Local Flaps for Partial Mastectomy Defects
Moustapha Hamdi
Ibrahim Al Bassam
History
Perforator flaps have been described and used since the mid-1990s. Harvesting a flap without any muscle sacrifice as well as sparing the functional motor nerves to the underlying muscle has expanded the horizons of reconstructive breast surgery, minimizing donor-site morbidity (1).
There are two basic types of surgical techniques in partial breast reconstruction: volume displacement and volume replacement techniques (2). Volume displacement techniques with the concept of breast tissue rearrangement will be described more in details in another chapter. Volume replacement techniques are used in small to moderate-sized breasts or when the tumor/breast ratio is large and the residual breast tissue is insufficient for the reshaping and the replacement of the defect. Volume replacement is performed with nonbreast local or distant flaps offering both tissue for the filling of the glandular defect and the skin deficiency of the reconstructed breast. The use of local flaps as a volume replacement technique are the main focus of this chapter.
Local perforator flaps are commonly utilized in our department for partial breast reconstruction. The thoracodorsal (TD) and intercostal (IC) arteries provide many perforators to the area adjacent to the breast with minimum donor-site morbidity, unlike the latissimus dorsi (LD) muscle or musculocutaneous flap which has an increased risk for donor-site morbidity (1).
Indications
Patients often require surgery after partial mastectomy to correct volume discrepancy, contour deformity, and nipple malposition (3). The resection of more than 15% to 20% of the breast parenchyma in a small-volume (A or B cup) breast and more than 30% in larger breast will result in volumetric deformities and bilateral asymmetries (Fig. 35-1). Patients with small or nonptotic breasts could require volume replacement. In addition,
radiotherapy distorts the shape of the breast, initially causing breast edema and skin erythema and eventually causing parenchymal fibrosis, retraction, skin atrophy, hyper/hypopigmentation, and telangiectasia. The long-term results of radiation are unpredictable but usually stabilize 1 to 3 years after radiation (4). In these patients, partial breast reconstruction with flaps could be considered as an important part of whole breast cancer treatment.
radiotherapy distorts the shape of the breast, initially causing breast edema and skin erythema and eventually causing parenchymal fibrosis, retraction, skin atrophy, hyper/hypopigmentation, and telangiectasia. The long-term results of radiation are unpredictable but usually stabilize 1 to 3 years after radiation (4). In these patients, partial breast reconstruction with flaps could be considered as an important part of whole breast cancer treatment.
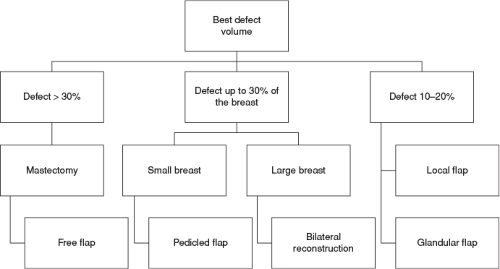 FIGURE 35-1 Partial breast reconstruction: a decision-making process. |
 FIGURE 35-2 Indications of partial breast reconstruction flaps. |
The main indication for pedicled flaps is immediate or delayed partial breast reconstruction when volume replacement is necessary. However, these flaps can be utilized as a salvage procedure after partial/total previous free flap loss for breast reconstruction or as soft tissue coverage of the thoracic area after radical excision. Moreover, these flaps can be combined with implants in breast reconstruction as well when reconstructing larger-volume breasts (Fig. 35-2).
Contraindications
Perforator flaps are considered very meticulous surgeries that require sufficient training in microsurgery; lack of adequate training would be a contraindication to perform such procedure. As local pedicled flaps these flaps have limitation when it comes to the site of the defect and it will be difficult to reconstruct inferomedial defects of the breast with such flaps. Planning partial breast reconstruction for large breasts or larger defects with these local flaps won’t give sufficient volume for the reconstruction.
Previous axillary or thoracic surgery with damage to the TD vessels is a contraindication for LD flap or thoracodorsal artery perforator (TDAP) flap but these patients may still be candidates for a lateral intercostal artery perforator (LICAP) flap. Previous scars and irradiation to the area may be considered as relative contraindications of local pedicled perforator flaps as they also might result in damaging the perforator complex (1). In the end, when breast deformity after partial mastectomy and radiotherapy is severe, the optimal choice is to perform a complete mastectomy and autologous reconstruction with a free flap transfer.
Preoperative Planning
Preoperative evaluation of the patient must be standardized and detailed. Any previous breast surgery should be taken into account. Different body types, skin laxity, and fat distribution are important factors in the decision-making process. Breast physical examination must include the evaluation of breast skin elasticity and thickness, scars, and any defining marks such as tattoos, stretch marks, and contour irregularities. Breast shape, grade of ptosis, and size are determinants of success in surgical treatment. The base and width of the breast, the width of the nipple areolar complex (NAC), the height of the nipple, and the distance from the sternal notch, midline, and inframammary fold (IMF) must be documented in detail. Any natural breast asymmetry should be pointed out to the patient before surgery. Furthermore, palpation for masses or abnormalities in the breast parenchyma, nipple examination, and detailed documentation of breast sensation are mandatory.
