Key Words
pigmentation, café-au-lait macules, erythema ab igne, melasma, lentigo, vitiligo, pityriasis alba, hydroa, sun damage, porphyrias, polymorphous light eruption
Photobiology
Sunlight has profound effects on the skin and is associated with a variety of diseases ( Boxes 19.1 to 19.3 , Table 19.1 ). Ultraviolet (UV) light causes most photobiologic skin reactions and diseases. The accepted unit for measurement of the wavelength of light is the nanometer (nm). The solar radiation that reaches the earth is a continuous spectrum consisting of wavelengths of electromagnetic energy greater than 290 nm. By convention, UV light is divided into UVA (320 to 400 nm; long wave, black light), UVB (290 to 320 nm; middle wave, sunburn), and UVC (100 to 290 nm; short wave, germicidal). UVA is further subdivided into two regions: short-wave UVA, or UVA II (320 to 340 nm); and long-wave UVA, or UVA I (340 to 400 nm). The ratio of UVA to UVB is 20:1, and two thirds of this UVA is UVA I. Eighty percent of UVB radiation and 70% of UVA radiation occur between the hours of 10 AM and 2 PM. More than 90% of UV radiation may penetrate clouds. UV radiation generates reactive oxygen species that damage skin.
Idiopathic
Polymorphous light eruption
Actinic prurigo
Hydroa vacciniforme
Hydroa aestivale
Chronic actinic dermatitis
Solar urticaria
Degenerative and Neoplastic
Actinic damage
Actinic keratosis
Basal cell carcinoma
Squamous cell carcinoma
Malignant melanoma
Secondary to exogenous agents
Phototoxicity: contact and systemic
Photoallergy: contact and systemic
Drug eruptions
Metabolic
Erythropoietic porphyria
Erythropoietic protoporphyria
Porphyria cutanea tarda
Variegate porphyria
Photoexacerbated Dermatoses
Autoimmune Diseases
Lupus erythematosus
Dermatomyositis
Pemphigus
Pemphigus foliaceus
Bullous pemphigoid
Genodermatoses
Familial benign chronic pemphigus
Keratosis follicularis (Darier disease)
Bloom syndrome
Rothmund–Thomson syndrome
Kindler syndrome
Cockayne syndrome
Xeroderma pigmentosum
Trichothiodystrophy
Hartnup disease
Infectious Disease
Herpes simplex labialis
Nutritional Deficiencies
Pellagra
Pyridoxine deficiency
Primary Dermatologic Diseases
Atopic dermatitis
Transient acantholytic dermatosis
Disseminated superficial actinic porokeratosis
Lichen planus actinicus
Psoriasis
Reticular erythematous mucinosis
Acne rosacea
Acne
Darier disease
Hailey–Hailey disease
Childhood
- •
Erythropoietic protoporphyria (burning pain, increased protoporphyrin levels in red blood cells)
- •
Hydroa vacciniforme (scar formation)
- •
Juvenile spring eruption (lesions on ears in spring)
- •
Polymorphous light eruption (itchy lesions in V area of chest and extremities)
Adulthood
- •
Drug-induced photosensitivity (sun-exposed areas)
- •
Lupus erythematosus
- •
Polymorphous light eruption (females with itchy lesion in V area of neck and elsewhere)
- •
Porphyria cutanea tarda
- •
Solar urticaria (lesions appear within 5–10 min and disappear in 1–2 hours)
Old Age
- •
Chronic actinic dermatitis (persistent redness of face in elderly man)
- •
Dermatomyositis
- •
Drug-induced photosensitivity (sun-exposed areas)
Ataxia telangiectasia
Bloom syndrome
Cerebro-oculo-facial-skeletal syndrome
Cockayne syndrome
Darier disease
De Sanctis–Cacchione syndrome
Dermatomyositis
Fanconi anemia
Hydroa vacciniforme
Lupus erythematosus
Pellagra
Pseudoporphyria
Rothmund–Thomson syndrome
Solar urticaria
Trichothiodystrophy
UV-sensitive syndrome
Xeroderma pigmentosum
XPF-ERCC1 progeroid syndrome
UV, ultraviolet.
| Disorder | Action Spectrum | Protection Required |
|---|---|---|
| Polymorphous light eruption | 290–365 nm | Broad spectrum |
| Porphyrias | 400–410 nm | Physical blocking agent |
| Solar urticaria | 290–515 nm | Broad spectrum |
| Lupus erythematosus | 290–330 nm | UVB most important, also UVA |
| Xeroderma pigmentosum | 290–340 nm | Broad spectrum |
UVA.
UVA causes immediate and delayed tanning and contributes little to erythema and burning. It is constant throughout the day and throughout the year. The longer wavelengths of UVA can penetrate more deeply, reaching the dermis and subcutaneous fat. Chronic exposure to UVA radiation causes the connective tissue degeneration seen in photoaging, photocarcinogenesis, and immunosuppression. Photocarcinogenesis is augmented in patients who are immunosuppressed for organ transplantation. UVA augments the carcinogenic effects of UVB. UVA penetrates window glass and interacts with topical and systemic chemicals and medication. It produces photoallergic and phototoxic reactions.
UVB.
UVB produces the most harmful effects and is greatest during the summer. Snow and ice reflect UVB radiation. UVB delivers a high amount of energy to the stratum corneum and superficial layers of the epidermis and is primarily responsible for sunburn, suntan, inflammation, delayed erythema, and pigmentation changes. It produces tanning more efficiently than does UVA. Chronic effects include photoaging, immunosuppression, and photocarcinogenesis. It is most intense when the sun is directly overhead between 10 AM and 2 PM. UVB is absorbed by window glass. Prior exposure to UVA enhances the sunburn reaction from UVB.
