Introduction
The pectoralis major myocutaneous flap for reconstruction was first described in 1968. Its application in the head and neck region, however, was not reported until Ariyan’s publication in 1979. The reliability and versatility of this flap were subsequently confirmed by many other reports. During the 1980s and early 1990s, before the era of the microvascular free tissue transfer, the pectoralis major myocutaneous flap had been considered as the workhorse reconstruction option following tumor extirpation in the head and neck region. Even in recent years, in institutes where microvascular free tissue transfer is not available, the pectoralis major myocutaneous flap remains to be one of the primary reconstruction options.
Flap Anatomy (see Ch. 11 and Fig 11.1 , Fig 11.2 , Fig 11.3 , Fig 11.5 , Fig 11.8 , Fig 11.9 )
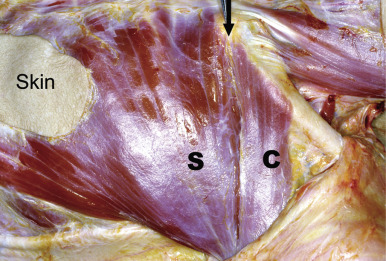
The pectoralis major muscle is a thick, fan-shaped muscle, situated on the upper chest that provides adduction and internal rotation of the arm ( Fig. 34.1 ). It has four sites of origin: first, the anterior surface of the medial half of the clavicle; second, the lateral half of the anterior surface of the manubrium and the sternum extending inferiorly to where the 6th or 7th costal cartilages are attached; third, the costal cartilage from the 2nd to the 6th rib; and fourth, the aponeurosis of the external oblique muscle. From this wide origin, the muscle fibers converge laterally toward the insertion. Those fibers arising from the clavicular portion pass obliquely downward and laterally and are separated from the sternocostal portion by a groove; the fibers from the sternocostal head pass laterally and upward ( Fig. 34.2 ). They join to form a 5 cm flat tendon, which is inserted into the crest of the greater tubercle of the humerus.
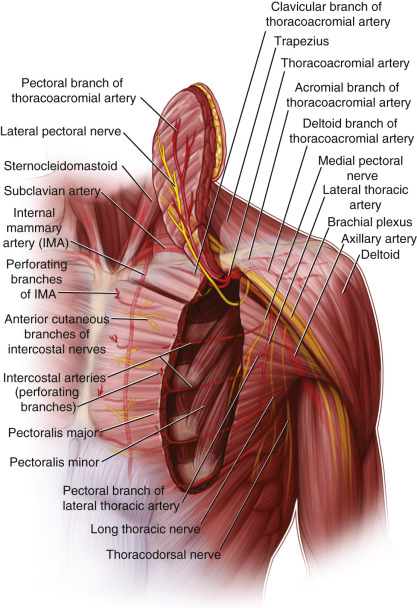
The pectoralis muscle along with its tendon provides the natural look of the anterior axillary fold. The pectoralis minor muscle, which originates on the anterior surface of the 3rd–5th ribs and inserts on the coracoid process of the scapula, lies deep to the pectoralis major muscle. It functions in drawing the scapula downward and forward. The anterior serratus muscle, and the intercostal muscles are present deep to the pectoralis muscles. Superiorly, the pectoralis muscle borders the deltoid muscle. The skin of the anterior chest is pliable and matches that of the face. In females, the breast occupies a large portion of the subcutaneous tissue overlying the pectoralis major muscle.
Arterial Supply of the Flap ( Fig. 34.1 and Fig 11.1 , Fig 11.2 , Fig 11.3 , Fig 11.5 )
The thoracoacromial arterial trunk arises from the second part of the axillary artery and pierces the clavipectoral fascia. It has four branches: acromial, humeral, clavicular, and pectoral.