In planning the approach to treat the partial mastectomy defect, the primary decision that must be made is whether reconstructive surgery will be needed after the tumor excision. Poor cosmetic outcomes after partial mastectomies can occur from both the amount of breast tissue removed and/or the site of the cancer. Partial breast reconstruction with flaps depends on the size of the tumor, its anatomical location, the need for skin excision, and the amount of tissue resection required to achieve free margins in relation to the volume of the breast.
When volume replacement is necessary, the decision of which technique will be used is determined mostly by the surgeon’s experience, the location of the tumor,
and the size of the defect in relation to the size of the remaining breast. The nonbreast locoregional flaps offer extra tissue required in large tumor excisions/quadrantectomies for the replacement of the breast volume, however they can be more demanding procedures and associated with donor-site and flap morbidity. Small lateral defects can be easily repaired with skin rotation flaps or lateral thoracic axial flaps. However, most of these fasciocutaneous flaps may be unavailable in patients who have had axillary lymph node dissection. The LD muscle or musculocutaneous flaps have been very popular as a method of choice in partial breast reconstruction (4). On the other hand, local pedicled perforator flaps have allowed surgeons to replace large defects with the minimum donor-site morbidity. Fasciocutaneous perforator flaps offer sufficient soft tissue coverage while sparing the muscle and tend to have a lower seroma rate.
and the size of the defect in relation to the size of the remaining breast. The nonbreast locoregional flaps offer extra tissue required in large tumor excisions/quadrantectomies for the replacement of the breast volume, however they can be more demanding procedures and associated with donor-site and flap morbidity. Small lateral defects can be easily repaired with skin rotation flaps or lateral thoracic axial flaps. However, most of these fasciocutaneous flaps may be unavailable in patients who have had axillary lymph node dissection. The LD muscle or musculocutaneous flaps have been very popular as a method of choice in partial breast reconstruction (4). On the other hand, local pedicled perforator flaps have allowed surgeons to replace large defects with the minimum donor-site morbidity. Fasciocutaneous perforator flaps offer sufficient soft tissue coverage while sparing the muscle and tend to have a lower seroma rate.
Relevant Surgical Anatomy
Both breast and plastic surgeons must have a thorough understanding of breast anatomy, physiology, and the standards of aesthetically pleasing breast shape. Oncoplastic surgeons should consider the aesthetic breast subunits when planning both cosmetic quadrantectomies and reconstructions (Table 35-1) (4,5).
The Latissimus Dorsi Flap
The LD flap has the advantage of having a constant anatomy (6). The blood supply of the LD comes from the TD artery, a terminal branch of the subscapular artery. The subscapular artery runs about 5 cm before splitting into the scapular circumflex and the TD arteries. The TD artery is about 2 to 4 mm in diameter and it courses along the posterior axillary fold for about 8 to 14 cm before piercing the LD on its costal surface. The TD artery gives off one or two branches to the serratus anterior muscle and one branch to the overlying skin. The basic pattern of the TD bundle (artery, nerve, and one to two venae comitantes) branches into a lateral (vertical) and a medial (horizontal) branch. The lateral branch follows a course parallel to the muscle fibers, 1 to 4 cm medial to the free lateral border of the muscle and gives off perforating vessels that supply the skin. The smaller medial branch diverges at an angle of 45 degrees and travels medially. There are perforating vessels from the IC and lumbar arteries which supply the muscle and overlying skin as well (6).
TABLE 35-1 Aesthetic Subunits of the Breast | |||
|---|---|---|---|
|
The TDAP Flap
The TDAP flap is based on the perforators from the descending (vertical) or horizontal branches of the TD vessels. Anatomic studies on cadavers showed the presence of two to three musculocutaneous perforators from the vertical branch. The proximal perforator enters in the subcutaneous plane obliquely 8 to 10 cm below the axillary fold and 2 to 3 cm posterior to the lateral border of the muscle. The second perforator is located 2 to 4 cm distally to the first one. Occasionally, a direct cutaneous perforator arising from the TD vessel passes around the lateral border of the muscle, making flap harvesting easier.
Due to anatomical variations, there may not be always a single reliable perforator for the TDAP flap (7). In this case the surgeon must be aware and be prepared to modify the flap dissection intraoperatively into a muscle-sparing LD flap.
Related posts:
 Patient Selection for Breast-Conservation Therapy
Patient Selection for Breast-Conservation Therapy
 Oncoplastic Approach to Maximizing the Lumpectomy-Level I
Postneoadjuvant Axillary Assessment and Management
Oncoplastic Approach to Maximizing the Lumpectomy-Level I
Postneoadjuvant Axillary Assessment and Management
 Selection of Vascularized Lymph Node Donor Sites for Upper Extremity Lymphedema Surgery and Strategies to Minimizing Complications
Selection of Vascularized Lymph Node Donor Sites for Upper Extremity Lymphedema Surgery and Strategies to Minimizing Complications
 Avoiding Pitfalls in Symmetry Procedures Following Unilateral Autologous Versus Implant-Based Reconstruction
Avoiding Pitfalls in Symmetry Procedures Following Unilateral Autologous Versus Implant-Based Reconstruction
 Breast Reduction and Mastopexy After Massive Weight Loss
Breast Reduction and Mastopexy After Massive Weight Loss
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


