8Lip (Perioral) Reconstruction
Abstract
This chapter presents an algorithmic approach to reconstructive options for repairing perioral defects after Mohs micrographic surgery with a focus on cosmetic subunits. These algorithms represent common reconstructive techniques and their variations utilized within each subunit in the perioral region serving as general principles. Perioral anatomy, key principles, practical pearls, and common pitfalls are reviewed to offer a solid foundation for successful perioral reconstruction.
Capsule Summary and Pearls
•Know the perioral anatomy including cosmetic subunits, neurovascular supply, musculature, and tissue reservoirs.
•Restoration of the oral sphincter is prioritized, followed by preservation of motor and sensory innervation and optimizing cosmesis.
•Mark cosmetic subunits, vermilion border, and favorable lines of closure with ink prior to local anesthesia.
•Respect the various cosmetic subunits when designing closures.
•Maintain the position and alignment of the vermilion-cutaneous junction (VCJ) and the philtrum at the midline.
•Place closures along relaxed skin tension lines and at the junction of cosmetic subunits.
•Do not distort the free margin.
•The vermilion is not an inviolable structure.
•Recruit tissue from lateral reservoirs on the lip or adjacent cheek.
•Consider extending surgical defects to subunit boundaries or removing an entire subunit in order to better conceal the incision lines of the repair.
•Repair defects within a single subunit when possible.
•Divide defects that bridge the VCJ into vermilion and cutaneous defects and repair each individually.
•Avoid pincushioning by appropriately sizing and adequate thinning of flaps and undermining the surrounding tissue.
•Achieve thorough hemostasis of the lip prior to closure.
•Recreate the alar crease at the isthmus and the melolabial fold with a periosteal stitch.
•Close vermilion–vermilion and vermilion–cutaneous wound edges with braided interrupted sutures.
•Close full-thickness defects in four layers, starting with reapproximation of the orbicularis oris sphincter.
•Always consider individual factors in selecting the best method of repair.
•Limit mobility of the perioral region postoperatively to avoid complications and maximize cosmetic results.
8.1 Introduction
The upper and lower lips are the predominant feature of the lower face and carry considerable aesthetic significance. Beyond this, the lips have important motor and sensory functions including facial expression, oral competence and articulation of speech, as well as the protective perception of touch, pain, and temperature. The variations in texture, color, and contour between its numerous cosmetic subunits add to the complexity of the perioral region. Given these significant functional and aesthetic considerations, perioral surgical defects present reconstructive challenges from which innovation has led to a multitude of repair options. The goal in all lip reconstructions is to preserve or restore the function and aesthetics of this unique structure. Key principles for successful perioral reconstruction are detailed in Capsule Summary and Pearls at the beginning of this chapter.
8.2 Cosmetic Subunits and Relevant Anatomy
The perioral region is comprised of five distinct cosmetic subunits: two cutaneous lateral upper lip subunits, the philtrum, the cutaneous lower lip and chin, and the vermilion lip (Fig. 8.1). Together, the philtrum and two lateral subunits form the cutaneous upper lip. The nasal base, defined by alar creases, the alar sill, and the columella border the upper lip superiorly. The melolabial fold and the labiomandibular crease (marionette lines) serve as the lateral boundaries of the upper and lower lips, respectively. Although considered a single subunit, the lower lip and chin can be divided at the labiomental crease, which serves as the inferior limit to the lower cutaneous lip. A small triangle of skin, the isthmus or the hairless triangle, exists in the superolateral corners of both cutaneous lateral upper lip subunits adjacent to the nasal ala. These apical triangles warrant special consideration during reconstruction, as their preservation is essential to optimize cosmetic outcomes. Of similar aesthetic importance, the philtrum is a concave subunit bounded by parallel convex philtral columns in the medial upper lip and is defined inferiorly by the Cupid’s bow of the vermilion lip.
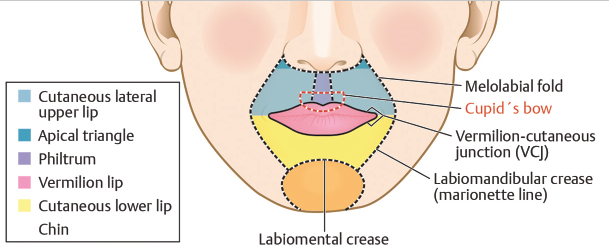
Fig. 8.1 Perioral cosmetic subunits and junctions.