Dominant to the Clavicular Head:
clavicular branch of the thoracoacromial artery
Length: 1 cm (range 0.5–1.5 cm)
Diameter: 2 mm (range 1.5–2.5 mm)
The clavicular artery is the relatively smaller branch of the thoracoacromial axis. It comes out of the groove between the clavicular and sternocostal heads of the pectoralis major muscle and runs on the undersurface of the clavicular head of the muscle, which it supplies. It also supplies the subclavius muscle and soft tissue around the clavicle.
The clavicular artery is the branch that is most frequently subjected to anatomic variations. From a cadaveric dissection study, 62% of the clavicular arteries arose together with the pectoral and the deltoid branches, forming a trifurcation from the thoracoacromial axis. In the remaining cases, the clavicular arteries might arise from the axillary artery, the thoracoacromial trunk proximal to the main bifurcation, the pectoral artery, the deltoid artery, and the acromial artery.
Dominant to the Sternocostal Head:
pectoral branch of the thoracoacromial artery
Length: 4.5 cm (range 3–5.5 cm)
Diameter: 2 mm (range 1.5–2.5 mm)
The pectoral artery is one of the dominant branches of the thoracoacromial artery. It pierces the clavipectoral fascia medial to the tendon of the pectoralis minor muscle and comes out at the groove between the clavicular and the sternocostal heads of the pectoralis major muscle. It then runs in a cephalocaudal direction on the undersurface of the muscle plastered to it by its fascial envelope. The vessel communicates with the intercostal branches of the internal mammary artery and also the lateral thoracic artery. It gives off muscular branches to supply almost exclusively the sternocostal portion of the muscle, as well as multiple cutaneous perforating arteries to supply virtually the entire ipsilateral chest wall.
Minor:
pectoral branch of the lateral thoracic artery
Length: 3.5 cm (range 3–4 cm)
Diameter: 2 mm (range 1.5–2.5 mm)
The pectoral branch of lateral thoracic artery emerges below the clavicle and pierces the clavipectoral fascia lateral to the tendon of the pectoralis minor muscle, passing along its lateral border for 4–5 cm before running on the undersurface of the pectoralis major muscle, 3–4 cm lateral to the pectoral branch of the thoracoacromial artery. It anastomoses with the internal thoracic, subscapular, intercostal arteries and the pectoral branch of the thoracoacromial artery. In females, the lateral thoracic arteries also give off branches, which pass around the lateral border of the pectoralis major muscle supplying the breast.
Minor Supplying the Sternocostal Portion:
perforating branches of the internal mammary artery (1st to 6th intercostal space)
Length: 1.5 cm (range 1–2 cm)
Diameter: 0.6 (range 0.5–1 mm)
The internal mammary perforating arterial branches pass through the 1st to 6th intercostal spaces to enter the deep surface of the muscle within 1.5–2.0 cm of the sternal margin.
Minor:
perforating branches of the intercostal arteries (5th to 7th)
Length: 1.5 cm (range 1–2 cm)
Diameter: 0.6 (range 0.5–1 mm)
The perforating artery branches of 5th to 7th intercostal arteries pass through the respective intercostal spaces to enter the deep surface of the muscle 4–6 cm from the sternal origin. The row of minor segmental pedicles is located 2–3 cm lateral to the perforators from the internal mammary artery.
The main arterial supply of the pectoralis major muscle is from the branches of the acromio-thoracic arterial trunk. The clavicular branch supplies the clavicular head while the pectoral branch is the dominant arterial supply to the sternocostal head of the pectoralis major muscle. In some female subjects, the lateral thoracic artery can be fairly prominent and may contribute a significant portion of the overall blood supply. All these vessels descend on the undersurface of the pectoralis major muscle. The perforators of the pectoralis major muscle then in turn supply the overlying skin. There are more perforators supplying the skin paddle situated on the lateral aspect of the muscle.
The cutaneous perforators supplying the skin paddle of the flap can be divided into three zones:
- 1.