UVC.
UVC is almost completely absorbed by the ozone layer and is transmitted only by artificial sources such as germicidal lamps and mercury arc lamps.
Sun-Damaged Skin
Sunlight–Skin Interaction.
DNA is mutated by UVB. Absorption of UVA leads to the release of reactive oxygen species that cause oxidation of lipids and proteins that affect DNA repair, produce dyspigmentation, and cause photoaging and carcinogenesis.
Aging Versus Sun Damage.
Sun exposure is the major cause of the undesirable skin changes often inaccurately perceived as aging. These changes, known as photoaging, are caused primarily by repeated sun exposure and not by the passage of time. Many of the clinical signs attributed to aging are actually manifestations of solar damage. The two processes are biologically different. The difference can best be demonstrated to patients by comparing the appearance of the skin under the arm near the axillae with the sun-exposed surface of the lower arm.
Normal Aging.
The skin begins to show signs of aging by ages 30 to 35. Aged skin is thin, fragile, and inelastic. The epidermis becomes thin. There is a gradual loss of blood vessels, dermal collagen, fat, and the number of elastic fibers. There is a reduction in the density of hair follicles, sweat ducts, and sebaceous glands, resulting in a reduction in perspiration and sebum production. Potent steroids should not be used on aged skin with few blood vessels because the steroids are not cleared from the skin as easily as in younger persons.
The skin becomes atrophic and fragile when subcutaneous tissue is lost. Elastic fibers are responsible for the elasticity and resilience of the skin. In normal aging, there is loss and fragmentation of elastic fibers, which result in fine wrinkles that resemble crumpled cigarette paper. These shallow wrinkles disappear by stretching. The skin is easily distorted, but it recoils slowly.
Photoaging.
Photoaging refers to those skin changes superimposed on intrinsic aging by chronic sun exposure ( Box 19.4 ). Unprotected, chronically exposed children can acquire significant actinic damage by the time they reach age 15. The effects of this damage may become apparent after age 20. Sun-damaged skin is characterized by elastosis (a coarsening and yellow discoloration of the skin), irregular pigmentation, roughness or dryness, telangiectasia, atrophy, deep wrinkling, follicular plugging, and a variety of benign and malignant neoplasms. The epidermis thickens. Although many different cells are affected, it is the elastotic material that accounts for the most striking effects of sun damage.
Texture Changes
Solar elastosis
Thickened, wrinkled, yellowish skin
Atrophy
Thinning of the skin; fine wrinkling, prominent blood vessels, easy bruising and tearing of the skin, often with many linear scars
Wrinkles
Deep – do not disappear by stretching
Posterior neck sun damage (cutis rhomboidalis nuchae)
Thickened skin is crisscrossed by deep lines creating rhomboidal patterns
Vascular Changes
Diffuse erythema
Most apparent in fair-skinned people
Ecchymoses and stellate pseudoscars
Bleeding into the skin follows minor trauma – only on exposed surfaces of the back of the hands and arms; associated with atrophy, ease of skin tearing, and linear scars
Telangiectasias
Cheeks, nose, and ears
Venous lake
Round, purple, ectatic vessels – lower lips and ears
Pigmentation Changes
Freckles
Small, oval, brown macules – primarily on the face
Lentigines
Large brown macules – face, back of the hands, arms, chest, upper back
Guttate hypomelanosis
Discrete, round, white macules – lower legs and arms
Brown and white pigmentation (irregular)
Deep brown with areas of hypopigmentation
Poikiloderma of Civatte
Reddish brown reticulated pigmentation with telangiectasias, atrophy, and prominent hair follicles – chest and neck
Papular Changes
Nevi
More numerous on sun-exposed surfaces in predisposed individuals
Yellow papules (solar elastosis)
Dull to bright yellow papules that may coalesce to form plaques
Seborrheic keratosis
Discrete superficial (stuck-on) lesions – more numerous in sun-exposed areas; flat on extremities, elevated on the trunk
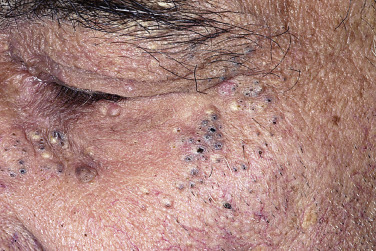
Comedones and cysts around the eyes (Favre–Racouchot syndrome)
Solar elastosis is a sign highly characteristic of severe sun damage ( Figs. 19.1 and 19.2 ![]() ). There is massive deposition in the upper dermis of an abnormal, yellow, amorphous elastotic material that does not form functional elastic fibers. This altered connective tissue does not have the resilient properties of elastic tissue.
). There is massive deposition in the upper dermis of an abnormal, yellow, amorphous elastotic material that does not form functional elastic fibers. This altered connective tissue does not have the resilient properties of elastic tissue.

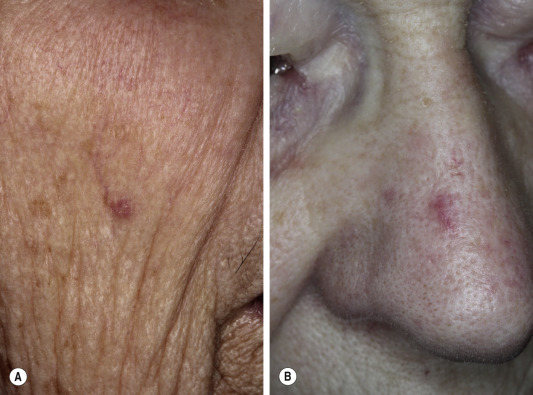
Wrinkling becomes coarse and deep rather than fine, and the skin is thickened ( Fig. 19.3 ). These wrinkles do not disappear by stretching. Sun-induced wrinkling on the back of the neck shows a series of crisscrossed lines ( Fig. 19.4 ) that form a rhomboidal pattern (cutis rhomboidalis nuchae).


Reactive hyperplasia of melanocytes causes persistent pigmentation in the form of freckles, lentigines, and irregular hyperpigmentation and hypopigmentation on the hands, forearms, legs, chest, back, and neck ( Figs. 19.4 and 19.5 ).

Chronic sun exposure disrupts the maturation of keratinocytes, causing scaling, roughness, seborrheic keratosis ( Figs. 19.6 to 19.9 ), actinic keratosis, actinic cheilitis, and squamous cell carcinoma.




Blood vessels diminish in number, and the walls of the remaining vessels become thin. Blood vessels need connective tissue for support. Bleeding occurs with the slightest trauma to the sun-damaged surfaces of the forearms and hands but not to the unexposed surfaces. Haphazard scarring may follow ( Figs. 19.10 and 19.11 ). Making patients aware of this difference convinces them that they do not have a platelet abnormality.


Comedones form about the eyes ( Fig. 19.12 ).
Prevention of Skin Aging.
A study of sunscreen use was performed. Participants assigned to daily sunscreen use applied sunscreen at least 3 to 4 days each week. Those in the daily-use group were less likely to have increased skin aging after 4.5 years than were those in the control group.
Treatment of Photoaging
Photoaging is treated either by applying topical treatments or by resurfacing through chemical peels, dermabrasion, or lasers.
Topical Treatment.
Topical treatments have the following characteristics:
- 1.
They are noninvasive.
- 2.
They are slow to produce changes (latency period is 3 to 6 months).
- 3.
Maintenance of improvements requires continued use.
- 4.
Medication is expensive.
Topical Tretinoin and Tazarotene.
Topical retinoids provide some reversal of photodamaged skin ( Box 19.5 ). Objective improvements in wrinkling are seen after 3 to 6 months. Dyspigmentation (brown spots and mottled hyperpigmentation), surface roughness, and fine wrinkles respond best. The greatest response to therapy occurs during the initial 6 to 9 months.
Fine wrinkling – improved
Coarse wrinkling – improved
Tactile roughness – improved
Lentigines – reduction in number
Freckles – reduction in color
Actinic keratoses – decrease in number
Telangiectasia – did not improve
Cutaneous reaction
Dermatitis – (1 to 10 weeks) xerosis, mild scaling, irritation
Increased pinkness, “rosy glow”
Inflammation – (3+ months) of presumed subclinical actinic keratoses
Repeated applications of retinoids produce a skin reaction resembling irritation. This reaction is characterized by redness and desquamation, signs that correspond histologically to alterations in the stratum corneum and epidermal hyperplasia. Initially patients experience skin tightening and a pink glow. This smoothening occurs within 1 to 2 weeks of treatment. It is the first sign of improvement, and it occurs because the stratum corneum is thinner and more compact, and the epidermal layer is thicker and spongiotic. Increased proliferation of basal keratinocytes eventually doubles the epidermal thickness.
Collagen formation is reduced in photoaged skin and is partly responsible for wrinkle formation. Tretinoin and tazarotene increase collagen levels in photoaged skin; the end result is wrinkle effacement. Effacement of fine wrinkles occurs after 3 to 4 months of tretinoin therapy. The deepest, coarse facial wrinkles are still evident. Despite continued improvement in wrinkle effacement, the epidermal histology reverts to the pretherapy state.
Hyperpigmented lesions are a predominant component of photoaging in Chinese and Japanese persons; tretinoin cream lightens the hyperpigmentation of photoaging in these patients. Tretinoin therapy for individuals with darker skin pigmentation is safe. Postinflammatory dyspigmentation at sites of retinoid dermatitis does not occur in black and Asian patients.
Retinoid Application Procedures.
The response to retinoids may be dose dependent; higher concentrations may be more effective. Many patients experience a “retinoid dermatitis” with erythema and peeling. To achieve maximum clinical improvement of photoaged skin, it is not necessary to push retinoid use to the point that brisk retinoid dermatitis develops. A 48-week regimen of once-daily treatment with medication, followed by treatment three times weekly for an additional 24 weeks, maintains and, in some cases, even enhances the improvements in photoaged skin. Treatment on a once-a-week basis with retinoids is less effective in sustaining the clinical improvement achieved by the initial treatment regimen of tretinoin on a once-daily basis. Some reversal of the beneficial effects of tretinoin treatment is observed after discontinuation of therapy for 24 weeks, which indicates the need to continue tretinoin therapy to maintain clinical improvement.
Begin with nighttime application. Start treatment with cream-based tretinoin (0.025%), emollient-based tretinoin, or cream-based tazarotene. A gradual introduction to treatment using every-other-day application is appropriate for patients with sensitive skin (usually type I; Table 19.2 ), followed by more frequent applications when patients accommodate. Apply moisturizing cosmetics or lubricating lotions if dryness occurs. Maximum response occurs after 8 to 12 months of treatment; thereafter application frequency should be reduced to three or four times a week to maintain improvement.
| Type * | Characteristic ** | Routine Day and Outdoor Activity (Waterproof) Recommended SPF |
|---|---|---|
| I | Always burns easily, never tans
| SPF 30 or above is recommended for all skin types |
| II | Burns easily, tans slightly
| |
| III | Sometimes burns, then tans gradually and moderately
| |
| IV | Burns minimally, always tans well
| |
| V | Burns rarely, tans deeply
| |
| VI | Almost never burns, deeply pigmented
|
* Reflects color of unexposed buttock skin. Skin types I to III are white, type IV is white or faintly brown, type V is brown, and those with skin type VI have dark brown or black buttock skin.
** Based on the first 30 to 45 minutes of sun exposure after winter season or no sun exposure.
Sun Protection During Use.
Encourage the daily use of sunscreens. Increased “photosensitivity” during tretinoin use is not an accelerated sunburn response. No increased risk of photocarcinogenesis has been detected in humans.
Tretinoin Use and Pregnancy.
The data on routine clinical use of topical tretinoin indicate that there is no increased risk during pregnancy. However, spontaneous malformation of the fetus occasionally occurs in “normal” pregnancies. It may therefore be prudent to postpone tretinoin therapy for patients who are actively trying to conceive, to avoid wrongful blame for congenital defects that may occur by chance. Tazarotene cream is a pregnancy category X medication and is contraindicated during pregnancy.
Estrogen Replacement.
Statistically significant reductions in dry skin and skin wrinkling occur with estrogen replacement.
Suntan and Sunburn
Light-induced skin changes depend on the intensity and duration of exposure and genetic factors.
Suntan.
A tan protects the body from photoinjury, but UV-induced injury must occur to produce a tan. Therefore intentional suntanning is unwise. Repeated brief exposures sufficient to induce tanning add to long-term damage. For a given individual, the deeper the tan, the more skin damage is sustained in achieving the tan.
Tanning follows moderate and intense sun exposure and occurs in two stages. The first stage, immediate pigment darkening (IPD), is caused primarily by UVA. The skin becomes brown while exposed but fades rapidly after exposure. IPD is caused by a photochemical change in existing melanin, not by an increase in melanin. A lasting tan requires the synthesis of new melanin; a more lasting tan becomes visible within 72 hours.
Tanning Parlors.
Artificial and natural UV sources will damage the skin to a similar degree and hence carry the similar photoaging effects and skin cancer risks. Artificial UV sources from tanning parlors are capable of delivering large amounts of radiation in a short amount of time, thereby increasing the risk of nonmelanoma and melanoma skin cancer.
Sunburn.
Forty-three percent of white U.S. children experienced one or more sunburns during the year. The sunburn reaction occurs in stages. With sufficient exposure, erythema appears within minutes (immediate erythema), fades, and then reappears and persists for days (delayed erythema). Vascular permeability of varying degrees results in edema and blisters. Desquamation occurs within a week. Systemic and topical corticosteroids have little or no clinically important effect on the sunburn reaction. Systemic and topical nonsteroidal antiinflammatory drugs (NSAID), when used at dosages to achieve optimal serum levels for antiinflammatory effect, only result in an early and mild reduction of UVB-induced erythema. Sunburn is best treated with cool, wet compresses. Topical anesthetic preparations that contain lidocaine provide some relief. Benzocaine, incorporated into some sunburn preparations, is a sensitizer and should be avoided. Protection with sunscreens can, if used properly, prevent burning in even fair-skinned individuals.
Sun Protection
UV-induced damage to collagen and elastic fibers and a number of skin cancers can be greatly reduced by high sun protection factor sunscreens and other methods to reduce sun exposure ( Box 19.6 ). Sun protection may allow for repair of damaged skin. New collagen and elastin may form, and precancerous changes may regress. Substantial lifetime sun exposure occurs with brief incidental exposures such as working outdoors, participating in recreational activities, and walking outside for lunch. Daily application of sunscreen or a moisturizer with sun protection factor minimizes the deleterious effects of incidental sun exposure.
Use a sunscreen sun protection factor (SPF) of at least 30 or above
Apply sunscreen 15 to 30 minutes before going outdoors
Reapply sunscreen every 2 hours or after exposure to water
Apply sunscreen in thick layers
Avoid peak sunlight hours (10 AM to 3 PM)
Wear dark, loose, dry clothing with a tight weave, wide brim hat, and long-sleeved shirt, pants
Methods of Sun Protection.
Natural protection is provided by the stratum corneum and the skin pigment melanin. People vary widely in their natural ability to tan or burn. A sun-reactive skin typing system has been devised to classify individuals according to their ability to tan or burn. These categories (see Table 19.2 ) are useful guides for devising programs for sun protection.
Recommendations for minimizing sun exposure are listed in Box 19.6 . Sunburns are particularly harmful, and great emphasis should be placed on preventing burns. Patients frequently relate that permanent freckling occurred on the upper back after one severe burn. Winter vacations in hot sunny climates appear to be very damaging, if the skin is burned. Total sun exposure during a lifetime is greatest on the face, back of the neck, bald head, upper chest, forearms, backs of the hands, and exposed lower legs. The effects of sunlight can readily be appreciated by comparing the lateral (sun-exposed) surfaces with the medial (sun-protected) surfaces of the forearms of older individuals.
Clothing.
Clothing is the best protection. Weave tightness and fabric type determine the potential for photoprotection. Stretched or wet fabric is less effective. Darker colors provide greater protection than lighter colors. Some manufacturers market special clothing with sun protection factor (SPF) ratings, including Solumbra (Sun Precautions, Seattle, WA, www.sunprecautions.com ).
Protecting the Young.
Significant sun exposure occurs during the early years of life when children spend hours playing outside. A study showed that regular use of a sunscreen with an SPF of 15 during the first 18 years of life reduces the lifetime incidence of basal and squamous cell carcinoma by 78%. All children should be protected with high-number SPF sunscreens. One-piece bathing suits that cover the trunk, upper arms, and legs are ideal for children.
Sunscreens.
Sunscreens are topical agents that protect the skin from UV light. Guidelines for their application are listed in Box 19.6 . Sunscreens should not be used as a means of allowing more time in the sun; this negates their beneficial effects.
