5 Local Anesthetics and Common Nerve Blocks Abstract A considerable number of plastic surgery procedures are done under local anesthesia with or without sedation; hence knowledge of their mechanism of action, dosages, and potential complications is of utmost relevance. Local anesthetics (LAs) block nerve conduction by binding to a modulated receptor located on the interior of the sodium channel, which prevents the increase in membrane permeability to sodium ions that would normally lead to a nerve impulse. The more potent and longer-acting LAs are more lipid soluble and show increased protein binding and less systemic absorption, but at the expense of having a higher potential for systemic toxicity. Even though systemic toxicity from LAs is an uncommon occurrence, when it occurs it should be managed promptly and effectively with supportive measures and intravenous (IV) administration of 20% lipid emulsion. LAs are used for field or regional blocks. Regional blocks supply anesthesia to a large territory with a comparatively small quantity of LA, avoiding the complications of general anesthesia and the systemic toxicity of large volumes of LA. Regional blocks in the face and limbs can be performed easily and effectively for a number of different procedures, such as wound closure, skin cancer excision and flap reconstruction, and nerve entrapment syndromes. This chapter describes the main aspects of the physiology of LAs and their use in the clinical setting, along with a technical description of the main blocks used in plastic surgery. Keywords: local anesthetics, maximum dose, regional block, sedation, toxicity The first local anesthetic (LA), cocaine, was isolated from leaves of the coca plant in 1860. The medicinal use of coca was first investigated and described by Freud in 1884. Koller, an Austrian ophthalmologist, introduced the use of cocaine as a topical anesthetic for ophthalmologic procedures, and subsequently the clinical application of cocaine became widespread. The development of organic chemistry enabled the synthesis of procaine, another ester LA, analogue of cocaine, in 1905. In the 1940s lidocaine, the first amide LA, was introduced with fewer undesirable effects and deeper anesthesia than procaine. Bupivacaine was synthesized in 1957 with a longer duration of action. Levobupivacaine and ropivacaine were later introduced to reduce cardiac toxicity. LAs block the generation and propagation of electrical impulses in nerves and other electrically excitable tissue. The nerve’s action potential must be reduced by at least 50% before measurable loss of function is observed. Generation of action potentials primarily results from the activation of voltage-gated sodium channels (v-gSCs), the key target of LA activity. These channels are protein structures spanning the bilayer lipid membrane composed of structural elements, an aqueous pore, and voltage-sensing elements that control passage of ions through the pore. LAs act on the v-gSCs by modification of the lipid membrane surrounding them and by direct interaction with their protein structure. Binding sites to LAs are located on the intracellular side of the v-gSCs and possess stereoselectivity with preference for the R isomers, although S isomers have nearly equal efficacy with less potential for systemic toxicity. Depending on p Ka and environmental pH, LAs exist both as a lipid-soluble neutral form and as a hydrophilic charged form, with the ionized cationic form being clearly more potent. LAs must penetrate the lipid-rich nerve sheaths and cell membrane in order to reach the v-gSC. The binding site of LAs is located inside the channel pore and is not readily reachable from the extracellular side; therefore, in order to reach their binding site, LAs must first reach the intracellular space by crossing the nerve’s membrane and diffusing through the lipid bilayer. Consequently, the potency of each LA is closely related to its lipid solubility and is dependent on pH. Most LAs have pKa values slightly higher than physiologic pH. Alkalinization by addition of sodium bicarbonate to LA solutions increases their pH and shifts the equilibrium in favor of the neutral base forms, which facilitates translocation of the LA into the cytoplasm. Nerve fibers show differences in susceptibility to LA blockade based on size, myelination, and length of fiber exposed to LA. In addition, a differential pattern of sensory block after application of LA to a peripheral nerve is observed. Temperature sensation is lost first, followed by