposed to the lower extremity.
In summary, MRA demonstrates the fluid-to-fat ratio very clearly and we can explain more precisely what to expect in terms of volume reduction if the fluid component of the limb is mostly reduced by a physiologic procedure. For example, if 50% of the limb is fat hypertrophy, this patient will never have normalization in limb size with a physiologic procedure alone, and their expectations can be tailored to their scan results. Lymphoscintigraphy and IGL provide a physiologic assessment, and while there are few data to go by at this time, it appears that earlier stage lymphedema with some form of functional lymphatics may respond more favorably to LVA or VLNT. Late stage fat-hypertrophied limbs with no pitting may not respond well and may be better served with liposuction provided constant compression is something the patient will adhere to. Combinations of these two procedures are still being explored at this time. If the patient is a candidate for LVA or VLNT, it is generally in the realm of surgeon preference in terms of which procedure to proceed with. Nonetheless, these imaging studies provide useful information for both patient and surgeon and may present us with keys to improved patient selection in the future.
Lymphaticovenular Anastomosis Versus Vascularized Lymph Node Transfer
Most microsurgeons are now exploring both LVA and VLNT and even combining these techniques – a sign that no single approach has been completely satisfactory. Unfortunately, there are no data comparing these two techniques. One of the major hurdles is that outcomes are difficult to assess in lymphedema. Limb volume or circumference has dominated outcome measures, yet can be easily manipulated postoperatively by aggressive compression and physiotherapy. This has led to skepticism and a broad spectrum of opinion on surgical management.
While there is currently no consensus on which procedure is most appropriate for a given patient, both procedures have shown both success and disappointment, and future study will clarify the indications. Lymph node transfer is conceptually appealing as it replaces the lymph nodes that were removed during surgery, providing not only an exit for lymph but also restoring a major immunologic organ. VLNT does not require specialized instrumentation and applies techniques familiar to all microsurgeons. Most reports demonstrate increased benefit over time, presumably as lymphangiogenesis progresses. However, the potential risk of donor site lymphedema has been the largest barrier to its use. Reverse lymphatic mapping (RLM), described later in this chapter, has addressed this issue in reducing potential morbidity.
On the other hand, one of the most compelling arguments for LVA is that it is minimally invasive, is apparently low-risk, and can be performed under local anesthesia. Limitations of LVA are that it depends on the status of the lymphatic vessels of the patient, it requires specialized instrumentation, and it is technically demanding. Questions regarding the long-term patency and efficacy of the tiny anastomoses have also come into question, although there are long-term successes reported. While many surgeons in the microsurgical community have adopted Koshima’s supermicrosurgical technique of LVA, it is important to note that the term “LVA” is often used interchangeably with Campisi’s technique. Campisi’s vast experience with anastomosis of larger deep lymphatic vessels to larger proximal veins has also shown good results, and is a very different procedure from Koshima’s, which is the subject of the following section.
Lymphaticovenular Anastomosis
Operative Technique
Lymphaticovenular anastomosis was first described by O’Brien and has since been through periods of enthusiasm, skepticism, and now resurgence. Two significant reasons for the renewed popularity is the development of IGL in identifying lymphatics and progress in supermicrosurgical technique and instrumentation. Indocyanine green lymphangiography involves intradermal injection of 0.1 mL of dye into the web spaces of the affected extremity. Using a near-infrared detector, the superficial lymphatics can be visualized and used to map out intact lymphatic vessels. Dark areas, which cross the lymphatics are typically veins that Chang uses as a guide to determine where to make the incisions. Koshima’s group uses a device that detects veins in addition to IGL to plan the incisions in areas where veins and lymphatics are in close proximity. Previous strategies involved injecting blue dye intradermally but the dye cannot be visualized deeply through the skin, and in more advanced cases, is not always taken up by the lymphatics. However, patent blue or Lymphazurin dye is still commonly injected distal to the planned incision to facilitate identification of lymphatic vessels and confirm patency of the anastomosis. The location and number of incisions is still a subject of controversy. Koshima’s group advocates as many anastomoses as possible, pointing out that their results correlate directly with number of bypasses. Others such as Chang, limit the number of anastomoses to only a few at most, with the incision placed at the most proximal terminal end of the visualized patent lymphatic vessel. He will also avoid a major lymphatic collector if it is traversing the entire limb and entering the proximal lymph node basin in a patient with a partial lymphatic obstruction. The concern is that dividing a lymphatic in continuity that is contributing to drainage of the affected limb may actually worsen the lymphedema, although no reports of this have yet surfaced in the literature.