Laterally, over the lateral aspect/free border of pectoralis major muscle, where numerous large musculocutaneous and direct fasciocutaneous perforators concentrate. Ink injection studies have suggested that skin paddle could be extended safely beyond the muscle towards the axilla, provided the deep fascia is included.
- 2.
Intermediately, over the main bulk of the muscle, where the musculocutaneous perforators are fine and sparse.
- 3.
Medially, at the parasternal region, where the supply is indirect via the “captured” territory of the internal mammary artery perforators. This circulation relies on intact connections between the pectoral branch of the thoracoacromial artery and the internal mammary artery system that exist within the sternocostal head of the pectoralis muscle.
Venous Drainage of the Flap (see Fig. 11.6 )
Primary:
vena comitantes accompanying the arteries
Length: 4.5 cm (range 3–5.5 cm)
Diameter: 2.1 mm (range 0.5–5.0 mm)
The venous drainage of the pectoralis major muscle is located on the undersurface of the muscle. They may form one or two venules and accompany the pectoral branch of the acromio-thoracic arterial trunk. They subsequently drain into the axillary vein. The venous drainage of the overlying skin is toward the subdermal plexus where the vessels join to form venules that subsequently run along the arterial perforators from the pectoralis major muscle.
Secondary:
venules from the periphery of the pectoralis major muscle also drain into the branches of the internal thoracic vein.
The cephalic vein, although drains the skin paddle of the flap, is not included with the flap during harvest.
Flap Innervation
Sensory:
Anterior cutaneous branches of the intercostal nerves (2nd through 7th) ( Figs 34.1 and 11.2 , 11.9 ).
These nerve branches supply the skin over the anterior chest wall.
Motor:
lateral and medial pectoral nerves ( Figs 34.1 and 11.1 , 11.2 ).
The clavicular head of the pectoralis major and the anteromedial part of the sternal head of the muscle are supplied by the lateral pectoral nerve, which originates from the lateral cord of the brachial plexus. It has a constant course running lateral to the axillary artery and then parallel to the thoracoacromial axis. The nerve courses on the deep surface of the pectoralis major muscle for a mean of 55 ± 7 mm, and is visible under the muscle fascia.
The medial pectoral nerve originates from the medial cord of the brachial plexus and supplies the posterolateral parts of the sternal head of the pectoralis major as well as the pectoralis minor muscle. It has a more variable course, but in most cases it travels medial to the axillary artery, piercing and supplying the pectoralis minor muscle at the level of the third intercostal space, at a mean of 10.3 cm from the margin of the sternum. The mean distance between the entry of the medial and lateral pectoral nerves into the pectoralis major muscle is 30.7 ± 10 mm.
Flap Components
In view of the short pedicle, the pectoralis major muscle is considered a less favorable muscle for free tissue transfer compared with other available muscle or myocutaneous flaps.
The pectoralis muscle can be harvested as a pedicled muscle flap or it can be harvested together with an intact skin island on the muscle as a pedicled myocutaneous flap. The latter is the most frequently used modality of the pectoralis flap. The muscle flap may also be harvested attaching to a segment of the costal cartilage or the lateral portion of the anterior cortex of the sternum. When a skin island is included, the former becomes the “costomyocutaneous flap” and the latter, “osteomyocutaneous flap.”
Advantages
- •
The vascular supply of the pectoralis major muscle is in general very constant. It is covered by small amount of soft tissue and is situated clearly among definite tissue planes, making its isolation relatively easy.
- •
The pectoralis major muscle as a pedicled flap is well vascularized and has abundant perforators to supply its overlying skin. Thus this muscle flap alone or as a myocutaneous flap can stand some degree of manipulation and survive under less optimal conditions such as when transferred to an infected or inflamed tissue bed, including the contamination of saliva.
- •
It is located outside the radiation field of the head and neck region, thus provides healthy tissue for reconstruction in an irradiated environment.
- •
The muscle provides adequate tissue bulk for covering important structures in the neck and for filling tissue defects in the chest wall or the neck.
- •
Harvesting of the flap can be performed with the patient in supine position. Thus for most operations in the head and neck region or over the chest wall, the resection and reconstruction can be carried out with the patient in one position.
Disadvantages
- •
Occasionally, the defect that requires coverage is small; the muscle may be too bulky. This is particularly true when a myocutaneous flap is used, as the thick subcutaneous tissue increases the tissue volume. In a female subject, the presence of breast tissue adds further to this bulk.
- •
In a female patient, the harvest of the flap distorts the form of the breast.
- •
Loss of the entire muscle results in a minor functional deficit and loss of the anterior axillary fold, which results in a suboptimal aesthetic appearance.
- •
The length of the pedicle limits the degree of rotation of the flap and the distance that the flap can be transferred to. For head and neck reconstruction, the highest point that it can reach safely is the zygomatic arch. For chest wall reconstruction, it can reach as far as the contralateral anterior axillary line.
- •
Due to its limited pedicle length and availability of other muscle flaps, the role of the pectoralis muscle as a free flap has been minimal.
- •
Several motor branches supply the muscle; therefore, if the flap is to be raised as a functional muscle transfer, all nerves must be coapted in order to attain maximal function.
Preoperative Preparation
All patients should be examined before raising the flap, any scar over the chest wall that might interfere with the design of the flap should be noted, and then the incision for skin island modified accordingly. The presence of the pectoralis major muscle should be checked by asking the patient to tighten the muscle by adduction of the arm. A patient suffering from Poland syndrome has congenital absence of pectoralis major muscle ( Fig. 34.3 ). For these patients, an alternative flap should be used for reconstruction.

For patients with a hairy chest wall, the hair should be removed to expose the skin so that the marking of incision for the skin island and the chest wall incisions can be clearly visualized.
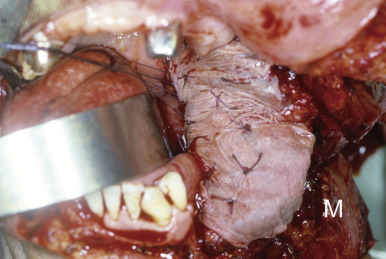
The pectoralis flap can be performed for patients of all ages and in both sexes, although in female patients, the factors of distortion of breast form and the relative thick subcutaneous tissue should be taken into consideration. In obese patients, the excessive thick subcutaneous tissue may make the pectoralis major myocutaneous flap unsuitable for reconstruction of some defects such as intraoral defects or turning the skin paddle into a tube. For intraoral reconstruction, the pectoralis major muscle can be harvested alone and split-thickness skin graft is placed on the muscle to be transposed to the recipient area for reconstruction ( Fig. 34.4 ).
For patients with medical comorbidities such as cardiac or pulmonary diseases, these should be optimized preoperatively, as after harvesting the pectoralis major flap, the chest wound is significant and this might affect the breathing efforts of some patients. This is evidenced by a significant decrease in forced vital capacity in 63.6% of patients after pectoralis major flap harvest. Alternative methods of wound closure, such as skin graft or local transposition flaps, might be considered when donor defects are large, especially in chronic smokers and in those with preexisting cardiopulmonary disease.
Flap Design
Anatomic Landmarks
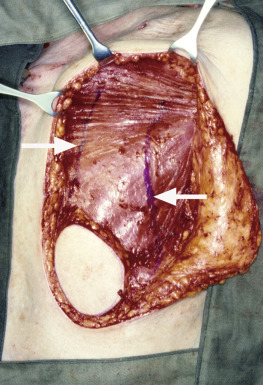
Superiorly, the pectoralis major muscle is attached to the clavicle. Medially the landmark ( Fig. 34.5 ) is the lateral aspect of the anterior surface of the sternum extending inferiorly to the insertion of the 6th costal cartilage. The lateral edge of the muscle can be felt as a ridge extending from the humerus medially and inferiorly to the upper part of the external oblique muscle.
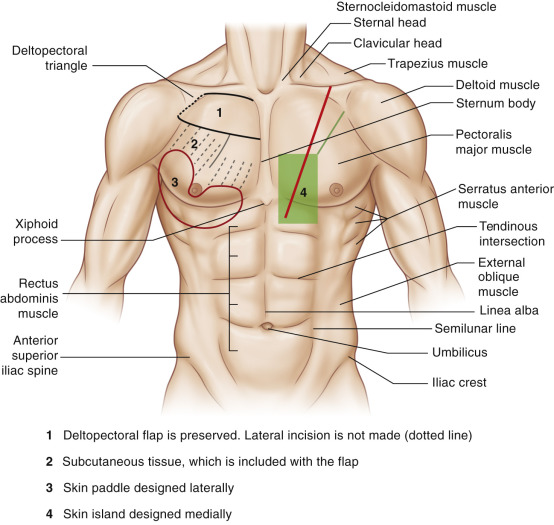
A line drawn between the acromion and the xiphoid cartilage marks the axis of the pedicle of the flap.
General Thoughts About Flap Design
- 1.
Pedicled myocutaneous flap: the skin island should be designed to be placed at the appropriate position on the anterior chest wall so that when the flap is harvested and turned, it will reach the defect without tension. The lower the skin island is situated, the higher it will reach in the head and neck region. To ensure survival of the entire skin island, the whole area of the skin island should be situated on the pectoralis major muscle. If possible, the skin island should be designed to lie on the lateral aspect of the muscle where there are more perforators, particularly when the skin paddle is small. The reliable lower limit of the skin island size is 5 cm by 7 cm situated medial to the nipple. The size of the skin island can be smaller when it is placed lateral to the nipple. There may be a role for preoperative localization of the vessels and the perforators using Doppler ultrasound studies, particularly when a small skin paddle is used in order to make sure that it contains at least one sizeable perforator.
- 2.
Pedicled costomyocutaneous flap: the 5th costal cartilage is identified during the design of the skin flap and marked. This will avoid inadvertently detaching the pectoralis muscle origin from the costal cartilage while harvesting the flap.
- 3.
Pedicled osteomyocutaneous flap: the outer cortex of the sternum should be marked at the design of the skin flap. On harvesting the flap, the periosteum and outer cortex of the sternum should be lifted together with the pectoralis major muscle.
Special Considerations
The pectoralis major muscle is composed of the clavicular and sternocostal heads. After harvesting the myocutaneous flap, the whole pectoralis major muscle together with the skin paddle is turned upward to the head and neck region. The muscle lying over the clavicle will produce a prominent bulge. The bulkiness of the flap at this point has disadvantages; the swelling besides being unsightly, although with time it will atrophy, limits the mobility of the pedicle. The vessels running on the muscle bulk may be stretched when the muscle swells in the early postoperative period. The muscle bulge also reduces the distance the flap can reach superiorly ( Fig. 34.6 ).
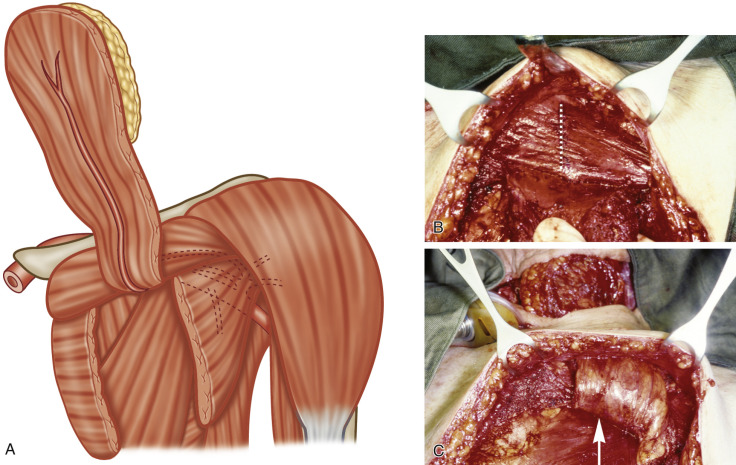
This can be avoided when only the sternocostal head of the pectoralis major is used to carry the skin island and turned upward to the head and neck region. As blood supply of the clavicular and the sternocostal heads are separate, the two heads can be separated by dissecting along the groove between the two heads. The origin of the pectoral branch as the pedicle of the flap can be identified in the groove and preserved on the deep surface of the sternocostal head. The clavicular head can be divided along the axis of the pedicle and the muscle fibers will retract, producing a triangular gap in the muscle to allow the positioning of the pedicle of the flap when turned upward to the head and neck area ( Fig. 34.7 ).
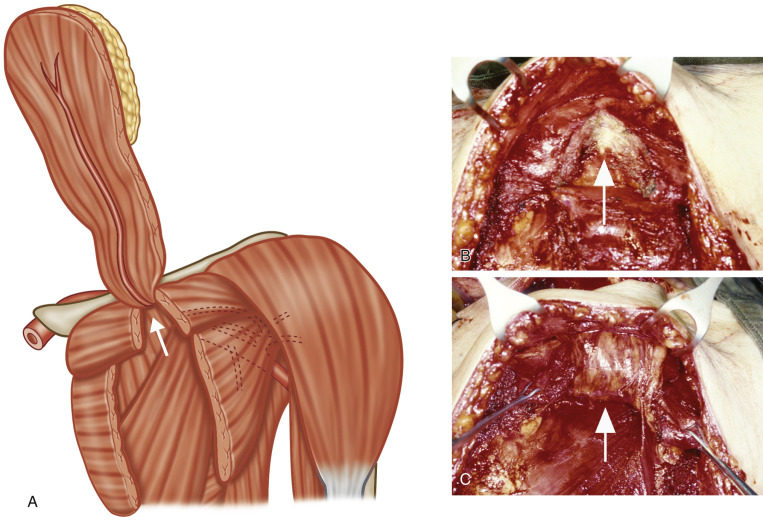
With the elimination of the muscle bulk formed by the clavicular head, the stretching of the pedicle is reduced and the length of the pedicle is also increased by 4–6 cm. The mobility of the myocutaneous flap is also enhanced, so that the tension exerted at the skin paddle is reduced.
In general, the bulk of the pectoralis major is its main disadvantage. Thus, while lifting the muscle, only the portion of the muscle that carries the skin island is required to be harvested and is included as the myocutaneous flap ( Fig. 34.8 ).
The skin island should be designed according to the shape of the defect that it aims to reconstruct. The skin island usually shrinks about 10% after skin incision. The dimension of shrinkage is more in young patients, and adjustments in designing the flap should take this into consideration.
To extend the length of the flap, the skin island may be placed more distally maintaining some subcutaneous tissue over a large part of the muscle more proximally. This helps to maintain a better venous drainage of the flap ( Fig. 34.5 ).
Difference in Design, if Any, When Performing the Flap as Pedicled or Free
The design is the same for a free and pedicled flap. If a longer pedicle is required, the skin island can be designed over the most distal part of muscle.
Flap Dimensions
Muscle Dimensions
Length: Average 15 cm (range 12–22 cm)
Width: Average 24 cm (range 21–26 cm)
Thickness: Average 1 cm (range 0.8–1.4 cm)
Skin Island Dimensions
Length: Average 12 cm (range 7–30 cm), maximum to close primarily 8 cm
Width: Average 8 cm (range 5–20 cm), maximum to close primarily 10 cm
Thickness: Average 1.4 cm (range 0.6–2.5 cm)
The location for easiest closure is where the skin paddle is placed laterally along the natural skin crease.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