sharp pain, and finally light touch. The quality of nerve blockade is determined not only by the potency of the individual LA but also by its concentration and volume. The latter is important because a sufficient length of axon must be blocked in order to prevent regeneration of the impulse in the adjacent node of Ranvier. The onset of action of LAs depends on the route of administration and dosage (e.g., concentration). In peripheral nerve blocks (PNBs) where LA is injected in the vicinity of the target nerve(s), the amount of drug that reaches such nerve(s) will depend on diffusion of the drug and the proximity of injection. For a given route of administration, increasing the concentration can accelerate onset. The duration of action of LAs is determined primarily by their protein binding. LAs with a high affinity for protein remain bound to the nerve membrane for longer periods of time. In other words, the higher the affinity for Na+ channels binding, the longer the duration of the LA. Furthermore, duration of action is also influenced by the rate of vascular uptake of LA from the injection site. All currently available LAs consist of a lipophilic phenyl ring and a hydrophobic tertiary amine. In general, with increasing length of the carbon backbone of the tertiary amine, LAs exhibit greater lipid solubility, protein binding, potency, and duration of action. Based on the type of chemical bond, amide or ester, linking the phenyl ring with the tertiary amine, LAs are classified as amino-amides (articaine, bupivacaine, lidocaine, prilocaine, ropivacaine) or amino-esters (cocaine, chloroprocaine, procaine, tetracaine). Amide and ester LAs differ in their chemical stability, metabolism, and allergic potential. Amides are extremely stable, whereas esters are relatively unstable, particularly in neutral or alkaline solution. Amide compounds undergo enzymatic degradation in the liver, whereas ester compounds are hydrolyzed by plasmatic esterase enzymes. The metabolites of esters include p-aminobenzoic acid (PABA), which can occasionally induce allergic reactions. Allergies to amides are very rare. Based on their chiral form, LAs are classified as single enantiomers or racemic mixtures. Enantiomers consist of two stereoisomers (left/sinister/S or right/dexter/R) that are mirror images of each other with respect to a specific chiral center. A racemic mixture contains equal amounts of the two enantiomers. The two forms possess different pharmacological properties that are of clinical importance. All currently available LAs are racemic mixtures, with the exception of lidocaine (achiral), levobupivacaine (S), and ropivacaine (S). Levobupivacaine’s potency and efficacy are comparable to those of bupivacaine, but it has significantly less cardiac and central nervous system (CNS) toxicity, likely due to reduced affinity for subtypes of Na+ channels expressed in brain and cardiac tissues. The time to resolution of PNBs is extremely variable for different blocks, and between patients, even when all block-related factors are equal. When patients are discharged from the operating area or from the hospital prior to complete resolution of the block, precautions should be taken to avoid injury to an insensitive limb and falls. Equipment such as slings, protective padding, and crutches may be needed. The duration of PNBs of short-acting agents, such as procaine and chloroprocaine, ranges from 30 to 60 minutes, whereas long-acting agents, such as bupivacaine and tetracaine, may remain active for nearly 10 hours. The rate of vascular uptake significantly affects LA duration of action because LAs can exert their anesthetic effect only as long as they remain at the site of deposition. Vasoconstriction slows the rate of vascular absorption and thus prolongs the duration of action. For this purpose, vasoconstrictive agents, such as epinephrine, are frequently added to LAs to increase duration. The prolongation of nerve block with vasoconstrictors is more prominent with LAs of intermediate duration, such as lidocaine and prilocaine, than with longer-acting agents, such as bupivacaine, possibly because the effect of long-acting LAs outlasts that of vasoconstrictors. Caution Getting the dose right Local anesthetic concentration is expressed in percentage, so that 1% solution = 1 g of anesthetic in 100 mL of sol ution = 10 mg/mL Hence, if the maximum recommended dose of, for example, lidocaine is 300 mg, then 30 mL of 1% solution would be the maximum to administer. Toxicity of LAs is the limiting factor