Lower Posterior Torso and Buttock Sculpting
Dennis J. Hurwitz
DEFINITION
Harmonious sculpturing of a feminine lower back, waist, and buttocks is a new frontier in body contouring surgery. Because less attention has been focused on these regions than the breasts and abdomen, many plastic surgeons need training in advanced approaches to achieve femininity of the lower posterior torso.
Although the public is increasingly requesting buttock enlargement, adjacent areas such as the flanks, hips, and lateral and posterior thighs should be also addressed when performing buttock augmentation. As there is minimal demand for augmentation of the male buttocks, the male situation will receive limited attention.
A summary of this author’s approach follows:
Back rolls with undersized buttocks are treated by thirdgeneration ultrasound-assisted lipoplasty of the torso with lipotransfer to the buttocks in the young overweight female.
Posterior torso tissue laxity with flank rolls and buttock ptosis is the indication for lower body lift with de-epithelialized adipose fascial flap buttock augmentation. Liposuction harvest of fat from the flanks and abdomen followed by fat transfer to the inferior buttocks may be helpful to complete the lower torso buttock reshaping.
Maximum narrowing of the waist in the older female, especially when none ever existed and the most effective safe correction of oversized love handles in all males is achieved with direct oblique excision of the flanks, ie, a oblique flankplasty.
Silicone elastomer implants are reserved for buttock augmentation when harvestable fat stores are inadequate.
The drawbacks of commonly accepted approaches have limited their use in favor of innovative solutions to be presented in this chapter.
Traditional liposuction is rather traumatic when applied to the fibrous posterior torso.
Hip-hugging circumferential lower body lifts with and without adipose fascial flaps for gluteal buttock augmentation often sag along the lateral gluteal region and fail to narrow bulging waists.
ANATOMY
A sensuous woman’s lower posterior torso, upper thigh, and buttocks and the procedures to create them are based anatomically (see FIG 1 for an artistic rendering of role of underlying anatomy to feminine shape). The photographic results of the four case presentations of this chapter approximate aesthetic ideal.
A subtle feminine S-shaped curvilinear midline is centered on the curving lumbar spine. Along with its paraspinous muscular ridges, this concavity bridges the convexities of the lower thoracic spine and sacrum.
A tapering lower thoracic rib cage narrows to the pelvic brim. This gap is spanned by the latissimus dorsi and external oblique muscles with overlying adipose.
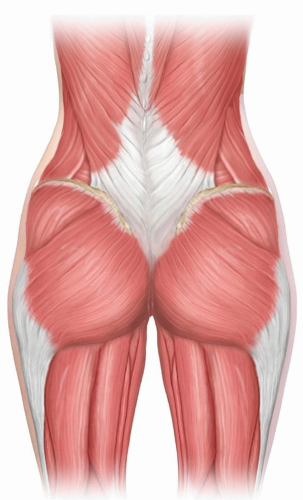
FIG 1 • Anatomy relationships in the aesthetic lower back and buttocks. The musculoskeletal structure and relationships are responsible for the underlying shape of the lower back, waist, and buttocks. Adipose fullness about the hips and buttocks accentuates femininity. The paramedian vascularity clearly nurtures advanced buttock flaps.
At an ideal 0.7 transverse diameter, waist-to-buttocks ratio, the waist abruptly expands laterally over the posterior iliac spines to adipose rounded hips that are wider than her shoulders.1
The maximal projection of the midbuttocks combines adiposity with the gluteus maximus muscle bulk and lies directly on a horizontal plane to the mons pubis.
Buttock projection abruptly extends from back lordosis.
From their widest diameter, lateral buttocks smoothly taper to slightly convex upper lateral thighs.
Posterior medially, the curved buttocks abruptly end in horizontal folds about the ischial tuberosity to border the upper posterior thighs.
Within those essential features, there are a variety of sensually pleasing sizes and shapes, but overall, the ideal 0.7 ratio of waist-to-buttock transverse diameter holds true.
Preserved generous paramedian perforating blood supply allows for high-tension closures and limited mobilization of adipose fascial flaps for buttock augmentation.
Android body build, massive weight gain and loss, aging, and lower body lifts may result in masculinization and/or undesirable contours.
Reducing of the curvilinear midline features
Dampening of lumbar lordosis
The lower back and waist undulating concavities are straightened and may even bulge.
Increased breadth of the back and waist dominates over the narrowing buttocks.
Lateral buttocks are flattened and even depressed.
Inferior buttock fold separations from the posterior thighs are obliterated.
