Key points
• Facial aging is characterized by fat atrophy and gravitational descent of facial soft tissue.
• Careful facial analysis is crucial for optimal outcomes.
• Fat grafting provides a minimally invasive technique to improve facial contouring in aesthetic and reconstructive patients.
• The Coleman technique for harvesting, processing, and grafting provides a reliable strategy for consistent results.
• Fat grafting is an effective tool to camouflage mild to moderate skeletal abnormalities.
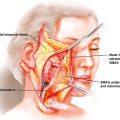
• A knowledge of vascular anatomy is necessary to minimize inadvertant arterial embolization.
Introduction
Autologous fat grafting has taken various applications since its inception in the 1800s from aesthetic to reconstructive purposes. Fat grafting was initially used in the face to improve tuberculosis-induced facial contour changes. Subsequently, it was trialed to obliterate the frontal sinus which still remains the gold standard today. But it was only in the 1980s and early 1990s that fat grafts were used as cosmetic fillers; however, the resorption rate was very variable and it was not widely used. Dr. Coleman popularized fat grafting with a reproducible technique. The tenets are aspiration of small aliquots of fat, processing the fat using centrifugation, separating out the unwanted components of the lipoaspirate (local anesthetic, oil, blood, and other noncellular material), and injecting the fat as tiny aliquots with each pass of the cannula. As research in the field increased, the indications and quoted graft retention rates also increased (as high as 90%), but the great variation persisted.
Youthful facial fullness is presumed to result from colloidal fluid held in place by a combination of hyaluronic acid, proteins, hormones, and other factors. These are gradually lost in the natural process of aging, and as a person approaches middle age, the fat deposits in the eyelids, cheeks, above the nasolabial folds, and the jowl become more visible as the surrounding fullness disappears. These changes also make underlying structures, such as submandibular glands and the facial skeleton, more obvious. As discussed in previous chapters, the aging face is universally characterized by fat atrophy as well as descent of the skin, muscles, and fat due to gravity and loss of elastic properties caused by time. González-Ulloa et al. have extensively discussed fat atrophy as the primary factor in aging and challenged surgeons to find ways of facial augmentation to reverse fat atrophy. Fat grafting allows us to address the atrophic changes caused by aging in a minimally invasive, yet very effective, manner. The transfer of fat from one part of the body to the face has proven to be a very powerful, effective, and longer-lasting treatment, especially compared with the increasing use of resorptive fillers, which can be a useful tool for temporary correction of facial defects. Furthermore, fat grafting will restore not only the youthful contours of the face but also its intrinsic qualities of skin texture, elasticity, and color return. Stem cells have been identified in large quantities in the harvested lipoaspirate and have been shown by our group to induce angiogenesis, skin thickening, and elasticity restoration.
Age-related atrophy is also associated with skin changes, excess skin laxity, and ptosis. Therefore fat grafting to the face is not only used as a stand-alone therapy, but often it is also used as an adjunct to other facial rejuvenation surgical procedures, such as rhytidectomy or blepharoplasty, to ensure an improved contour and smoother-appearing skin surface. This is to avoid an unnatural, overfilled, and unfeminine look caused by excess filling of the face. The potential aesthetic and surgical complications of fat grafting to the face warrant careful planning and attention to maximize the rejuvenation effect of lipofilling. This chapter examines the practical aspects involved in decision-making and in the technique of fat grafting to improve the contour of the facial skeleton.
Patient evaluation
As with any plastic surgery procedure, a thorough history and physical examination are the basis for a successful surgical strategy and a happy patient. The first step is to understand the patient’s concerns and goals to ensure that expectations can be met with fat grating alone and to determine whether other procedures are needed. The patient should be allowed to express what aspects of the face cause concern and what he or she hopes to achieve with surgery. Patients should be asked about recent weight changes and plans for future weight loss or gain. Evaluation of the patient’s preoperative medical status must include conditions that can affect the survival of fat grafting, such as smoking and tobacco use and history of prior infection (including methicillin-resistant Staphylococcus aureus ) or postsurgical infection. A surgical history, including prior surgeries, adverse events to anesthesia, and prior cosmetic medical or surgical procedures, should be taken. Patients should be specifically asked about prior liposuction or fat grafting procedures because these procedures can greatly affect the quantity and quality of fat that can be harvested from a donor site. A personal or family history of clotting or bleeding disorders, previous miscarriages, and deep vein thrombosis or pulmonary embolism should be noted. Allergies should be known, and lidocaine should be avoided if the patient is allergic to it. A thorough medication history should be obtained to determine whether the patient takes anticoagulants, such as enoxaparin, coumadin, aspirin, nonsteroidal antiinflammatory drugs, and certain vitamins and supplements known to affect clotting (e.g., vitamin K).