in their clinical use. LAs are relatively safe if administered appropriately; however, significant systemic or localized toxicity can result from unintended intravascular or intraneural injection or if excessive doses are administered resulting in major systemic absorption. When epinephrine is added to LAs, intravascular injection will result in tachycardia and hypertension, which are useful signs that inadvertent intravascular injection has occurred. Rapid uptake of LA injected into a vascular area may also lead to systemic toxicity, which generally occurs immediately, but may become apparent > 10 minutes after injection. Systemic toxicity manifests primarily in the cardiovascular and central nervous systems. The signs and symptoms of LA toxicity range from mild symptoms (ringing in the ears, metallic taste, tingling of the lips, and agitation) to severe neurologic (seizures) and cardiovascular signs (hypertension, hypotension, tachycardia, bradycardia, ventricular arrhythmias, and cardiac arrest). The effect of LAs on the cardiovascular system is dual: by directly affecting cardiac myocytes and peripheral vascular smooth muscle cells, and indirectly by their action on the autonomic nervous system. The more potent, lipophilic LAs, such as bupivacaine, tetracaine, and etidocaine, are more cardiotoxic than the less lipophilic agents, such as procaine, prilocaine, and lidocaine LAs readily cross the blood–brain barrier and generalized CNS toxicity may occur from systemic absorption or direct vascular injection. LAs’ potential for generalized CNS toxicity approximately parallels their action potential blocking potency. Signs of generalized CNS toxicity are dose dependent, with low doses producing CNS depression, and higher doses resulting in CNS excitation and seizures. Increasing doses of LAs produce light-headedness, tinnitus, and tongue numbness, before the appearance of seizures, unconsciousness, and ultimately respiratory arrest and cardiovascular depression with heart arrest. Treatment of LA systemic toxicity consists of IV administration of 20% lipid emulsion (1.5 mL/kg bolus, followed by 0.25 mL/kg/min infusion), together with supportive airway and hemodynamic management. Calcium channel blockers and β-blockers should be avoided; vasopressin is not recommended and initial doses of epinephrine should be small (10–100 µg IV). If there is no clinical improvement after 30 minutes, the bolus dose of lipid emulsion 1.5 mL/kg should be repeated and the continuous infusion increased to 0.5 mL/kg/min. Most adverse reactions to LAs are nonallergic and include psychomotor responses related to anxiety, sympathetic stimulation from pain or epinephrine, or toxic effects attributable to heightened sensitivity to known properties of the drug. However, two different types of allergic reactions have been described: allergic contact dermatitis and urticaria–anaphylaxis. Allergic contact dermatitis (type IV hypersensitivity) produces delayed swelling at the site of injection within 72 hours. Urticaria, anaphylaxis, and immediate allergic reactions (type I hypersensitivity), which typically begin within 1 hour of drug administration, are described in only a handful of case reports. Patients with suspected allergic reactions to LAs should be evaluated because most can tolerate other LA agents. An approach to safely precluding these reactions includes skin testing and controlled drug challenge. Peripheral nerve injury is rare with PNBs. Related symptoms are transient, lasting days to months. Major complications resulting in permanent (> 6 months) nerve damage range between 0.015 and 0.09%. Most nerve injuries are believed to occur secondary to intraneural injection, which can be minimized if injection is halted and the needle withdrawn if undue resistance to injection is encountered or if the patient feels sharp pain or paresthesias. Additional risk factors for nerve injury include preexisting nerve pathology (including diabetes) and the use of standard longer-beveled needles. Symptoms of nerve injury are primarily sensory (pain, tingling, or paresthesia), though they may include a combination of motor and sensory deficits depending on the nerve involved and the severity of injury. Most symptoms resolve within 6 months; if symptoms are either severe or persistent, the patient should be referred to a neurologist. Inadvertent puncture of nearby vascular structures can lead to perineural hematoma. It is prudent to avoid performing PNBs in patients with an abnormal coagulation status in anatomical