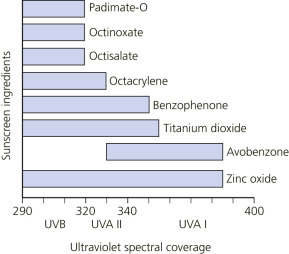
Sunscreens are topical agents that absorb, scatter, or reflect ultraviolet radiation (UVR) and visible light. UVA agents absorb radiation in the spectral range of 320 to 400 nm. UVB agents absorb radiation in the range of 290 to 320 nm ( Fig. 19.13 ). Food and Drug Administration (FDA)-approved active sunscreen ingredients are listed in Tables 19.3 and 19.4 . The proper use of sunscreen can prevent the development of melanoma.
| Active Ingredients | Maximum Concentration (%) | Peak Absorption λ (nm) | UV Action Spectrum |
|---|---|---|---|
| ORGANIC FILTERS | |||
| UVA Filters | |||
| Benzophenones | |||
| Oxybenzone (benzophenone-3) | 6 | 288, 325 | UVB, UVA II |
| Sulisobenzone (benzophenone-4) | 10 | 366 | UVB, UVA II |
| Dioxybenzone (benzophenone-8) | 3 | 352 | UVA, UVA II |
| Dibenzoylmethanes | |||
| Avobenzone (butyl methoxydibenzoylmethane, Parsol 1789) | 3 | 360 | UVA I |
| Anthralates | |||
| Meradimate (menthyl anthranilate) | 5 | 340 | UVA II |
| Camphors | |||
| Ecamsule * (terephthalylidene dicamphor sulfonic acid, Mexoryl SX) | 10 | 345 | UVB, UVA |
| UVB Filters | |||
| Aminobenzoates (PABA derivatives) | |||
| PABA ( para -aminobenzoic acid) | 15 | 283 | UVB |
| Padimate-O (octyl dimethyl PABA) | 8 | 311 | UVB |
| Cinnamates | |||
| Cinoxate (2-ethoxyethyl p -methoxycinnamate) | 3 | 289 | UVB |
| Octinoxate (octyl methoxycinnamates [OMC]) | 7.5 | 311 | UVB |
| Salicylates | |||
| Octisalate (octyl salicylate) | 5 | 307 | UVB |
| Homosalate (homomenthyl salicylate) | 15 | 306 | UVB |
| Trolamine salicylate (triethanolamine salicylate) | 12 | UVB | |
| Others | |||
| Octocrylene | 10 | 303 | UVB, UVA II |
| Ensulizole (phenylbenzimidazole sulfonic acid) | 4 | 310 | UVB |
| INORGANIC FILTERS | |||
| Titanium dioxide | 25 | UVB, UVA † | |
| Zinc oxide | 25 | UVB, UVA † | |
* Only as a component of certain approved sunscreen formulations sanctioned under the new drug application (NDA).
| Active Ingredients | Maximum Concentration (%) | Peak Absorption λ (nm) | UV Action Spectrum |
|---|---|---|---|
| Methylenebis(benzotriazolyl)tetramethylbutylphenol (MBBT) (Tinosorb M) (Bisoctrizole) | 10 | 305, 360 | UVB, UVA |
| Bis(ethylhexyloxyphenol)methoxyphenyltriazine (BEMT) (Tinosorb S) (Bemotrizinol) | 10 | 310, 343 | UVB, UVA |
| Ethylhexyl triazone (EHT) (octyl triazone) | 5 | 314 | UVB |
| Isoamyl methoxycinnamates (Amiloxate) | 10 | 310 | UVB |
| Methylbenzylidene camphor (Enzacamene) | 4 | 300 | UVB |
| Diethylhexyl butamido triazone (Iscotrizinol) | 3 | 312 | UVB |
| Terephthalylidene dicamphor sulfonic acid (Ecamsule) | 10 | 345 | UVB, UVA |
| Drometrizole trisiloxane (Mexoryl XL) | 15 | 303, 344 | UVB, UVA |
Sunscreen Labeling.
The term “broad spectrum” may appear on the product if FDA criteria are met. Labels can only contain either the statement “water resistant (40 minutes)” or the statement “very water resistant (80 minutes).” This claim is to be placed at the front of the product package. The time stated on the label reflects the actual water-resistant testing that is required to be done: SPF value needs to be determined after test subjects are immersed in a whirlpool for 2 times 20 minutes or 4 times 20 minutes.
User Application Amounts.
Sunscreen SPFs are determined by testing at an application density of 2 mg/cm 2 . Typical application densities by most consumers range from 0.5 to 1 mg/cm 2 . Therefore the actual protection received is often substantially less than that promised by the label. Encourage people to apply a substantial amount of product at least every 2 hours to obtain maximum benefit. High-SPF (50 SPF) sunscreens may provide more adequate protection even when applied by consumers in inadequate amounts.
Physical Sunscreens.
Physical sunscreens (referred to as inorganic or nonchemical sunscreens) are composed of particles that scatter and reflect light. Physical blocking agents, such as zinc oxide and titanium dioxide, are composed of particles of a size that scatter, reflect, or absorb solar radiation. Twenty percent zinc oxide, or 20% titanium dioxide, reduces transmittance in the UVA and visible ranges to a maximum of approximately 20%. Newer micronized preparations that are suspensions are more cosmetically acceptable.
Chemical Sunscreens.
Chemical sunscreens (organic agents) absorb radiation. Newer broad-spectrum chemical sunscreens include a combination of chemicals that absorb both UVB and UVA radiation.
Water-Resistant Sunscreens.
