Lip (Cancer and Reconstruction)
Description
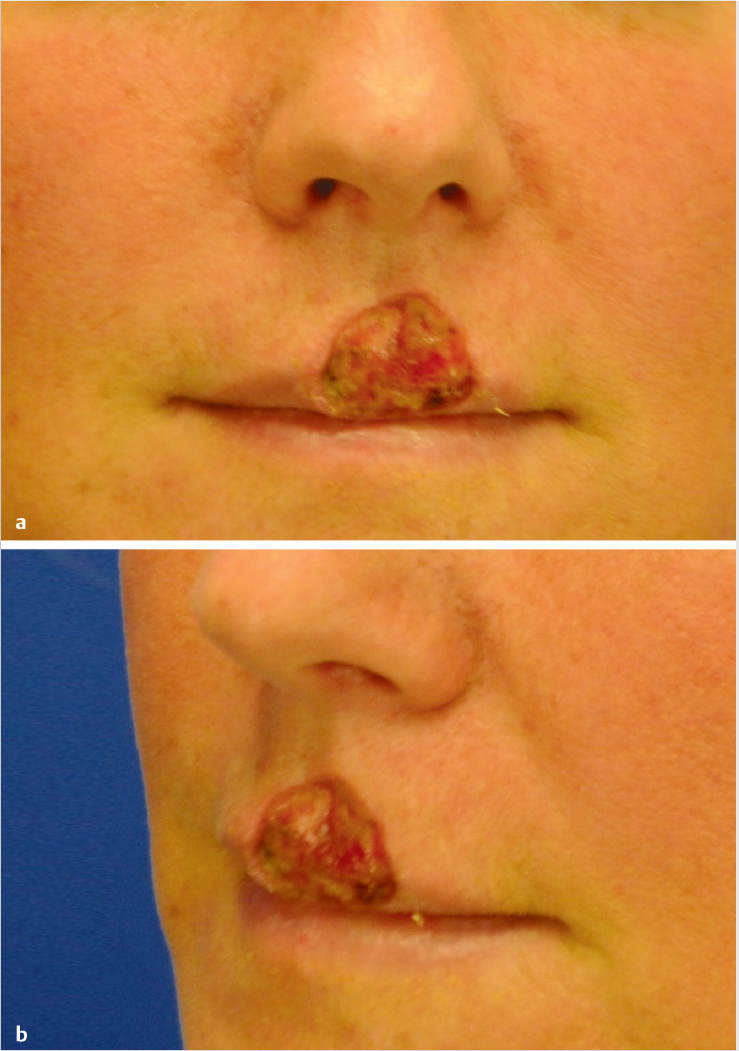
A 2.3 × 2.5-cm partial-thickness defect of central upper lip involving mucosa, vermilion, and cutaneous lip.
Involves multiple critical structures: Cupid′s bow, philtral dimple, and philtral columns bilaterally.
Orbicularis oris muscle intact.
Work-up
History
History of sun exposure.
Personal and family history of skin cancer.
Genetic conditions: Xeroderma pigmentosum, Gorlin (nevoid basal cell) syndrome, albinism.
History of radiation therapy
Organ transplantation: Squamous cell carcinoma is the most common cancer in solid organ transplant recipients
Physical examination
Full-body examination of integument.
Lymph node examination to rule out metastatic disease.
Diagnostic studies
If patient presents initially without resection, a biopsy should be performed at the time of evaluation to establish a diagnosis.
Full-thickness incisional versus excisional biopsies may be performed. Avoid shave biopsies.
Treatment
Consider Mohs surgery, if available.
Allows examination of ~ 100% of surgical margins; highest cure rates.
Board examiner may require that you excise this yourself.
Excision (Table 6.1)
Basal cell carcinoma:
Standard margin is 2-5 mm
Larger margin for high risk types (poorly defined borders, recurrent, perineural invasion, aggressive growth pattern)
Radiation therapy can be used for non-surgical candidates
Squamous cell carcinoma: Most common type in lip, > 90% occur on lower lip.
4 mm margins for low risk lesions: Well/moderately differentiated, well defined borders, trunk/extremity lesions > 2 cm.
6 mm margins for high risk lesions: Poorly differentiated, poorly defined borders, perineural/vascular involvement, Clark level IV or V, recurrent, high risk locations (mask area of face, hands/feet, genitalia)
Enlarged lymph nodes should be evaluated for metastases with FNA or core needle biopsy.
Radiation therapy can be used for non-surgical candidates
Melanoma: Margins determined by Breslow thickness.
In situ: 5 mm.
< 1 mm: 1-2 cm
1 to 2 cm.
2.1 to 4 mm: 2 cm.
> 2 cm: 2 cm.
Stage Ib (0.76-1 mm thick with ulceration or mitotic rate > = 1 per mm2) or stage II melanoma (> 1 mm thick) may require sentinel lymph node biopsy (ENT or surgical oncology consultation). If lymph nodes are positive, neck dissection is performed.
Stage III melanoma (positive lymph nodes) may require interferon (medical oncology consultation).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