locations in which application of pressure to the puncture site is not possible. The vast majority of hematomas can be controlled by directly pressing on the puncture site; rarely, surgical decompression may be required. Although many drugs have been added to LAs with the aim of decreasing onset time, increasing duration, increasing block density, or decreasing toxicity, they are not universally used because their side effects are felt to outweigh their benefits. The limited available evidence regarding potential adjuvants includes epinephrine, sodium bicarbonate, fentanyl, dexamethasone, and α2-agonists. Epinephrine is the most common vasoconstrictor added to PNBs, typically at a concentration of 1:200,000 to 1:400,000. It is used both to indicate rapid vascular uptake (e.g., during inadvertent intravascular injection an increase in heart rate of ≥ 20 bpm and/or an increase in systolic blood pressure ≥ 15 mm Hg after a dose of 15 µg of epinephrine should raise a suspicion of intravascular injection) and to decrease the LA’s absorption, which may in turn reduce potential toxicity (in vascular areas) and prolong duration of the block. Side effects of epinephrine include tachycardia and a potential for ischemia to nerves and other tissues due to vasoconstriction. Consequently, in patients at risk of cardiac ischemia or those with possibly decreased perineural blood flow (e.g., postchemotherapy, diabetes, or vascular disease), it is reasonable to use lower concentrations (1:400,000). Sodium bicarbonate is used to reduce onset time of the LA effect. The quicker onset is most evident in LAs with commercially added epinephrine—which are formulated at a lower pH—but is often not of clinical significance. The addition of fentanyl or morphine to PNBs does not provide a clear clinical benefit. The addition of dexamethasone to LAs in PNBs was associated with longer duration of action in several trials. The addition of clonidine to LA for PNB prolongs the duration of sensory and motor blockade, albeit at the expense of a higher risk of hypotension, bradycardia, and sedation. Benzodiazepines (BDZs) enhance the effect of the neurotransmitter γ-aminobutyric acid (GABA) at the GABAA receptor, resulting in sedative, hypnotic, anxiolytic, anticonvulsant, and muscle relaxant properties. Used as systemic adjuvants to PNB, BDZs reduce anxiety and improve patient cooperation. According to their half-life, BDZs are categorized as short (midazolam, tetrazepam, or triazolam), intermediate (alprazolam, chlordiazepoxide, lorazepam, or lormetazepam), or long-acting (bromazepam, clonazepam, clorazepate, diazepam, or flunitrazepam). BDZs are safe and effective for short-term use, although cognitive impairment and paradoxical effects, such as agitation, panic, aggression, or behavioral disinhibition occasionally occur. Low doses of short or intermediate BDZs are best titrated to optimize sedative effects. BDZ overdose produces CNS depression with impaired balance, ataxia, and slurred speech. Severe symptoms include coma and respiratory depression. Supportive care is the mainstay of treatment of BDZ overdose. There is an antidote, flumazenil, which can be used to reverse excessive sedation of BDZs. Regional nerve blocks provide anesthesia to a relatively large territory with small volumes of LA, thus avoiding potential complications of general anesthesia and the systemic toxicity associated with the administration of large volumes of LA. In addition, nerve blocks minimize patient discomfort, allowing a number of different procedures, such as local flaps in the face and limbs, debridement and suture of complex wounds, injection of botulinum toxin and limb surgery, with fast recovery. Herein we will describe the anatomy of cutaneous innervation of the face, scalp, ear, hand and wrist, and ankle and foot, followed by the technique of blocking the main nerves supplying these areas. The trigeminal nerve carries sensory information from the face through its three major branches: the ophthalmic nerve (V1), the maxillary nerve (V2), and the mandibular nerve (V3) ( To successfully anesthetize their different territories, the nerves supplying the face should be located at the points where they exit the skull, which corresponds roughly with a mid-pupillary line going from the forehead to the mandible ( The frontal nerve, a branch of the ophthalmic nerve, divides into the supraorbital and supratrochlear nerves. The former emerges from the supraorbital notch, whereas the latter exits the skull at a point just lateral