Substantivity is the characteristic of a sunscreen that reflects how effectively the advertised degree of protection is maintained under adverse conditions, including repeated water exposure or sweating. According to the FDA, a sunscreen is declared water-resistant if it can maintain its original SPF after two 20-minute immersions. A sunscreen is very water-resistant if it retains its protective integrity after four 20-minute immersions.
Sun Protection Factor.
The effectiveness of sunscreens is expressed as the SPF. The SPF is defined as the ratio of the least amount of UVB energy (minimum erythema dose) required to produce a minimum erythema reaction through a sunscreen product film to the amount of energy required to produce the same erythema without any sunscreen application. For an individual who wears a sunscreen with an SPF of 15, 15 times longer than usual is required to develop erythema. The SPF for commercially available products is derived from tests with application of a uniform amount of sunscreen that is thicker than most individuals routinely use. A substantial amount of sunscreen must be applied to obtain a full SPF rating.
Choice of Sunscreen Strength.
A sunscreen with an SPF of 30 or greater is recommended under most conditions. Sun protection does not increase proportionally with the designated SPF. In the higher range of SPFs, the differences become less meaningful. An SPF of 15 indicates 93% protection; an SPF of 34 indicates 97% protection. Newer sunscreens contain Mexoryl or Helioplex. Avobenzone is one of the best UVA absorbers, while oxybenzone is a very good UVB absorber with some UVA absorbency. Together with the Helioplex or Mexoryl SX stabilizing technology, these two sunscreen ingredients complement each other for high, broad-spectrum, and photostable coverage.
Frequency of Use.
The majority of lifetime sun exposure occurs during multiple brief exposures that are not intended to produce tanning; therefore daily sun protection should be encouraged. People who sunburn easily or those who have light complexions or sun-sensitivity disorders should use a high SPF sunscreen every day, all year, particularly if they live in more equatorial latitudes. Sunscreens should be applied once in the morning and reapplied every 2 hours or after swimming and heavy exercise. Encourage people to have sunscreens available in the bathroom and to make morning application part of their daily ritual. Sunscreen may fail to prevent sunburn if it is washed off during swimming or if it is not applied to all exposed skin. The protection against sunburn afforded by a reapplication of sunscreen relative to a single application is significant. Compared with the first application, the second sunscreen application affords 3.1 times more protection against minimal UVR-induced erythema. The combined effect of two sunscreen applications gives 2.5 times better protection from UVR than does a single sunscreen application.
Glass Filters.
Glass filters UVB radiation but transmits UVA radiation. Protective coatings applied to glass can block UVA radiation. LLumar window film ( www.llumar.com ) is a microthin film that is installed onto home and automobile glass surfaces to provide solar protection. It blocks 99% of the UV rays. Glass filters are indicated for patients with multiple skin cancers, transplant patients with skin cancers, and patients with photosensitive dermatoses.
Adverse Reactions to Sunscreens.
Allergic reactions to preservatives or fragrances occur more frequently than to the active ingredients. Irritation to creams is much more common than allergy to a component. Burning or stinging may be experienced in the eye area. Sunscreen active ingredients may cause photocontact allergic reactions. Most patients who develop photocontact dermatitis to sunscreens are patients with photodermatides.
Vitamin D Levels.
Sun protection is important to prevent skin malignancies. Vitamin D is formed in the skin through the action of the sun. Vitamin D deficiency may induce various types of cancer, bone diseases, autoimmune diseases, hypertension, and cardiovascular disease. Strict sun protection can cause vitamin D deficiency, although there is no evidence that normal sunscreen use results in vitamin D deficiency. Vitamin D status can be measured. Balanced recommendations on sun protection have to ensure an adequate vitamin D status. Twenty minutes of exposure each day to an area the size of the trunk may be reasonable until guidelines are established.
Sunless or Self-Tanning Lotions.
Sunless or self-tanning lotions contain dihydroxyacetone (DHA), which darkens the skin by staining. The preparations are nontoxic. The site of action of DHA is the stratum corneum. Staining of skin occurs when DHA combines with free amino groups in skin proteins (keratin) in the stratum corneum to form brown products called melanoidins. Little to no sunscreen protection is provided by their use. Some products are formulated with standard sunscreens.
The newer preparations do not produce the orange color that occurred from the older formulations.
Polymorphous Light Eruption
Polymorphous light eruption (PMLE) is the most common idiopathic light-induced skin disorder. PMLE is a chronic condition that may worsen with time, it occurs more commonly in women in temperate climates and is not associated with an increased risk of lupus erythematosus. Not only does the clinical picture vary, but also symptoms may vary over the years. There are several morphologic subtypes, but individual patients tend to develop the same type each year. Lesions usually heal without scarring. The eruption appears first on limited areas but becomes more extensive during subsequent summers. Most people with PMLE have exacerbations each summer for many years; a few have temporary remissions. The disease may begin at any age. The amount of light exposure needed to elicit an eruption varies greatly from one patient to another. Patients can tolerate a certain minimum exposure time, such as 30 minutes, after which the eruption appears. Light sensitivity decreases with repeated sun exposure; this phenomenon is referred to as hardening. The eruption may cease to appear after days or weeks of repeated sun exposure. Those exposed to sunlight all year rarely acquire PMLE. Most patients have symptoms 2 hours after exposure. In a 7-year follow-up study, 57% of patients reported a decrease in sun sensitivity, including 11% in whom the PMLE totally cleared; none of the patients developed systemic lupus erythematosus.
Etiology.
