Oncoplastic Approach to Maximizing the Lumpectomy-Level I
Pamela Li
Jill R. Dietz
The role of breast conservation, partial mastectomy with adjuvant radiation, in the surgical management of breast cancer has shown equivalent disease-free and overall survival to that of mastectomy with improved aesthetic outcomes, quality of life, and patient satisfaction (1). There are however limitations to breast conservation. For breast conservation to be successful, adequate negative surgical margins need to be achieved with a cosmetically acceptable result. In some instances, the extent of tissue that needs to be excised might compromise the resulting breast cosmesis. In this circumstance, a patient would be offered mastectomy.
Many patients still desire breast conservation, even when a large volume resection of tissue is required. Additionally, given the importance of patient appearance and satisfaction after treatment, there has been a drive to improve cosmetic outcomes after breast cancer surgery and treatment. With this came the development of oncoplastic breast surgery.
Goals and Benefits of Oncoplastic Breast Surgery
The primary goal of oncoplastic breast surgery is to optimize oncologic and cosmetic outcomes of breast conservation. Oncoplastic breast surgery allows for large cancer resections with reshaping of the breast performed during the same operation. Because of this, oncoplastic surgery facilitates partial mastectomy, especially in the setting of more extensive resections in patients who previously would be offered mastectomy. Oncoplastic surgery has been shown to reduce mastectomy and reexcision rates with improved cosmetic results and increased patient satisfaction (2). Because the cancer resection and reconstruction are performed during the same surgery, it avoids a subsequent surgery to repair a cosmetic deformity. Partial mastectomy also requires less recovery time and decreased surgical morbidity when compared to mastectomy.
Level I Versus Level II Oncoplastic Techniques
There are a wide variety of techniques and procedures used in oncoplastic breast surgery. These can be more broadly divided into two categories: level I versus level II procedures (3). They are categorized based on the volume of tissue excised and the degree of complexity necessary to reshape the breast mound. Level I procedures involve resection of less than 20% of the breast volume; these are the focus of this chapter. Level I techniques include glandular flaps that can be advanced or rotated to fill the lumpectomy cavity. Level II procedures are more complex. These include resection of more than 20% of the breast volume and the reconstruction of the breast usually involves mammoplasty techniques. Level II procedures often also involve excision of skin and are sometimes performed in conjunction with a plastic surgeon. Glandular density should also be considered in choosing the optimal oncoplastic techniques. When the breast tissue is fattier in composition, level II techniques will often provide a superior cosmetic result. When level large tumor resections are performed without level II techniques, the cosmetic result can be compromised (Fig. 9-1).
Performing Level I Oncoplastic Surgery
Preoperative Evaluation
All patients undergoing a breast cancer surgery should be considered a candidate for oncoplastic surgery. The assessment begins at the initial surgical consultation. Pertinent patient history includes complicating medical conditions, prior radiation, and smoking history. Physical examination should assess breast size, breast shape, degree of breast ptosis, and skin quality. Prior incisions
should also be noted. Patient discussion should include their aesthetic desires and goals with regard to breast size and shape.
should also be noted. Patient discussion should include their aesthetic desires and goals with regard to breast size and shape.
 FIGURE 9-1 Aesthetically placed incision but resection volume greater than 20%. Level II procedure would improve cosmetic outcome. |
Multidisciplinary evaluation of preoperative imaging between the surgeon and the radiologist helps to determine the location of the resection, the volume of tissue to be excised, and the overall glandular density of the breast. These factors help to determine the type of oncoplastic surgery to perform. Nonpalpable lesions are often excised with image-guided localization techniques such as wire localization, various types of seed localization, or ultrasound-guided excision. For those practices using wire localization, optimal localization approach can be discussed preoperatively.
Patient photographs are also a valuable aspect of preoperative planning and documentation. Photographs require informed consent. Photography consent can be included in a standard consent to treat or as a separate consent when photographs are taken.