After a general examination, a thorough analysis of the face and potential fat harvesting donor sites should be conducted. Care should be taken to identify prior liposuction deformities to avoid worsening of those sites during harvesting. Facial analysis should be conducted in a methodical manner by using the basic principles of facial aesthetics. The texture and quality of the skin should be assessed. Special attention should be given to the supraorbital area, temporal area, nasolabial folds, lips, and neck. A youthful face is fuller, thanks to the underlying fat, which also helps to soften the contour of deep structures, such as bones, muscles, cartilage, and glands. The sequelae of facial skeletonization due to aging is more prominent in the upper third of the face than in the rest of the face, usually with a greater degree of hollowing instead of sagging, which is more characteristic of the middle and lower thirds. With aging, the shapes of the skull and the supraorbital bony rims become more prominent; the temples become hollowed; blood vessels are no longer hidden within the fat and stand out more; and the muscles of facial expression are more visible, creating a frowning or scowling appearance because of an increase in lines and folds in the forehead and glabellar regions. The eyebrows appear ptotic because of the loss of forehea d, temple, and brow fullness and loss of lateral support of the brow. The overall effect is that the lateral eyebrows can no longer be seen from the front giving an illusion of eyebrow shortening and lateral descent. The eyes may also become more deep set and eventually skeletal with a sunken look due to loss of fullness in the eyelids, eventually leading to dermatochalasis. Similarly, the inferior orbital rim becomes more prominent because of fat atrophy and tissue descent, leading to elongation of the lid–cheek junction and deepening of the tear trough and the nasolabial and marionette folds. The zygomatic arches become more prominent because of malar fat pad deflation. Lips deflate predominantly in the subvermilion and subcutaneous regions, leading to the orbicularis oris muscle coming more in contact with the vermilion and the mucosa, which results in perioral wrinkling, and significant changes in the upper and lower lips. Upper lip changes are more variable and include inversion, loss of visible vermilion, increase in maxillary incisor show, and illusion of overall lip narrowing. Lower lip changes include deflation, inversion, central depression loss, flattening of the central pout, and descent with associated mandibular incisors exposure. The contour of the mandible is also affected because of fat atrophy and skin ptosis. The jawline becomes less defined because of the relative ascent of the anterior and posterior jawline and the descent of the jowl, leading to the appearance of excess jowls.
Indications/contraindications
Fat grafting is a very powerful minimally invasive procedure to treat cosmetic and reconstructive deformities. Although the procedure is very well-tolerated, there are some contraindications, including hematologic abnormalities and anticoagulant medication use (e.g., coumadin, aspirin, clopidogrel). Care should be taken in patients who have unrealistic expectations or have body dysmorphic disorder. Lidocaine should not be used for infiltration or tumescence if the patient is allergic to it. As with other surgical procedures, patients should be medically stable.
Preoperative planning
Preoperative planning is critical for fat grafting. Patients should be adequately assessed, as described previously, and should undergo medical clearance. The appropriate laboratory tests should be performed before surgery. Patients should be instructed to stop all medications that interfere with platelet function 2 weeks before surgery to avoid bleeding complications. Patients should be encouraged to stop smoking at least 1 month before surgery. Photographs of the face and the donor sites should be taken from various angles. Photographs are helpful to plan the surgery, trace the amount and location of planned fat harvesting and grafting, plan the cannula entry points, and critically assess the results postoperatively. Anesthesia type should be discussed preoperatively with the patient and the anesthesia team because both the harvesting and grafting of fat can be performed under general anesthesia or local anesthesia (or regional block), with or without intravenous sedation, depending on the amount of planned fat transfer and the surgical site. Informed consent should be obtained after discussing the procedure, alternatives, and complications. The surgeons should discuss postoperative care and prepare the patient on what to expect during the recovery period. The surgical plan, risks, and benefits should be reviewed again on the day of surgery to address any remaining patient concerns. Throughout preoperative planning, the surgeon should gauge the goals of the patient to ensure that the expectations are realistic and that the patient is ready for the surgery.
Primary operative approach and surgical technique
Patient positioning
Positioning of the patient is dictated by the donor and recipient sites. Fat can be harvested from anywhere in the body, but, often, the harvest site is selected according to the preference of the surgeon, the patient, or both. Usually, the biggest determinant of donor site selection is the amount of fat available for harvesting. As discussed in Chapter 14 , the site has no impact on how much of the harvested fat can be used after processing. Furthermore, both animal and human studies have shown no differences. Therefore the decision regarding the harvest site should be based on safety, ease of access, and the preference of the patient. Generally, patients undergoing facial fat grafting will be placed in the supine position to facilitate easy access to the inner thighs, flanks, and abdomen for harvesting and to the face for transfer. The donor and recipient sites are then prepared with povidone-iodine (Betadine), and the patient is draped in a sterile fashion. Various techniques to harvest, process, and inject fat have been described, but this chapter will focus on our preferred technique, which is commonly described as the Coleman technique.
Harvesting
Tumescent solution is infiltrated subcutaneously through small incision sites (approximately 2 mm) usually hidden within skin creases, stretch marks, previous scars, or the umbilicus. The volume infused should be less than the amount of fat harvested. If local anesthesia is used, the infiltration solution consists of 0.5% lidocaine with 1:200,000 epinephrine buffered with sodium bicarbonate infused with a Lamis (or other blunt) infiltration cannula (Mentor Worldwide LLC, Santa Barbara, CA). If intravenous sedation or general anesthesia is used (preferred for removal of larger volumes), the infiltration solution of choice is 0.2% lidocaine, lactated Ringer’s solution with 1:400,000 epinephrine. No tumescent solution techniques are used for two reasons: first, the potential for mechanical damage to fat parcels, which may decrease the survival of the transferred fat; and, second, the inefficiency and prolongation of the procedure due to an excessive fluid fraction in the aspirate. The solution is left in for 10 minutes before fat harvesting to optimize the vasoconstrictive effects. A nine-hole Coleman harvesting cannula (12- or 14-gauge, 15- or 23 cm-long, depending on the volume needed), attached to a 10-mL syringe, is used to harvest fat. A curved cannula may be helpful when harvesting from the flanks and other curved regions. The plunger of the syringe is pulled back only 1 to 2.5 mL to create enough vacuum to harvest the fat while minimizing pressure of vaporization that could rupture fat cells.
Processing
After each syringe is filled, the cannula is disconnected and replaced with a Luer-Lok cap (Becton, Dickinson and Company, Franklin Lakes, NJ) to prevent spillage during centrifugation. The plunger is then removed. Syringes are then placed into individual sleeves within a sterilized centrifuge and spun at 1286 g for 2 minutes to separate the viable components from the nonviable components of the tissue. This process produces three layers: a top supernatant layer (least dense) containing oil from ruptured cells; a middle layer containing adipose tissue, adipose-derived stem cells (ASCs), stromal cells, vascular cells, endothelial cells, and mural cells, termed the stromal vascular fraction (SVF); and a lower layer (most dense) containing blood, tissue fluid, and the local anesthetic. The oil in the top supernatant layer is decanted, and then the Luer-Lok cap is removed, allowing the lower aqueous layer to be drained from the bottom of the syringe. A Codman neuropad (Codman Neuro, Raynham, MA) is then placed in the superior portion of the harvested fat found in the syringe to wick away the remaining oil. Another neuropad can then be replaced after 4 minutes, but care should be taken to minimize the time that the fat is exposed to air. The plunger is then replaced after allowing the fat to slide to the bottom of the syringe. The processed fat is then transferred to 1 mL Luer-Lok syringes for placement, and the plunger is replaced and advanced ready for use.
Fat transfer
The planned incision sites for fat transfer are locally anesthetized with 0.5% lidocaine with 1:200,000 epinephrine before creating stabbing incisions with a No. 11 scalpel. The graft is also infused with small volumes of 0.5% lidocaine with 1:200,000 epinephrine for anesthesia and vasoconstriction. This reduces the risk of bruising, blood loss, hematoma, and the risk of intraarterial injection of fat, especially when injecting around the periorbital or temporal areas. The incisions can be lubricated by using the decanted oil produced from centrifugation to avoid causing friction on the puncture or incision sites with the infiltrating cannula. Selection of the appropriate cannula is key to success. We use cannulas developed by SRC Inc., which consist of three basic styles of blunt-tipped cannulas as well as a V- or W-dissectors (Mentor, Irvine, CA):
- •
Coleman type I cannula—completely capped on the tip with a lip extending 180 degrees over the distal aperture. This is the workhorse cannula for most facial fat grafting because it reduces the risk of iatrogenic traumatic injury to the underlying structures.