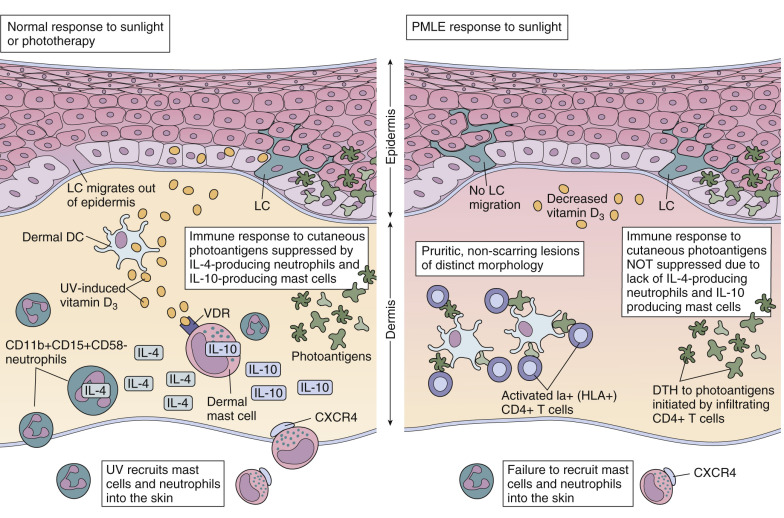
The precise underlying mechanism of PMLE is not known. Patients with PMLE may not develop the normal cutaneous immune suppression, seen after UVR exposure. When the skin is exposed to UVR, cells are altered at the DNA and protein level. These organic cellular alterations may be recognized by the immune system as foreign, eliciting the autoimmune reaction seen in PMLE. Normal individuals do not likely react to these altered cellular components because their skin has been locally immunosuppressed by UVR ( Fig. 19.14 ![]() ).
).
Hereditary PMLE (Actinic Prurigo).
Hereditary PMLE eruption occurs in the Inuit of North America and in Native Americans of North, Central, and South America. Its transmission appears to be autosomal dominant with incomplete penetrance and variable expressivity. In northern latitudes, the eruption appears on sun-exposed areas of the body as early as March and persists through October. The face is the most commonly involved area. Intensely itchy papules, plaques, and nodules, along with excoriations and scars, are present on the sun-exposed area ( Fig. 19.15 ). The onset is usually in childhood. The majority of patients are sensitive to UVA light. The younger ages of onset (up to 20 years of age) are associated with cheilitis and more acute eruptions and are more likely to improve over 5 years. Those who develop actinic prurigo as adults (21 years of age and older) tend to have a milder and more persistent dermatosis.

Clinical Presentation.
Women are affected more often than are men. The mean age at onset is 34 years (5 to 82 years). For men the mean age is 46 years and for women, 28 years. The most common initial symptoms are burning, itching, and erythema. The eruption usually lasts for 2 or 3 days, but in some cases it does not clear until the end of summer. Many patients experience malaise, chills, headache, and nausea starting approximately 4 hours after exposure but lasting only 1 or 2 hours. The most commonly involved areas are the V of the chest (the area exposed by open-necked shirts), the backs of the hands, the extensor aspects of the forearms, and the lower legs of women. Reports vary about the wavelength of light responsible for inducing lesions. The wavelength of light necessary to elicit the eruption varies with each patient. Many react to UVB, others to UVA, or some to both.
Clinical Subtypes.
There are a number of clinical types of PMLE.
Papular Type.
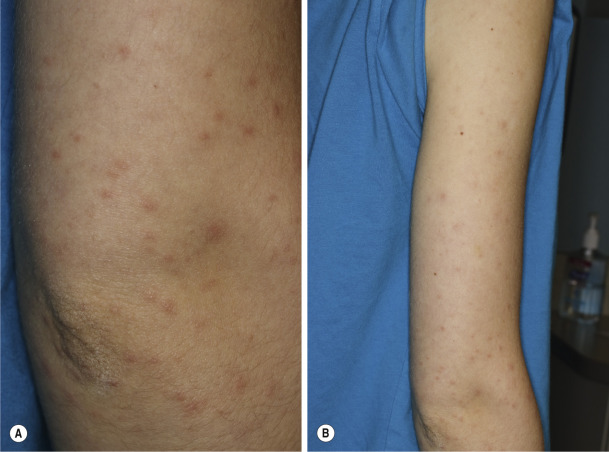
The papular type is the most common form ( Figs. 19.16 and 19.17 ). Small papules are disseminated or densely aggregated on a patchy erythema. A pinpoint papular variant has been described.


Plaque Type.
The plaque type is the second most common pattern. Plaques may be superficial or urticarial. They may coalesce to form larger plaques and at times are eczematous ( Figs. 19.18 and 19.19 ).


Papulovesicular Type.
The papulovesicular type is less common. It occurs primarily on the arms, lower limbs, and V area of the chest and usually begins with urticarial plaques from which groups of vesicles arise ( Fig. 19.20 ). Itching is common and is usually moderate or marked. This form occurs almost exclusively in women.

Eczematous Type.
Erythema, papules, scale, and sometimes vesicles occur. Eczematous lesions occur almost exclusively in men.
Erythema Multiforme Type.
Erythema multiforme–type lesions and distribution are similar to those of classic erythema multiforme, with lesions most frequent on the backs of the hands and extensor forearms.
Hemorrhagic Type.
The hemorrhagic type may first appear as hemorrhagic papules or purpura. This form is rare.
Spring and Summer Eruption of the Elbows.
Pruriginous, erythematous–edematous papules and plaques are located on both elbows.
Differential Diagnosis.
The papular form resembles atopic dermatitis. PMLE is less pruritic and occurs in a sun-exposed distribution, not in crease areas, as does atopic dermatitis.
Systemic and discoid lupus erythematosus plaque–like lesions and histologic features may be identical to those of PMLE. The characteristic direct and indirect immunofluorescence patterns of lupus erythematosus clarify the diagnosis.
Diagnosis.