The transition from cutaneous upper and lower lips to vermilion takes place at the vermilion-cutaneous junction (VCJ). A well-defined line, referred to as the mucocutaneous or anterior vermilion line, and its rolled border represent an important landmark in lip reconstruction. The combination of thin, nonkeratinizing epithelium and abundant underlying vasculature gives the vermilion a characteristic pink hue. The modified mucosa of the vermilion covers the free margin of the lip and is adapted for external exposure, with relatively few salivary glands compared to the multitude found deep to the labial and buccal mucosa.1 Its surface is divided into internal (wet) and external (dry) components and the innermost point of contact between the upper and lower lips is defined as the posterior vermilion line.
From superficial to deep, lip tissue is comprised of skin, muscle, and mucosa. The body of the lip is predominantly formed by the orbicularis oris muscle, which is concentrically oriented and inserts directly into the skin’s undersurface. The relaxed skin tension lines (RSTLs) of the upper and lower lips are oriented in a radial fashion about the oral stoma coursing perpendicularly to the underlying orbicularis muscle. These radial lines are accentuated with pursing and are ultimately paralleled by the wrinkle lines of older patients and enhanced by chronic sun damage and smoking (Fig. 8.2). The radial RSTLs, the melolabial fold, and the labiomental crease are favorable sites to conceal incisions in lip reconstruction.
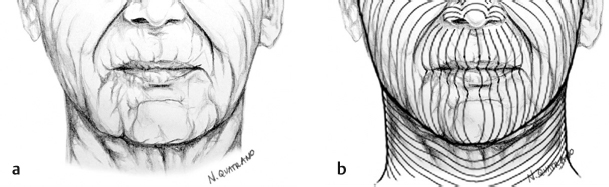
Fig. 8.2 Perioral relaxed skin tension lines (a) and overlying Langer’s lines (b).
In bilaterally paired sets, the muscles of facial expression attach radially along the outer margin of the orbicularis oris, marked by the melolabial fold and labiomental creases. Motor innervation to these lip elevators and depressors originates primarily from the buccal and marginal mandibular branches of the facial nerve, respectively. Although rarely damaged due to their location beneath the musculature, injury to the marginal mandibular nerve anterior to the angle of the jaw during undermining as the nerve becomes more superficial over the bony prominence can lead to significant functional and cosmetic deformity due to the inability to laterally depress the lower lip.2 This inability is most notable when smiling due to the resulting asymmetry but can also effect speech.
Many of these muscle fibers converge at the modiolus just lateral to the commissure and, as a group, provide the orbicularis oris with an indirect connection to the facial skeleton. This lack of direct connection allows for the advantage of lip tissue to be significantly stretched during reconstructive surgery.1 Even with larger defects slightly more than half of either lip, reconstruction can be accomplished in most cases without causing excessive microstomia. When the orbicularis oris muscle is compromised, priority is placed on restoration of the muscle sphincter. The orbicularis oris muscle sphincter of the lower lip is crucial given its greater role in the retention of intraoral contents.3
Sensory innervation of the upper lip originates from branches of the infraorbital nerve, while branches of the mental nerve provide that of the lower lip. Both infraorbital and mental nerves arise from foramens along the mid-pupillary lines in the maxilla and mandible, respectively, and can be reached percutaneously or via an intraoral route for regional blocks if needed (Fig. 8.3).
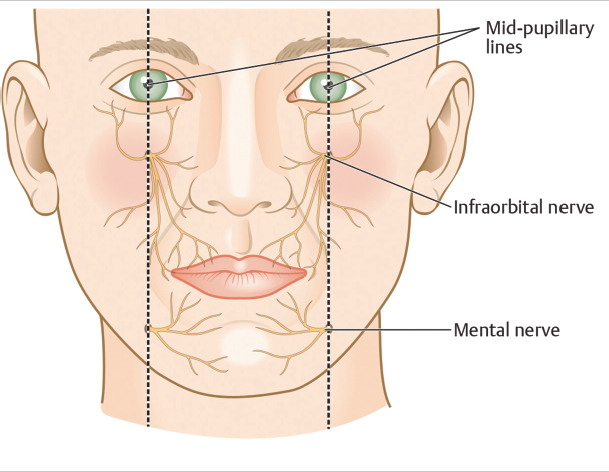
Fig. 8.3 Sensory innervation to the upper and lower lips.