- •
Coleman type II cannula—similar to type I, but partially capped. It has a lip extending over the distal aperture at approximately 130 to 150 degrees. This cannula is useful in the majority of situations, but it is a little more traumatic.
- •
Coleman type III cannula—flat end (not capped) allowing dissection of tissues in cases of fibrotic tissue or old scars or when subdermal infiltration is needed.
- •
Coleman V-dissector and W-dissector—sharper cannulas used to release adhesions.
Although cannulas of different gauges and lengths can be used, we use smaller gauge (21-gauge) and shorter length (3 to 7 cm) cannulas for facial fat grafting, especially when grafting in the eyelids. The infiltration technique is crucial to increasing the survival of fat grafts. The principles of infiltration are based on fat injections in adequately vascularized tissue and avoiding infiltration of large volumes. Fat should therefore be infiltrated in small aliquots (no more than 0.1 mL of fat with each pass) as the cannula is withdrawn. Transferring fat parcels that are too large may lead to oil cysts, fat necrosis, fat resorption, contour irregularities, or infection. Fat can be injected at different depths, depending on the needed outcome. Fat injected in the intradermal or subdermal layers improves facial skin quality and smooths wrinkles, but surgeons should be aware of the increased risk of creating superficial contour irregularities. Fat injected in the subcutaneous layer restores volume to correct fat deficiencies, to rejuvenate, and to reestablish facial proportions. Fat injected in the supraperiosteal layer can be used to change how the remaining soft tissue envelope drapes over the bone structure of the face. Molding of, and pressure on, the fat placed should be avoided because of the risk of fat necrosis and resorption. When injecting larger volumes, it is recommended that injection be performed evenly by using multiple passes, different ports, different trajectories, and different depths to minimize the risk of contour irregularities and improved fat survival. However, this will vary significantly, especially if reconstructing traumatic or oncological defects. The combination of small-aliquot injections and even distribution grants maximal amount of contact between the fat parcels and the surrounding recipient tissue for better fat graft survival through imbibition and neovascularization. Throughout the injection process, it is important to compare the treated site with the contralateral side to ensure adequate symmetry. The surgeon should also be aware of the tip of the cannula at all times to avoid causing injury to vital structures. Once satisfied with the injected volume and contour, the facial incisions are sutured with interrupted 5-0 fast gut and then infiltrated with 0.2 to 0.3 mL of concentrated fat by using a 22-gauge needle to aid healing of the incision sites. The donor-site incisions are closed with buried, deep-dermal 3-0 Monocryl sutures.
Case 1
A 50-year-old woman presented with hollowing of the temples with prominent veins, hollowing of the orbits, prominent tear troughs, loss of malar prominence, and loss of definition of the nasal dorsum ( Fig. 35.1 A–D). A total of 200 mL of fat was harvested from her inner, outer, and anterior thighs by using 10-mL syringes and Coleman harvesting cannulas. The fat was processed in the standard manner by using the Coleman technique described previously. The refined fat was then placed as follows: right temple, 4 mL; left temple, 3.5 mL; glabella, 1.5 mL; right upper eyelid, 2 mL; left upper eyelid, 2 mL; right lateral eyelid, 0.8 mL; left lateral eyelid, 0.8 mL; dorsum, 2 mL; right anterior malar fold, 2 mL; left anterior malar fold, 2 mL; right lateral infraorbital rim, 2 mL; left lateral infraorbital rim, 2 mL; right lateral cheek, 1 mL; and lateral cheek, 1 mL. The fat was placed by using a combination of Coleman cannulas and 22-gauge needles, but mostly with type III cannulas. Fig. 35.1 shows photographs of the patient preoperatively with and without markings of the areas to inject and at 4 months and at 1 year after fat grafting, with no other procedures in the interim. The patient obtained lasting restoration of fullness in every area of the face infiltrated, a decrease in hollowness, reduction of visibility of the temple veins, and a remarkable improvement in the quality of skin over time.