The histologic features are not diagnostic. Immunofluorescence is negative. Phototesting is not essential but, when performed, must include both UVB and UVA testing.
Treatment
Topical steroids, antimalarial agents, and beta-carotene are often disappointing. Prophylactic therapy with sunscreens is partially effective. In the case of minor complaints, patients can become disease free by using sunscreens and gradually increasing sun exposure in the spring. Phototherapy and photochemotherapy are most effective. Table 19.5 summarizes treatments for PMLE.
| Agent | Mechanism |
|---|---|
| Sunscreens | UVA+UVB photoprotection |
| Photohardening | Melanization in the skin Restoring UV-induced LC depletion and neutrophil infiltration into skin Restoration of an abnormal chemotactic potential of neutrophils Increasing 25-hydroxyvitamin D 3 serum levels |
| Chloroquine | Immunomodulatory and antiinflammatory properties |
| Oral Polypodium leucotomos extract | Antioxidant and antiinflammatory effects |
| Nutritional supplement containing lycopene, beta-carotene and Lactobacillus johnsonii | Antioxidant effects |
| Topical DNA repair enzymes | Potential elimination of an antigenic trigger |
| Topical vitamin D 3 | Immunomodulating and -suppressive properties similar to UVR |
| Afamelanotide | Melanization in the skin |
Topical and Oral Steroids.
Short, intermittent 3- to 14-day courses of group I to V topical steroids are effective. Group II through V topical steroids reduce pruritus and hasten resolution. Short courses of oral steroids are useful for very itchy, widespread eruptions or for patients who flare during a course of phototherapy or photochemotherapy.
Protection.
Sun exposure during times of maximum intensity (between 10 AM and 2 PM) should be avoided. Sunscreens with maximum sun-protecting factors should be used. The most sensitive patients are advised about filters for car windows (LLumar UV shield, www.llumar.com ) and fluorescent lighting at home.
Desensitization With Phototherapy.
The sensitivity of human skin to UV radiation decreases after exposure to UV radiation. Adaptation occurs by exposing patients to small and controlled doses of light. Doses small enough not to cause any abnormal reaction but large enough to increase the tolerance of the skin to light are used. A regular series of such exposures, with small increments in exposure time, can result in an appreciable tolerance. Increments of 10% per exposure are given as long as there are no adverse reactions. This is the so-called phenomenon of hardening. This practice is safe; therefore controlled exposure to sunlight or artificial UV light sources should be the first type of treatment. Patients treated with UVB or narrowband UVB (NB-UVB) in the dermatologist’s office receive five exposures per week for 3 weeks in the spring, with gradually increasing exposure doses. Hardening may also be accomplished with either UVA (340 to 400 nm) or UVA and UVB (300 to 400 nm) (10 exposures to UV light). Commercial “sun beds” are not recommended because they are most likely to provoke the PMLE rash. Prophylactic UVB may sometimes trigger the eruption, particularly in severely affected subjects, necessitating concurrent systemic corticosteroid therapy.
Psoralen UVA (PUVA).
Treatment can be acquired in the dermatologist’s office by using artificial UVA light and 8-methoxypsoralen (PUVA). A remission can be obtained for most patients by treatment two or three times each week for 4 to 12 weeks in the early spring. PUVA therapy protects temporarily, and repeated sun exposures are required to maintain protection. A number of patients remain protected for 2 to 3 months, even after pigmentation has faded. Topical steroids should be applied if the disease is activated by treatment. Maximum protection is reached 3 weeks after a 1 week course of treatment, and a single course offers a minimum of 6 weeks of protection. The course can be repeated each month during the spring and summer months if needed. Protective glasses such as NoIR should be worn for the remainder of the day after taking psoralens.
Antimalarial Drugs.
Antimalarial drugs may be effective and should be considered for patients who are not protected by sunscreens and do not respond to UVB or PUVA phototherapy. Antimalarials need to be used only during the summer months; therefore the total necessary dose is small. A 3-month trial (hydroxychloroquine 400 mg/day for the first month and 200 mg/day thereafter) has been effective in reducing rash and irritation. Although the risk of eye damage is slight, ophthalmologic examinations should be obtained periodically to monitor for antimalarial toxicity.
Other Treatments.
Beta-carotene is somewhat effective for prophylactic treatment of PMLE, but the skin turns yellow-orange. Only 30% of patients responded satisfactorily to a dosage of 3 mg/kg body weight continued throughout the summer. Cyclosporine or azathioprine may be used for rare severe disabling cases.
Hydroa Aestivale and Hydroa Vacciniforme
Hydroa aestivale (summer prurigo of Hutchinson) and hydroa vacciniforme (HV) are rare but very distinctive light-induced eruptions. They may represent a type of PMLE that is peculiar to children. The onset is before puberty (average age at onset is about 6 years), and males are affected more frequently than females. It begins with moderate erythema and itching within 1 to 2 hours of sun exposure. The lesions of hydroa aestivale consist of papules with weeping and crusting. The symmetric photodistributed eruption is most prominent on the face, ears, and backs of the hands ( Fig. 19.21 ). Involvement of non–sun exposed areas, especially the buttocks, is not uncommon. The rash fades but may persist through the winter months. There is evidence of genetic transmission. In many cases, UVB light reproduces the lesions.

Hydroa vacciniforme (HV) ( Figs. 19.22 and 19.23 ) is similar to hydroa aestivale, except that tense, umbilicated vesicles resembling smallpox appear on the face, ears, chest, and backs of the hands; after they break and form a crust, they may heal with varioliform scarring. UVA light may reproduce the eruption. Both diseases usually clear after puberty. Avoidance of the sun and use of sunscreens, group V topical steroids, and wet compresses and antimalarials can control these diseases.


Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