Superior and inferior labial arteries provide the principal vascular supply to the lips. Both arteries originate from the facial artery along its course beneath the orbicularis oris muscle about 10 to 12 mm from the oral commissure.4 Often with a tortuous course, the labial arteries run horizontally in the submucosal plane, just beneath the orbicularis and at approximately the level of the anterior vermilion line. While the superior labial artery gives off septal and alar branches medially, the lower labial artery anastomoses with the mental artery through a variable pattern of labiomental branches often vertically oriented across the lower lip and chin (Fig. 8.4).5,6,7
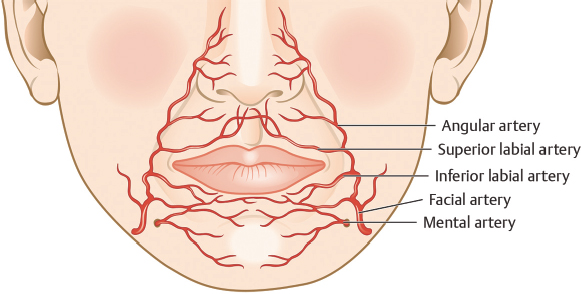
Fig. 8.4 Arterial anatomy of the upper and lower lips.
8.3 Reconstructive Algorithm
When planning reconstruction of the perioral region, great effort should be made to maximize cosmesis; however, priority should always be placed on the preservation of function. Careful marking of the vermilion border, aesthetic subunits, and favorable lines of closure, such as the RSTL and subunit junctions, is essential prior to executing any perioral reconstruction and preferably done prior to local anesthetic infiltration. One of the most important considerations in lip reconstruction is preservation of lip position. Pushing or pulling the upper or lower lip out of place, pulling the Cupid’s bow off center, or creating any misalignment of the vermilion border can be aesthetically devastating and all efforts must be made to plan reconstructive options that minimize these outcomes. Over time, the high mobility of the perioral region tends to organize tissue in this region back toward baseline positioning and, therefore, even large repairs can result in excellent final outcomes. In addition, it is better to confine reconstructive design to within a single subunit using tissue from within the respective aesthetic region of the lip. With larger defects or those that span multiple subunits, repairs are more likely to involve tissue from the adjacent regions of the cheek or chin.
Certain repairs are more commonly utilized within specific subunits as their closure lines are favorably hidden in the lines of that subunit. The location, size, shape, and depth of the defect will influence the choice of closure within a given subunit. Individual patient characteristics such as skin texture, thickness, and laxity (often influenced heavily by age and sun damage) should also be taken into consideration when choosing the optimal closure. However, an algorithmic approach based on region can be helpful as common patterns of repair within certain aesthetic subunits can serve as a guideline for reconstructive design.8
8.3.1 Vermilion
The vermilion lower lip is most commonly plagued with squamous cell carcinomas (SCC), often in the setting of actinic damage and tobacco exposure. While SCC of the vermilion upper lip tend to involve the cutaneous lip, those of the lower vermilion often have little to no cutaneous involvement, unless they are allowed to progress before treatment. For this reason, defects limited to the vermilion lower lip are considered separately (Fig. 8.5), while defects involving the vermilion upper lip are included in the algorithms described below for the cutaneous upper lip.
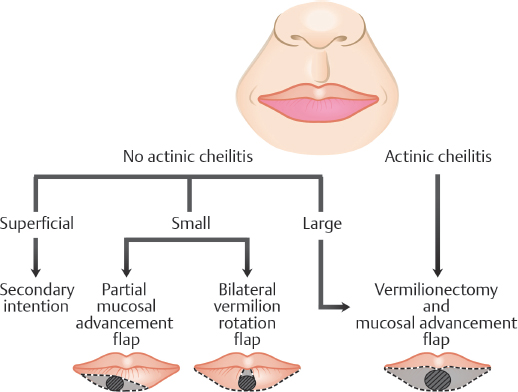
Fig. 8.5 Vermilion lower lip reconstruction algorithm.
