■ Level 6 is also known as the central neck and includes the lymph nodes medial to the carotid sheath on each side and bounded by the hyoid bone superiorly and the sternum inferiorly.
■ Levels 1 through 5 are also known as the lateral neck and include all of the node compartments lateral to the carotid sheath on each side.
PATIENT HISTORY AND PHYSICAL FINDINGS
■ Thyroid cancer lymph node metastases can be palpable or, more often, nonpalpable but identifiable by imaging. Very small foci of thyroid cancer in lymph nodes may only be evident at microscopic pathology examination.
IMAGING AND OTHER DIAGNOSTIC STUDIES
■ Patients with thyroid cancer should each have a staging ultrasound examination prior to operation.1 This allows mapping of the lymph node status of each compartment in the neck (FIG 2).
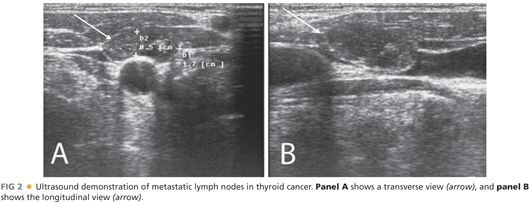
■ The level 6 lymph nodes are the most difficult to evaluate by ultrasound when the thyroid gland is still present, as these structures are in the same compartment.
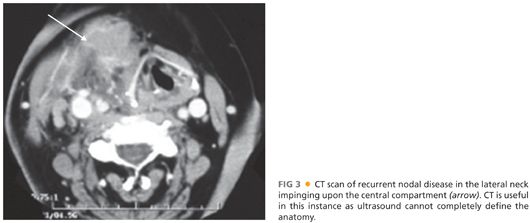
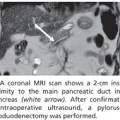
■ Patients with large tumors or gross adenopathy may be best studied by computed tomography (CT) scan with contrast or magnetic resonance scanning, as these modalities allow better examination of the areas low in the neck that may be obscured by gross disease on ultrasound (FIG 3).
SURGICAL MANAGEMENT
■ Dissection of the level 6 lymph nodes is generally performed in conjunction with total thyroidectomy.
■ The level 6 lymph nodes are removed by clearing the soft tissue that surrounds the thyroid gland. No additional incision or mobilization is necessary.
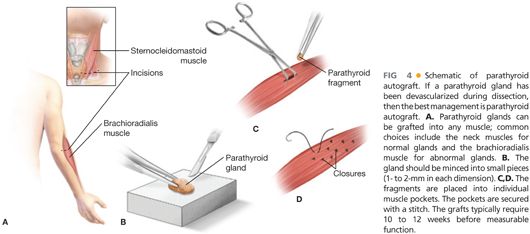
■ Clearing these level 6 nodes involves additional manipulation of the soft tissue and vascular supply that surrounds the parathyroid glands. With these glands at additional risk of being damaged during operation, the performance of parathyroid autograft is particularly important to avoid permanent hypoparathyroidism2 (FIG 4).
Preoperative Planning
■ Review of the preoperative ultrasound findings is critical to the proper inclusion of all suspicious lymph nodes.
■ Especially in reoperations, ultrasound in the operating room after the induction of anesthesia and positioning can be helpful to localize small lymph nodes.
■ A nerve stimulating and monitoring system can be helpful and is commonly used to identify and to test function of motor nerves during dissection. Testing of the vagus nerve is probably best accomplished by using a specialized nerve stimulator that includes electromyography (EMG) monitoring pads on the endotracheal tube to detect vocalis muscle contraction. Testing of motor nerves for which the enervated muscle is visible can be done with a simple nerve stimulator.
Positioning
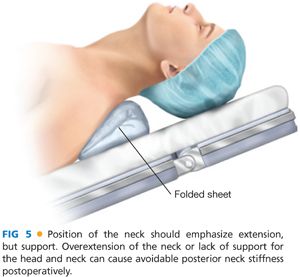
■ The patient should be supine and the head may be raised above the heart to decrease venous congestion in the neck (FIG 5).
■ Airway management is of particular concern. Preoperative anesthesiology consultation should alleviate positioning concerns while ensuring proper airway safety during the procedure.
■
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