Based on the patient’s anatomy and IGL findings, a series of 2 cm transverse incisions are planned along the medial aspect of the extremity; 1% lidocaine with 1 : 100 000 epinephrine is injected into these markings and the entire procedure can be performed under local anesthesia if desired. The incision and dissection are performed under a high-powered microscope (at greater magnification than an average operating microscope provides) where the target lymphatic vessel(s) and neighboring vein(s) are identified in the subcutaneous layer using superfine instruments.
At this point, a decision is made regarding the various potential anastomotic combinations that can be performed. The goal is to allow for a favorable pressure gradient from the lymphatic system flowing into the venous system. When the vein is divided, ideally there should be minimal to no back bleeding, as excess venous back pressure would prevent lymph from flowing into the vein. The lymphatic vessel does not need to be clamped, but if there is some venous back bleeding, a microvascular clamp is placed proximally on the vein.
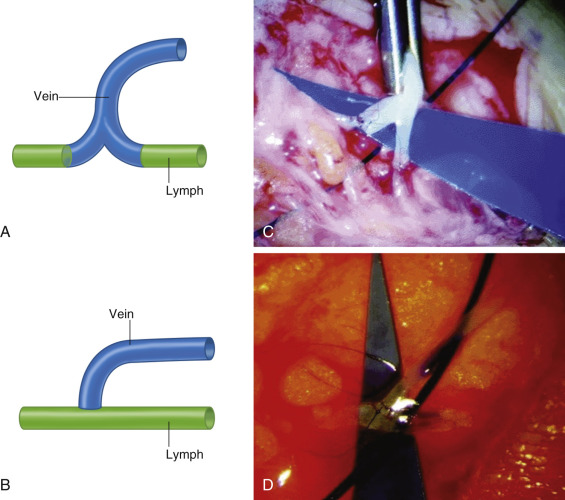
The anastomotic arrangement depends on the number and size of the lymphatics and veins. Koshima has previously illustrated a number of arrangements, the most convenient of which is a lymphatic vessel in proximity to a bifurcated vein. The lymphatic is divided and both the proximal and distal ends are anastomosed to each vein branch, allowing for antegrade venous outflow. If such a configuration is not possible, the second best scenario is a side-to-end arrangement. A window is cut into the sidewall of a lymphatic using a microscissor, and this aperture is then anastomosed to the end of a proximal vein. This allows for bidirectional drainage into the proximal vein. While conceptually appealing, this is also technically challenging. Placing a temporary microvascular clamp proximally on the lymphatic vessel will allow it to dilate to a point where creating the window and performing the anastomosis is more feasible. Using the parachute technique and/or intravascular stenting methods can minimize back-walling these tiny anastomoses. A nylon suture 2/5 the width of the lymphatic vessel, is sharply cut with a blade (and not a scissors, to avoid creating a barb) and is introduced intraluminally into the lymphatic vessel and vein across the planned anastomotic site. This allows for enough room to pass a needle while blocking it from back-walling the vessel. The stent is removed prior to tying the last knot. When the lymphatic vessel is much smaller than the neighboring vein, a variety of alternative arrangements have been used such as a side-to-side anastomosis or the “Pi” arrangement, where the lymphatic is divided and both proximal and distal ends are attached end-to-side to a single larger vein ( Fig. 8.7 ).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