After tumor extirpation, second intention healing can be considered for partial-thickness defects restricted to the vermilion. Superficial defects limited to the mucosal lip are often best left to heal with granulation alone and even some larger defects with partial resection of the orbicularis can heal by second intention with satisfactory results.9,10 With an abundant vascular supply, defects of the mucosal lip re-epithelialize rapidly. A visible stellate scar may result from and represent a disadvantage of second intention healing but can be easily revised with minimal recovery (Fig. 8.6).
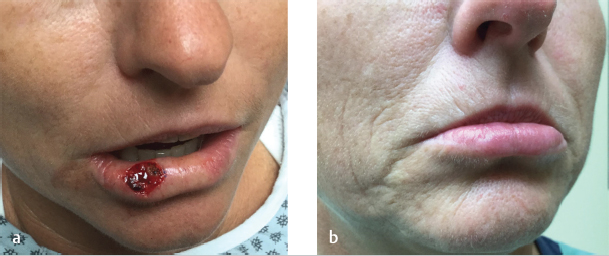
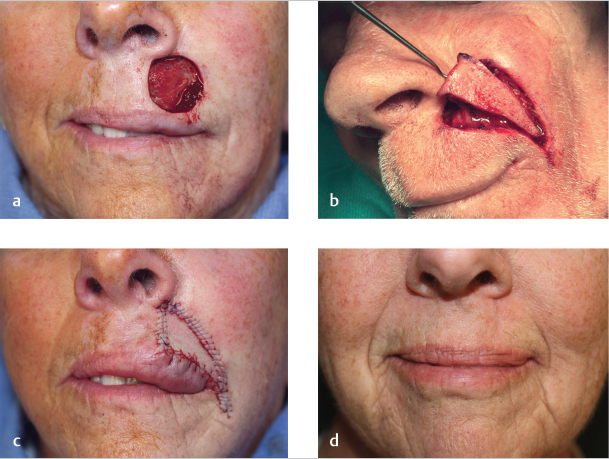
Fig. 8.6 Second intention healing. (a) Defect limited to vermilion lower lip. (b) Final result with subtle stellate scar. (These images are provided courtesy of Stanislav N. Tolkachjov, MD.)
The remaining vermilion after tumor extirpation often consists of actinically damaged tissue. For defects in this setting, a complete vermilionectomy, followed by repair of the entire vermilion subunit is preferred. The favored method of vermilion restoration is the mucosal advancement flap (Fig. 8.7). With any vermilion repair, the design, wet–dry line, and vermilion border should be marked prior to local anesthesia. When performing the vermilionectomy, the anterior incision lines extend laterally from the defect along the VCJ, while the posterior incision lines extend laterally from the most posterior aspect of the defect to meet the anterior incision lines at the commissures with removal of mucosal Burow’s triangles as necessary. The vermilion is then removed with care to minimize trauma to the underlying orbicularis muscle. The mucosal advancement flap utilizes the mucosa lining the inner surface of the lip and is elevated by undermining within the submucosal plane deep to the minor salivary glands and immediately superficial to the orbicularis muscle. To allow sufficient anterior advancement under minimal tension, dissection may need to be extended along the vertical length of the lip to the apex of the gingivolabial sulcus, but this is often not required. The flap is then advanced anteriorly over the free margin of the lip to the anterior vermilion line where a key suture is placed in the middle of the advancing edge. Soft braided absorbable suture, such as polyglactin 910, is used to place interrupted sutures along the remainder of the flap’s leading edge and reestablish the VCJ. The editors often use nonabsorbable epidermal sutures only if sufficient undermining has been done to relieve tension. Accurate positioning of the VCJ is of upmost importance for optimal aesthetic outcome and can be challenging especially in the setting of an adjacent cutaneous lip defect. Inherent contraction of the mucosal flap with wound maturation may distort the anterior vermilion line despite best efforts to properly align and require subsequent revision surgery. If needed, additional excision of the normal tissue of adjacent cutaneous lip may allow for proper alignment.
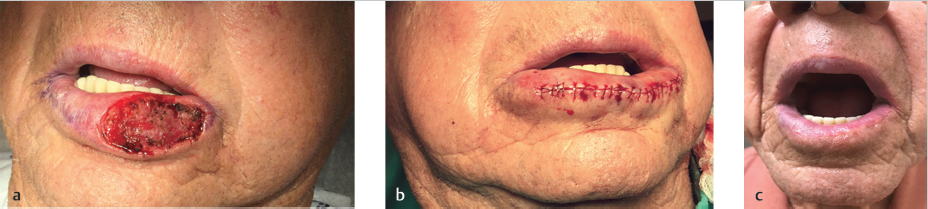
Fig. 8.7 Mucosal advancement flap (complex layered closure). (a) Vermilion lower lip defect. Vermilionectomy design marked. (b) Mucosal flap advanced and sutured. (c) Final result (1-year follow-up). (These images are provided courtesy of Stanislav N. Tolkachjov, MD.)
For small defects restricted to the vermilion where there is minimal adjacent actinic cheilitis, a partial mucosal advancement flap and a bilateral vermilion rotation flap are excellent reconstructive options. Both techniques allow preservation of the healthy vermilion and favorable placement of closure lines along the VCJ. A partial mucosal advancement flap may be favored for defects with a long axis aligned with the anterior vermilion border. An ellipse is designed that places the anterior incision along the vermilion border without extending the incisions from commissure to commissure. After removal of the vermilion cones, a partial mucosal advancement flap is elevated and brought anteriorly to meet the VCJ as described earlier.
A bilateral vermilion rotation flap is designed with bilateral incisions off of the anterior aspect of the defect along the VCJ (Fig. 8.8). The flaps are elevated superficial to the orbicularis and a mucosal Burow’s triangle is taken posterior to the defect. Incisions along the VCJ may be extended to the commissures to allow adequate rotation under minimal tension but may not be required. Soft, braided absorbable interrupted sutures allow precise VCJ and flap alignment. The main advantage of a bilateral vermilion rotation flap is the tension is largely displaced laterally and therefore does not pull the lower cutaneous lip up superiorly, making the lower lip appear smaller (as can occur with mucosal advancement flaps).

Fig. 8.8 Bilateral vermilion rotation flap. (a) Vermilion lower lip defect. (b) Bilateral rotation flaps sutured in place. (c) Final result.
8.3.2 Cutaneous Lateral Upper Lip
The cutaneous lateral upper lip can be further divided into apical and mid-lower regions, which are helpful to consider when debating reconstructive options. Second intention healing on the cutaneous lateral upper lip is limited to superficial defects located in concavities such as that of the isthmus or apical triangle.11 Granulation of deeper defects often creates a hypertrophic scar. Full-thickness skin grafts (FTSG) are rarely used in this area as they are often complicated by pincushioning, offer a poor color and texture match, and are an unacceptable alternative for the hair-bearing upper lip of men. Primary linear closures are useful for small defects in the mid-lower lateral subunit. For apical or larger defects, a variety of local flaps can be utilized to tap into regional or distant laxity and displace tension, thereby avoiding displacement of the free margin. Local skin redundancy offers excellent texture, thickness, appendage, and color match. Most local flaps in the perioral region are advancement or rotation flaps that slide tissue, almost always, from a laterally based reservoir along natural motion vectors and stay within the cosmetic unit. Depending on the location of the defect, specific flaps are used in particular regions of the cutaneous lateral upper lip to best hide suture lines (Fig. 8.9). Ultimately, individual variation in tissue laxity and size of the cosmetic subunits will heavily influence the reconstructive method chosen.
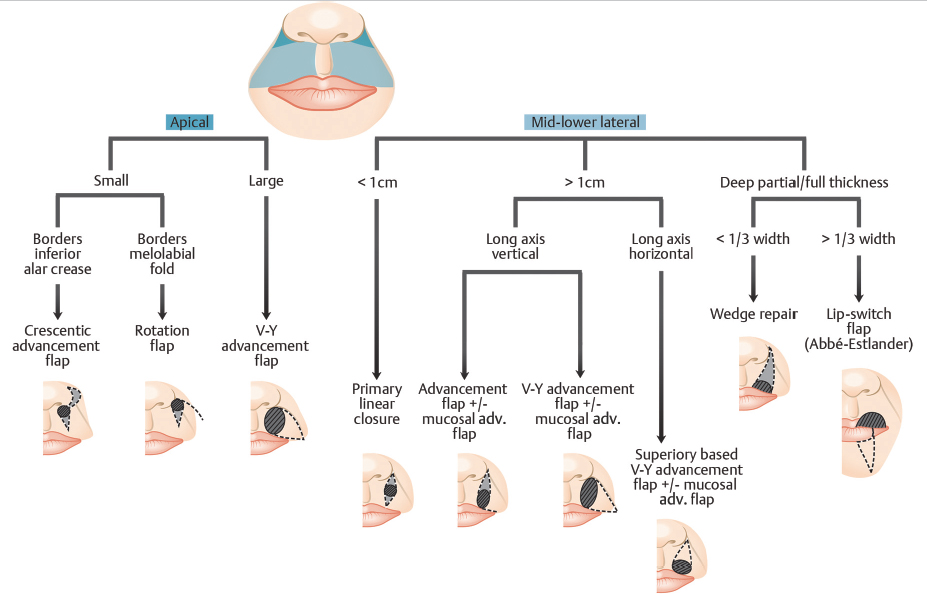
Fig. 8.9 Cutaneous lateral upper lip reconstruction algorithm . adv., advancement.
Small defects, less than 1 cm in diameter, on the lateral subunit can be closed primarily with a linear closure without the concern of free margin distortion.8,12 A fusiform defect is first created by removing Burow’s triangles with the optimum angle of 30 degrees at the apices above and below the primary defect. Closure lines should deliberately be placed along the radial RSTLs or at the junction of cosmetic subunits to both minimize tension on the wound and improve cosmetic results. With a linear closure, the distance between the two ends of the defect will lengthen to match that of the fusiform’s arc. The superior portion of the closure should not cross the melolabial fold, and if approaching this boundary, the scar line should be redirected along the alar crease for better camouflage. If the inferior portion of the closure ends near or on the vermilion border, extension of the incision through the upper vermilion to the mucosal portion of the lip is often required to avoid standing cones (Fig. 8.10). This is favored over the use of an M-plasty, which extends outside of the RSTLs and is therefore less well camouflaged and, with all of the very small and acute angles, is more prone for tissue mismatch and minor step-off deformities. Minimal tension on the closure is achieved through undermining laterally above the orbicularis oris. During layered suturing, emphasis is placed on maintaining alignment of the VCJ as even small offsets yield poor aesthetic results. Once again, careful marking of this important landmark prior to local anesthetic infiltration is essential to aid in precise repositioning. Suturing technique to optimize wound eversion is critical on the upper lip, especially on the hair-bearing lip of men where decreased collagen density between hair follicles reduces suture grip and increases the risk of scar inversion.13
Apical Triangle
Apical defects are best reconstructed with flaps that hide suture lines within the perialar groove or melolabial fold. Crescentic advancement flaps are ideal for small defects in the apical region that borders the inferior alar crease or lateral nostril sill. With this repair, the inferior Burow’s triangle is placed along the RSTLs of the upper lip, identical to that in primary closure; however, the superior Burow’s triangle is displaced along the alar crease in a crescentic fashion to facilitate medial advancement of tissue (Fig. 8.11). After excision of both triangles, the flap is undermined laterally in the subcutaneous tissue and advanced medially to bring together the inferior aspect of the crescent and the superior aspect of the defect with a key suture. For larger defects that have more tension on the closure, deep tacking sutures from the flap to periosteum below the ala help advance the flap medially without pulling the ala laterally. The crescent may be excised after advancement and closure of the lip in order to minimize the excised tissue.14 Strategic placement of incision lines within the RSTLs and the alar groove consistently results in well-concealed scars and excellent cosmetic outcomes.
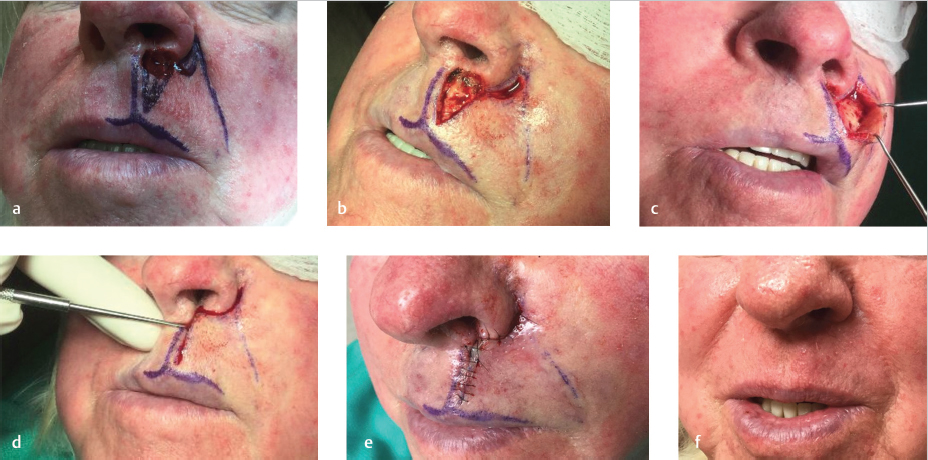
Rotation flaps offer an excellent reconstructive option for similarly sized defects of the apical region that border the melolabial fold (Fig. 8.12). Once again, the inferior Burow’s triangle is designed along the RSTLs of the upper lip. The arc of the rotation flap is designed from the superior aspect of the defect and extends inferolaterally along the melolabial fold. The incision should be designed outside of the fold and then follow its curvature in order to maintain both lip height and proper position of the melolabial fold upon medial rotation and closure. Undermining takes place laterally in the subcutaneous–orbicularis oris junction of the lip and the flap is both rotated and advanced medially to close the defect. The repair is confined within the cutaneous lateral upper lip subunit and suture lines are well camouflaged within the melolabial fold offering excellent cosmetic outcomes. A variation on this repair displaces the inferior Burow’s triangle along the lateral alar crease extending to the alar sill, offering superior camouflaging of incision lines along subunit junctions.

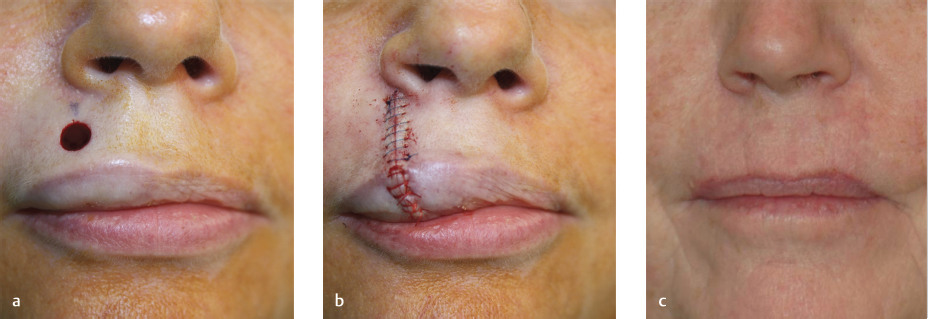
Fig. 8.12 Rotation flap. (a) Apical region defect bordering the melolabial fold. (b) Flap sutured. (c) Final result.
Both the crescentic advancement and rotation flaps can be utilized for larger defects of the apical region by extending the inferior Burow’s triangle through the VCJ and onto the vermilion as described for primary linear closure earlier. However, for larger defects of the apical region, specifically those that abut the nasal ala and the melolabial fold, V-Y advancement flaps, traditionally referred to as island pedicle flaps (IPF), may be better a reconstructive option.15 Unlike other advancement flaps that are pulled into place, the V-Y flap is mobilized as a subcutaneous island that is pushed toward the primary defect through closure of the secondary defect. The V-Y flap is designed with its leading edge along the inferolateral aspect of the defect and its axis parallel to the melolabial fold. The two limbs of the triangular incision should be placed along boundary lines whenever possible. The superior lateral limb of the V-Y flap is placed along the melolabial fold to preserve this boundary and for optimal camouflage. The incision should be carried outside of the fold and then mimic its curvature in order to both maintain lip height and properly position the melolabial fold upon closure. Depending on the proximity of the defect’s inferior margin to the vermilion, the inferior limb can be well camouflaged along the VCJ (Fig. 8.13). Expanding the defect superiorly to the alar base or inferiorly to the vermilion through removal of intervening skin may be necessary to facilitate this placement and avoid transection of the RSTLs by the inferior scar line. The width of the flap should match the widest diameter of the defect and its length should be at least twice that diameter along the axis of the flap.16 Gradual tapering of the limbs to meet at an angle no more than 30 degrees minimizes any upward or lateral tension on the oral commissure upon closure.