to the bridge of the nose. Together these nerves supply the forehead and parietal scalp. To block these nerves, the supraorbital notch is first identified by palpation, and the needle is inserted pointing medially, injecting 2–3 mL of anesthetic. The needle is then advanced parallel to the brow toward the glabella, where another 2 mL are injected. Finally, the whole area is gently massaged to evenly distribute the anesthetic and favor its penetration into the nerve. If the glabellar area or the bridge or dorsum of the nose is not adequately numbed, then the infratrochlear nerve can be blocked by injecting 0.5 mL of LA at the junction of the nose with the medial canthus of the eye.
5.1 Introduction
5.2 Basic Science
5.3 Classification of Local Anesthetics
5.4 Pharmacology
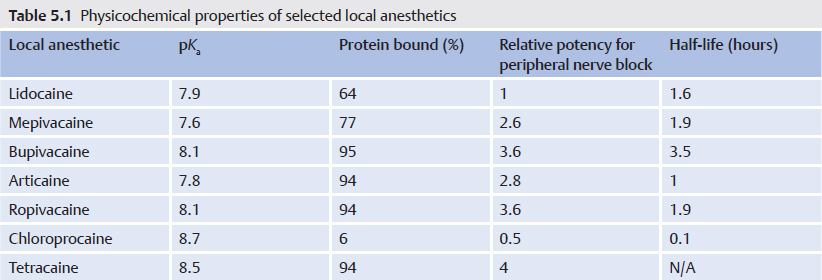
![]() Table 5.1 and
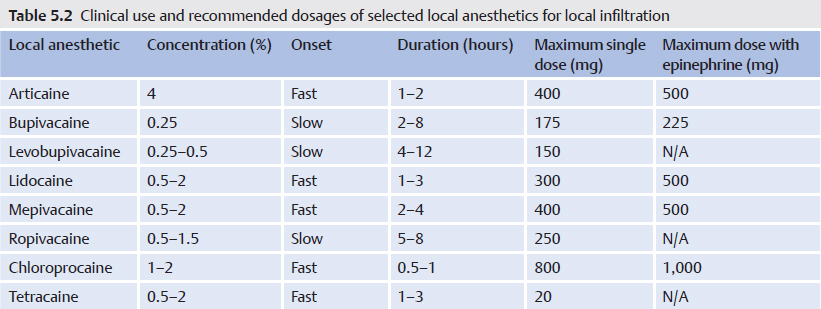
Table 5.1 and ![]() Table 5.2 give an overview of the physicochemical properties, clinical use, and dosing of each agent. Recommended maximum doses given here relate to normal conditions (e.g., healthy individual weighing 70 kg). However, the dose must be tailored individually, depending on body weight and the patient’s condition; reduced clearance of LAs associated with renal, hepatic, and cardiac diseases is the most important reason for lowering the dose of anesthetic in repeated or continuous administrations. Recommended maximum doses are orientative and do not constitute an absolute maximum dose because they are not evidence based. Furthermore, recommended maximum doses may vary according to injection technique, injection site (e.g., regions of high absorption), or single versus protracted injection. The common occurrence of CNS toxicity symptoms following infiltration of large volumes of lidocaine led to the recommendation of just 200 mg as the maximum dose. Epinephrine in concentrations of 2.5 to 5 µg/mL should be added to the LA solution when large doses are required, provided that there are no contraindications for the use of epinephrine.
Table 5.2 give an overview of the physicochemical properties, clinical use, and dosing of each agent. Recommended maximum doses given here relate to normal conditions (e.g., healthy individual weighing 70 kg). However, the dose must be tailored individually, depending on body weight and the patient’s condition; reduced clearance of LAs associated with renal, hepatic, and cardiac diseases is the most important reason for lowering the dose of anesthetic in repeated or continuous administrations. Recommended maximum doses are orientative and do not constitute an absolute maximum dose because they are not evidence based. Furthermore, recommended maximum doses may vary according to injection technique, injection site (e.g., regions of high absorption), or single versus protracted injection. The common occurrence of CNS toxicity symptoms following infiltration of large volumes of lidocaine led to the recommendation of just 200 mg as the maximum dose. Epinephrine in concentrations of 2.5 to 5 µg/mL should be added to the LA solution when large doses are required, provided that there are no contraindications for the use of epinephrine.

5.5 Toxicity and Complications of Local Anesthetics
5.6 Allergic Reactions
5.6.1 Nerve Injury
5.6.2 Hematoma
5.7 Adjuvants
5.7.1 Benzodiazepines
5.8 Essential Regional Blocks for Plastic Surgery
5.8.1 Face
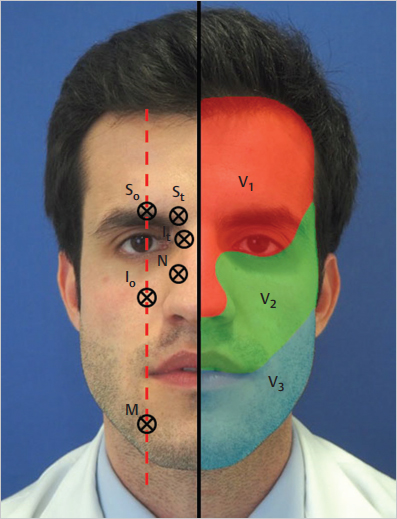
![]() Fig. 5.1). Whereas V1 and V2 are purely sensitive, V3 also carries motor axons that control muscles involved in biting and swallowing. The terminal branches of these nerves, namely supraorbital, supratrochlear (V1), infraorbital (V2), and mental nerve (V3), innervate the face and part of the scalp.
Fig. 5.1). Whereas V1 and V2 are purely sensitive, V3 also carries motor axons that control muscles involved in biting and swallowing. The terminal branches of these nerves, namely supraorbital, supratrochlear (V1), infraorbital (V2), and mental nerve (V3), innervate the face and part of the scalp.
![]() Fig. 5.1). In general, only 2–3 mL of LA are enough to anesthetize a given territory, always remembering to inject in the vicinity of the nerve and aspirate first to prevent intravascular injection.
Fig. 5.1). In general, only 2–3 mL of LA are enough to anesthetize a given territory, always remembering to inject in the vicinity of the nerve and aspirate first to prevent intravascular injection.
Supraorbital and Supratrochlear Nerves (V1)
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine