Latissimus Dorsi Flap for Chest Wall Defects
Essie Kueberuwa Yates
David H. Song
DEFINITION
Composite defects of the chest wall can arise secondary to oncological extirpation, ablation due to infection, congenital defects, trauma, radiation, or iatrogenic causes such as surgical access and hardware extrusion.
Methylmethacrylate (in a nonradiated wound bed), bioprosthetic mesh, vascularized bone, local myocutaneous flaps, and free tissue transfer are all routinely used in the reconstruction of chest wall defects.
The choice of technique is related to size, extent, and location of the defect and the availability of donor site.
The latissimus dorsi flap (LDF) is a reliable flap with a robust and predictable vascularity. The proximity of the flap to the chest wall makes it an ideal choice for providing muscle, fat, and skin for use in reconstructing large chest wall defects.
The thoracodorsal artery system nourishes the LDF and offers the possibility for incorporating multiple tissue types of its single vascular pedicle (chimeric flap).
ANATOMY
The LD muscle has multiple origins (FIG 1):
Spinous processes of T7-T12
Thoracolumbar fascia
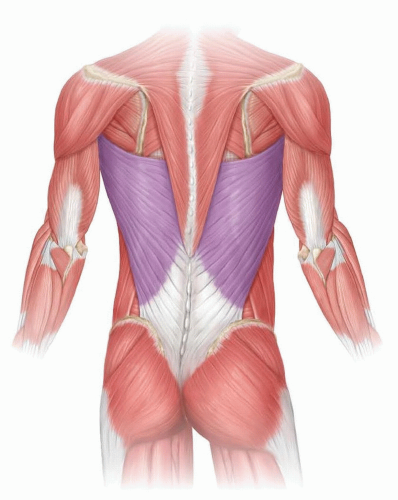
FIG 1 • Latissimus dorsi muscle.
Posterior third of the iliac crest
Lowest six ribs
The LD muscle inserts into the intertubercular groove of the humerus.
It is a broad flat muscle, which is the most superficial back muscle overlying the paraspinous muscles medially and serratus anterior laterally. It lies deep to the trapezius superomedially.
The LD is a type V muscle, with the dominant vascular pedicle being the thoracodorsal artery, a terminal branch of the subscapular artery, which arises from the third portion of the axillary artery.
The thoracodorsal artery runs on the underside of the muscle, and the main pedicle divides into two main branches: an upper horizontal branch that travels medially along the superior border of the muscle and a descending oblique branch that runs inferiorly, parallel to the anterior border of the muscle about 2.5 cm from the edge.
The bifurcation is predictably found 4 cm distal to the inferior scapular border and 2.5 cm medial to the anterior border of the muscle.
Thoracodorsal artery perforators exit the muscle and perfuse the subcutaneous tissue, one of these perforators is typically located 8 cm below the posterior axillary fold and 2 cm behind the anterior border of the LD muscle.1
Secondary pedicles arise dorsally and mostly perfuse the distal part of the muscle. They are typically found about 5 to 10 cm lateral to the spinous processes and are arranged in a medial row (branches of the lumbar arteries) and a lateral row (branches of the intercostal arteries).
The largest and most constant of these secondary blood supplies are the branches of the 8th to 11th intercostal arteries. They are typically not useful for large anterior chest wall reconstructions due to their location and short pedicle length.
These branches can be used, however, when the LD has been previously transected in a standard non-muscle-sparing thoracotomy incision, as the distal portion of the muscle can still be mobilized to provide coverage of limited posterior defects.
PATIENT HISTORY AND PHYSICAL FINDINGS
When evaluating a chest wall defect, important considerations include the following:
Viability and quality of the wound bed (radiated, inadequately debrided; presence of contaminated hardware and large dead spaces result in poor wound healing)
Effect of the wound on respiratory mechanics
Exposure of vital structures
Aesthetics and contour of the chest
Typically, defects larger than 5 cm or involving more than three ribs require chest wall stabilization in addition to soft tissue coverage.
In the postirradiated chest wall, larger defects can be tolerated without fixation due to the rigid scarring and fibrosis of tissue.
SURGICAL MANAGEMENT
The LDF is ideal for chest wall reconstruction because the axis and length of the thoracodorsal pedicle afford this flap an excellent arc of rotation and virtually any part of the ipsilateral chest wall can be reached.
The most common uses of the LD in chest reconstruction are as a muscle-only flap for intrathoracic obliteration of dead space or as a musculocutaneous flap for coverage of large chest wall defects.2
Preoperative Planning
When planning chest wall reconstruction with an LD flap, the main considerations are as follows:
Ensuring vascularity and availability of donor site. (On occasions, the muscle is transected during thoracotomy.) Some syndromes (eg, Poland) are associated with congenital absence of the pectoralis and LD muscle.
Assessing defect size: The thoracodorsal artery provides branches to the serratus muscle, which can be taken in conjunction with the LDF if a larger flap is necessary.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








