Lip Reconstruction With Radial Forearm Free Flap
Vishal Thanik
DEFINITION
Lip reconstruction is restoration of form and function after loss from a number of causes, the most common being oncologic resection and trauma.
The lips are critical functional units in the processes of speech and alimentation and are one of the prime conveyors of emotion in the human face. They are also a focus of beauty in cultures worldwide.
Reconstructive options in lip reconstruction are determined primarily by size and location of the defect; as defects become larger in more critical locations, functional outcome becomes paramount and aesthetic quality diminishes.
Smaller defects typically can be addressed with local flaps, and in general, the use of free flaps is reserved for defects that cannot be reconstructed with local tissue alone.
ANATOMY
The lips are a trilaminar structure containing mucosa, muscle, and skin.
External anatomy (FIG 1A)
Upper lip—base of nose to nasolabial fold
Lower lip—mental crease to nasolabial fold
Corners of the lip referred to as commissures
Skin transitions to mucosa at the vermilion border, with the transition skin referred to as the white roll.
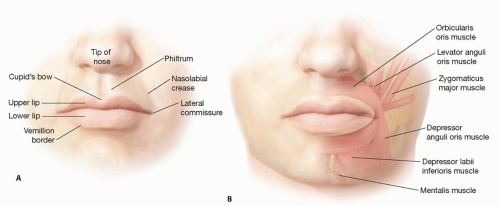
FIG 1 • A. External anatomy of the lip. B. Musculature of the lip.
Midline of the upper lip has a curve referred to as the “Cupid’s bow.”
Cupid’s bow progresses vertically to the philtrum, a depression that is bordered on either side by the philtral columns.
The vermilion is a specialized mucosal surface that does not contain minor salivary glands.
Internal anatomy (FIG 1B)
Muscular anatomy of the lip functions as a specialized sphincteric system.
Orbicularis oris forms a sphincteric ring and is the major muscle of the trilaminar structure.
Major elevators of the lip are the zygomaticus major and levator anguli oris, with zygomaticus minor and levator labii superioris as secondary elevators.
Major depressor of the lip is the depressor anguli oris, with contributions from the depressor labii inferioris, mentalis, and platysma.
The modiolus is just lateral to the commissure and is the confluence of muscle fibers to the dermis, the functional insertion of the levator and depressor muscles.
Innervation
Sensory innervation to the upper lip is provided by the maxillary branches of the trigeminal nerve, whereas the lower lip is supplied by the mandibular branches.
Motor innervation is via branches of the facial nerve.
Vascular supply
The facial artery is the main blood supply to the lip and branch, diving and entering the lips laterally, becoming the superior and inferior labial arteries. These vessels can run between the mucosa and orbicularis muscle or through the muscle depending on the patient.
PATIENT HISTORY AND PHYSICAL FINDINGS
Understanding the underlying etiology of the defect is paramount. Traumatic wounds can generally be reconstructed immediately after adequate debridement and ruling out of concomitant injuries that could delay treatment. With oncologic defects, margin status and need for further excision or adjuvant therapy should be assessed prior to reconstruction.
A full history should be established, with particular attention paid to previous lip/facial reconstruction, smoking and comorbid status, and any history of radiation therapy of the head and neck.
Physical examination requires assessment of the defect and the surrounding tissues.
Assessment of the size and location of the defect, as well as the size of the opposite, typically normal lip
Evaluation of the depth of injury, including status of the orbicularis oris
Evaluation of the opposite lip for concomitant injury, typically in trauma
Neurovascular examination, inventorying sensibility and perfusion of the remaining lip
Evaluation of donor sites if free flap reconstruction is warranted
IMAGING
Imaging is typically unnecessary prior to lip reconstruction.
In patients with traumatic lip defects, head CT and C-spine imaging may be performed to rule out concomitant injuries.
Surgical Management
Operative management of lip defects depends on the location, size, and thickness of the defect.
Partial-thickness defects of the lip and vermilion, if small (generally less than 30% of the lip), can be converted into full-thickness defects and closed primarily in a V-shaped manner.
Larger partial-thickness defects of the vermilion that are not amenable to V-excision and closure are best managed with mucosal advancement flaps from the labial or buccal surface. Other options include mucosal V-Y advancement flaps or cross-lip mucosal flaps.1,2
Large, full-thickness defects of the lip are considered those that are 80% or more. For defects of this size, free flap reconstruction is usually indicated. Another option in some patients, particularly those who are not free flap candidates, is bilateral nasolabial flaps or other local approaches.
Lower lip defects are more common than the upper lip defects due to increased sun exposure.
Full-thickness lower lip defects reconstructed with free flaps are difficult due to the potential for lip incontinence and benefit from suspension of the flap with a tendon or fascia graft. Upper lip defects typically do not require tendon grafting.
The radial forearm flap is the workhorse flap in lip reconstruction because of its thinness and pliability, ability to easily integrate the palmaris tendon, and long pedicle length, which facilitates anastomosis in the neck or superficial temporal system.3,4Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree