| Marcus Gunn syndrome with functional or cosmetically displeasing jaw wink |
| Unilateral ptosis with poor levator function requiring frontalis suspension |
| Ptosis evaluation (MRD1, levator excursion, frontalis function, eyelid malpositions, lagophthalmos) |
| Photographic and/or video documentation of eyelid position with opening, closing and side-to-side movements of the jaw (synkinetic movement) |
| Rule out amblyopia |
| Presence of Bell’s phenomenon |
| Evaluation for associated strabismus (including monocular elevation deficiency) |
| Slit lamp examination/ocular surface evaluation |
Introduction
Eyelid ptosis repair with levator extirpation and concomitant frontalis suspension may be performed for a symptomatic jaw wink associated with Marcus Gunn syndrome as well as severe unilateral, poor levator ptosis.
Marcus Gunn syndrome is characterized by aberrant innervation between cranial nerve III and V resulting in synkinetic movements of the levator palpebrae superioris and the ipsilateral pterygoid muscles. The synkinetic movement can be seen during infancy as variable upper eyelid retraction with opening of the mouth, chewing, and sucking. Lateral, side-to-side jaw movements may also bring about the jaw wink associated with this syndrome. Marcus Gunn is typically unilateral, but bilateral cases have been described.
The clinical presentation of Marcus Gunn is variable, depending on the degree of aberrant miswiring. Ipsilateral ptosis from levator dysgenesis may be the prominent presentation necessitating levator resection ( Chapter 14 ) or frontalis suspension ( Chapter 15 ). Alternatively, the levator function may be preserved and the most symptomatic finding is the displeasing wink seen with jaw movements.
The evaluation of Marcus Gunn should include documentation of eyelid position and levator excursion with full jaw movements. Photographic and video documentation are useful to educate patient and parents about the condition and surgical outcomes. An evaluation for associated strabismus, in particular co-existent superior rectus dysfunction, should be performed. Any amblyopia from strabismus or anisometropia must be addressed with spectacle correction and patching before considering eyelid surgery.
If the jaw winking phenomenon does not objectively improve with age or if the patient is unable to mask the synkinesis, levator extirpation with frontalis suspension may be considered for treatment of this displeasing jaw wink. The decision of unilateral versus bilateral surgery is a controversial topic. Parents typically opt for unilateral surgery of the aberrantly innervated side to spare the normal side from surgical intervention. The primary benefit of surgery on both sides is to drive bilateral frontalis function when eyelid elevation is desired.
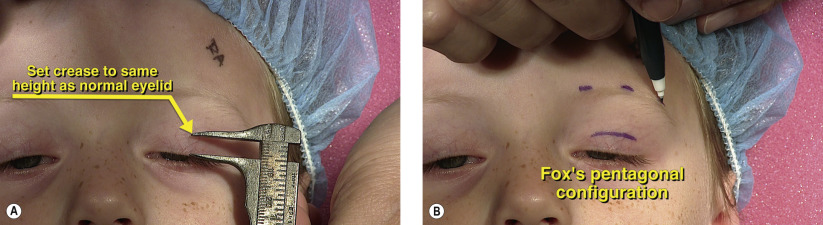
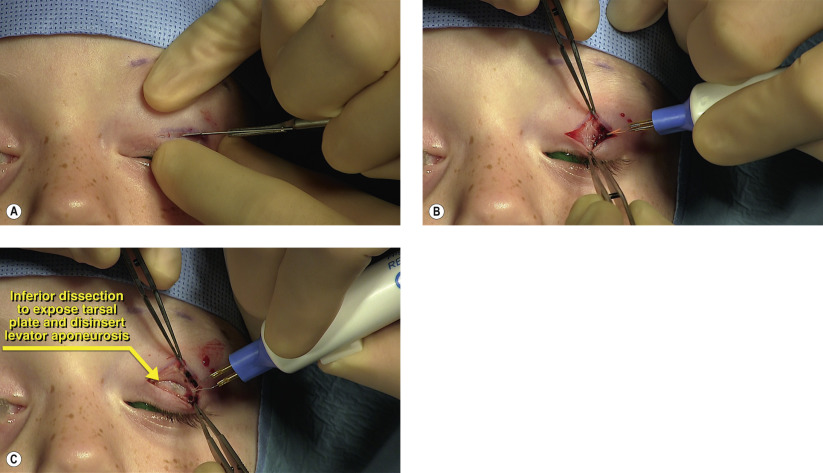
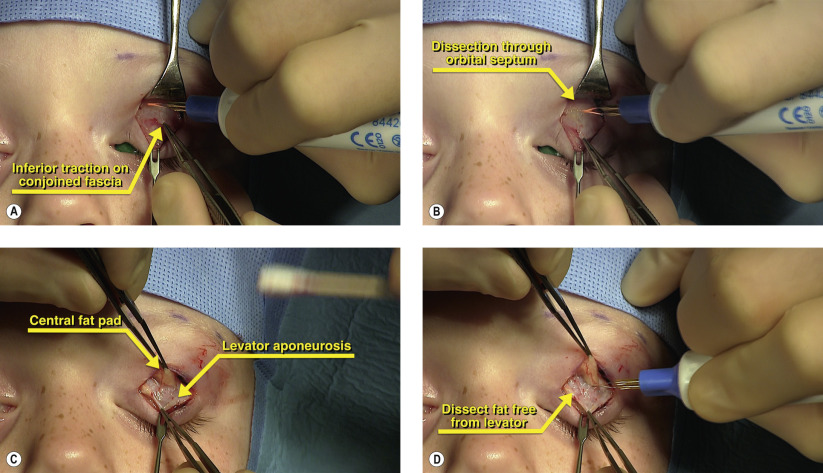
The surgical approach involves disinsertion of the levator aponeurosis from the tarsal plate and then extirpation of the levator. Multiple approaches have been described including anterior and posterior approaches as well as extirpation of the muscle at the level of Whitnall’s ligament and even to the orbital apex. The risks of recurrence of the jaw wink with suboptimal levator extirpation versus damage to the superior rectus with more aggressive muscle removal must be weighed carefully. Our preferred technique for mild-to-moderate jaw wink is a unilateral, anterior approach levator extirpation to the level of Whitnall’s ligament with disinsertion of the medial and lateral horns of the levator. Frontalis suspension is then performed with fascia lata or silicone rod. Silicone rod affords the advantage of easy reversibility, and this is important especially in patients with reduced corneal protection (poor Bell’s phenomenon). Furthermore, in patients under 2 years of age, harvesting of autologous fascia lata is not recommended.
Surgical Technique