Operative Markings for Surgical Planning
Performing preoperative marking is necessary in performing successful oncoplastic breast surgery (4). Markings should be performed with the patient standing in the normal anatomical position. Initial fixed anatomic landmarks to be marked include the sternal notch, the midline, the clavicles, and the inframammary crease. The nipple meridian is a line that starts at a point on the clavicle approximately 6 cm from the sternal notch and extends to the center of the nipple. This line divides the breast in half. The final nipple position should be along the nipple meridian. Pitanguy point is identified by placing your fingers behind the breast at the inframammary ridge and marking the point on the skin. The nipple should ideally be placed at this point so if there is significant ptosis, then an oncoplastic level II procedure might yield a better cosmetic result. See Figure 9-2.
Intraoperative Surgical Steps for Performing General Level I Procedures
Though there are many different level I procedures, the general components of performing these procedures are similar. Clough et al. describes six steps to performing all level I oncoplastic surgery procedures (3).
Step 1: Optimizing Incision Location
Oncoplastic surgery does not emphasize minimizing the incision length. It does prioritize incision location. The choice of incision/technique can be guided based on tumor location. The location of the incision needs to allow for good operative exposure, wide excision of the cancer, and extensive mobilization of the neighboring tissue to allow for reshaping of the breast. Upper pole
tumors can be approached with crescent, batwing, or hemi-batwing incisions. Many lower pole lesions can be accessed through an inframammary incision. An axillary incision can be used for lesions in the upper outer quadrant. Circumareolar or donut mastopexy incisions can be used to access multiple areas of the breast (see Fig. 9-3). All of these approaches will be discussed in more detail in this chapter.
tumors can be approached with crescent, batwing, or hemi-batwing incisions. Many lower pole lesions can be accessed through an inframammary incision. An axillary incision can be used for lesions in the upper outer quadrant. Circumareolar or donut mastopexy incisions can be used to access multiple areas of the breast (see Fig. 9-3). All of these approaches will be discussed in more detail in this chapter.
 FIGURE 9-2 Sternal notch, xiphoid process, inframammary ridge, breast meridian are marked with the patient standing. Pitanguy point is marked by identifying the inframammary ridge projected through the breast. |
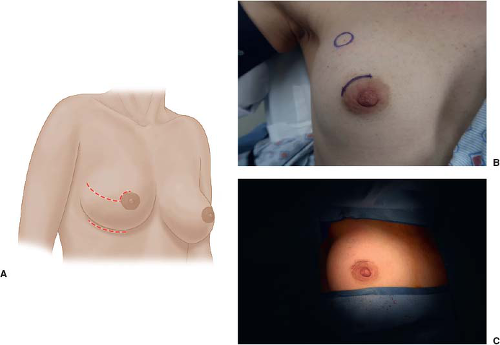 FIGURE 9-3 A: Schematic well-placed incision. B: Fibroadenoma in upper outer quadrant. C: Closed circumareolar incision with hidden scar. |
Step 2: Undermining of Skin
Skin undermining is a key component to performing level I oncoplastic surgery. The skin should be undermined in the mastectomy plane beyond the lesion to be excised. This will aid in both exposure for lesion excision and for the reapproximation of glandular breast tissue (see Fig. 9-4). Consideration of breast density and other risk factors such as current/recent tobacco use or diabetes are necessary to reduce the risk of fat necrosis with extensive undermining. Fatty density breast tissue carries a higher risk of fat necrosis limiting options with level I techniques. Fat necrosis can lead to infection and wound complications with subsequent cosmetic deformity.
Related posts:
 Patient Selection for Breast-Conservation Therapy
Patient Selection for Breast-Conservation Therapy
 The Surgical Management of Locally Advanced and Stage IV Breast Cancer
The Surgical Management of Locally Advanced and Stage IV Breast Cancer
 Alternative Methods for Axillary Sentinel Lymph Node Dissection
Alternative Methods for Axillary Sentinel Lymph Node Dissection
 Optimizing Mastectomy Flaps Based on Breast Anatomy
Optimizing Mastectomy Flaps Based on Breast Anatomy
 Liposuction as a Viable Treatment for End-Stage Upper Extremity Lymphedema
Liposuction as a Viable Treatment for End-Stage Upper Extremity Lymphedema
 Oncoplastic Techniques in Breast Conservation Therapy—The Plastic Surgeon’s Perspective
Oncoplastic Techniques in Breast Conservation Therapy—The Plastic Surgeon’s Perspective
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