NATURAL HISTORY
The shape of the posterior torso and buttocks can be distorted by congenitally flared posterior costal margins, wide and high pelvic rims, localized flank adiposity, weight gain, weight loss, pregnancy, and menopause.
Most commonly, aging with weight gain broadens the midtorso, deposits, and transverse rolls and narrows and flattens the buttocks. Buttock ptosis may obliterate the fold at the medial posterior thighs and leave sagging, wrinkled skin.
Once acquired, increased girth of the flanks is hard to lose through exercise and weight loss, and narrow buttocks rarely expand.
PATIENT HISTORY AND PHYSICAL FINDINGS
For the back and buttocks, women usually request elimination of sagging back rolls and filling flat buttocks. On occasion, they specifically mention a smaller back, a narrower waist with smooth contours bridging the lower chest and buttocks, and rounder buttocks. More commonly, they complain of sagging abdomen and/or breasts.
They either ignore the back, waist, or buttocks or simply feel that little can be done to improve bulging or masculine features. Because of that, women considering breast reshaping or abdominoplasty should have their posterior torso, thighs, and buttocks examined. If those areas are sensually alluring, she should be complimented.
As a rule, in all but morbidly obese patients or after extreme weight loss, the central back is feminine and need no correction. Her figure faults are presented, and if there is interest, the means for their correction are offered.
In Western Pennsylvania and probably throughout most of America, candidates for body contouring of the back and waist rarely request improvement. Instead, they inquire about breast reshaping and are pleased to learn that the lateral breast roll and upper back can be reduced.
They request a tummy tuck and are pleased to learn that their waist can be reduced by liposuction or direct excision. A deep and defined waist with rounded buttocks during youth suggests fertility, which is an aphrodisiac.
With buttock augmentation requests, patients are pleased to learn that fat removed from around the buttocks not only can be processed to augment it but also the perimeter reduction can picture frame buttock prominence. Because their companions better see the posterior view, they tend to be enthusiastic about the anticipated improvement. For some, a lower body lift is the best approach to suspend the thighs and buttocks.
The examination while standing exposes the entire aesthetic complex.
Overall and localized excess adiposity and skin laxity are noted.
Tightly bound skin expanded by underlying fat is noted as the contour can be improved by liposuction with the expectation of reasonable skin retraction.
Hanging tissues and rolls are described by location (lateral breast, scapular, midback, flanks, and hips) and magnitude.
Back rolls are characterized by transverse accumulations of adiposity within loose skin bordered inferiorly by transverse dense fibrous adherence from the dermis to the underlying muscular fascia through relatively thin subcutaneous fat.
Ptotic rolls, in most over 50 years of age, are best treated with direct or superior excisions.
Sagging and flat buttocks are congenital, age related, or the aftermath of severe weight loss.
Laxity with lateral flattening and even indentation are common with aging.
While pointing out figure faults in front of a full-length mirror aids communication, reviewing standardized digital images is usually less awkward. In either case, lines can be drawn that indicate proposed excisions, liposuction or lipoaugmentation, and resulting scars.
IMAGING
There are no supportive radiologic or other diagnostic studies.
NONOPERATIVE MANAGEMENT
If the posterior torso and buttocks are obese, then a weight loss program is indicated.
There are a variety of noninvasive treatments that apply energy to cause lysis of adipose for reduced volume. Topical treatments of proven but limited and somewhat variable reduced shaping are CoolSculpt, Thermage, VelaShape, Liposonix, and VASER Shape.
They are intended to reduce small selected areas over repeated and rather painful treatments. Large contour adipose excess is difficult to reduce.
The appeal is nonsurgery and minimal to no downtime.
Smartlipo with YAG laser energy leads the list of recognized minimally invasive adipose lysis with some skin retraction, but this costly technology has not been widely embraced among plastic surgeons.
Recently, minimally invasive treatments with subcutaneous thin probes delivering controlled radiofrequency energy, Thermi and InMode BodyTite, have shown consistent lipolysis with some shrinkage of the lower torso.
SURGICAL MANAGEMENT
Indications
Patient recognizes correctable deformity of the lower posterior torso and buttocks.
Patient is reasonable in goals and accepts the therapeutic recommendations and risks.
Patient is in good health with control of chronic disease.
Preoperative Planning
Medical, mental, and psychological conditions must be evaluated and acceptable for elective surgery.
The roles of liposuction, fat grafting, tissue excision, adipose fascial flaps, and silicone implants toward reaching their aesthetic goals
The functional working order of all equipment with special attention to high-technology instrumentation
An awareness of the areas to be liposuctioned, lipoaugmented, and excised and the resulting scars
The trade-off of scars for unwanted contour deformities
Understanding of the unpredictable quality of scars and the likelihood of faded scars over many years
The planned areas for liposuction and incisions for skin and fat excisions are drawn on the awake patient either the evening before or immediately prior to the operation.
Patient understands the unpredictable magnitude of fat graft take.
Patient understands the risks of implant malposition, exposure, and infection.
Immediately prior to the procedure, the tissues are pushed together to simulate closures. Excessive width of resection is avoided. When closures are planned over buried adipose fascial flaps, the width of resection is appropriately reduced.
Following neighboring liposuction and flap undermining, manual assurance of the proper width of resection is made during the operation for the final time with the plan to tangentially resect more tissue if needed to obtain mild tension at closure.
Positioning
Surgery only on the posterior trunk is performed with the patient prone. The table is airplane towards lateral for deep liposuction of the flanks.
When an abdominoplasty is part of the plan and fat harvest in the prone position is estimated inadequate for the buttock augmentation, then the operation starts supine with the lipoabdominoplasty followed by a turn prone with strategic placement of gel body rolls to obtain a jack-knife position.
Approach
Some combination of the following advanced techniques are considered:
VASERlipo with optimal probe, mode, power, and cannula selections for extraction and harvesting of fat
Lower body lift with adipose fascial flap augmentation
Direct oblique excision of flank excess selectively replaces lower body lift.
Silicone soft elastomer gluteal implant augmentation
TECHNIQUES
▪ VASERlipo of the Posterior Torso With Lipoaugmentation of the Buttocks (Video 1)
The demand for gluteal fat augmentation has increased in recent years, with 9993 reported procedures in 2013 and 11 505 in 2014 in the United States.
VASERlipo is best indicated for flatten buttocks with mild to moderate torso adipose deposits in a previously well-shaped young woman (TECH FIG 1A-D).
The 1 year result of 3500-cc VASERlipo and 300 cc of lipofill of each lateral buttock reveals more pleasing feminine contours (TECH FIG 1E-H).
Markings
Through visual and palpable cues, bulging and moderately ptotic back rolls are mapped with purple marker from one to three pluses for the extent of adiposity to be removed via liposuction.
Excessive removal or etching is indicated in black. Depressed areas, such as adherences, should be avoided and are marked in red. Inadequate and depressed buttock projection is encircled with green marker with dashes indicating the extent of deficiency.
Power-Assisted Lipoplasty
The densely fibrous adipose of the posterior torso makes traditional suction-assisted liposuction (SAL) arduous and traumatic. Popular power-assisted lipoplasty (PAL) reduces the surgeon’s effort but not the damage to the retained tissue.
Excessive disruption of the connective tissue and neurovasculature intensifies the trauma and disrupts tissue elasticity.
With large volume removal, the patients are traumatized and intrinsic skin contraction damaged. Recovery can be prolonged for weeks.
Nevertheless, traditional liposuction and PAL are the most common means of fat shaping and the results can be dramatically excellent.
Fat Emulsification and Harvest
VASER provides for the preliminary application of internal focused ultrasound. VASER is the acronym for Vibration Amplification of Sound Energy at Resonance.
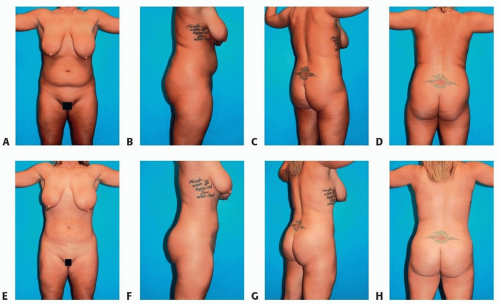
TECH FIG 1 • A-D. Preoperative frontal, right lateral, right posterior oblique, and posterior view presentation for 4400 cc VASERlipo of the torso, followed by 330-cc lipoaugmentation of each buttock. A 33-year-old woman desires a smaller, more sensual body with buttock roundness. E-H. One-year postoperative result of VASERlipo of the torso with lateral lipoaugmentation of the buttocks.
Resonance is a natural phenomenon referring to the possibility to amplify up to nine times the input resonance versus the energy released. The use of ultrasound frequencies at resonance means that the energy release is most efficient, translating to less power needed to create the same effect, resulting in reduced adverse effects.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








