Introduction
•
The problem being treated
Prominent leg veins affect as many as 41% of women and 15% of men in the United States. Vascular pathology can be divided into superficial spider veins or telangiectasias, deeper reticular veins, and protuberant varicosities ( Fig. 7.1 ). Causes include heredity, hormones, prolonged standing, obesity, pregnancy and aging. Although leg veins may cause symptoms such as fatigue, aching, swelling, throbbing and pain, treatment is sought mainly because of their unsightly appearance.
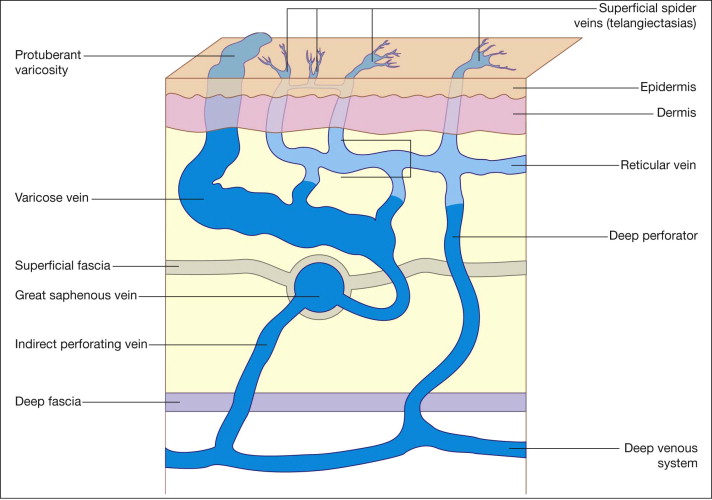
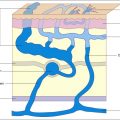
The venous system of the lower extremity is composed of a complex, interconnected superficial and deep plexus. The superficial veins lie just beneath the skin, and the deep veins travel within the muscles of the leg. Because of flow patterns between the two networks, superficial spider veins may be the result of increased pressure in deeper reticular or varicose veins.
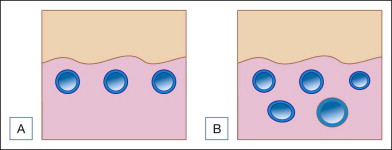
The variety of sizes, depths, flow patterns, and vessel thickness make the treatment of leg veins much more difficult than treatment of facial veins. One important consideration is that even the fine, relatively superficial telangiectatic vessels of the legs are not very close to the surface of the skin, like facial veins, but rather can lie at a depth of up to several millimeters. Most smaller telangiectasias (0.2–1.0 mm) lie at a depth of about 300 µm below the surface of the skin and represent the most common complaint among patients presenting with leg veins. Adverse events and incomplete response may result as laser energy is dissipated in the overlying skin with only partial effect permeating to the targeted vessels ( Fig. 7.2 ). There is no single treatment for all leg veins and lasers may be used as adjunctive therapy in patients receiving sclerotherapy, ambulatory phlebectomy or endovenous ablation.
Laser therapy is particularly useful for the treatment of small spider veins or telangiectasias (<0.5 mm) and in the treatment of telangiectatic matting resulting from other modes of treatment. It can also be used in the treatment of large spider and small reticular veins. Sclerotherapy is generally still considered the gold standard for treatment of larger leg veins, however several studies suggest that results between laser therapy and sclerotherapy are equivalent in spider and small reticular veins. Varicose veins are best treated with phlebectomy, ligation or endovenous ablation ( Box 7.1 ). This chapter will deal only with laser surgery; sclerotherapy and surgical procedures are discussed elsewhere in this book.
- •
Small telangiectasias: laser or sclerotherapy
- •
Telangiectatic matting: laser or sclerotherapy
- •
Large spider veins, reticular veins: sclerotherapy
- •
Varicose veins: endovenous ablation, ambulatory phlebectomy or ligation
Patient Selection
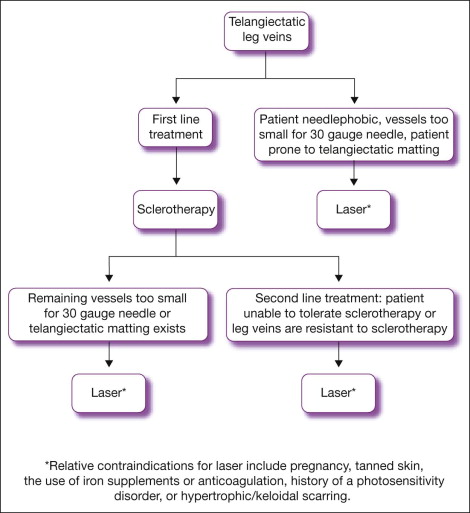
Laser treatment is most effective for small, superficial red or blue veins. It is an ideal therapy for patients who are prone to telangiectatic matting, do not respond to sclerotherapy, or are fearful of needles. Relative contraindications to laser surgery include pregnancy, tanned skin, the use of iron supplements or anticoagulation, history of a photosensitivity disorder, or hypertrophic/keloidal scarring ( Fig. 7.3 ).
Expected Benefits
Laser therapy is an effective modality for the treatment of leg veins. Small telangiectatic vessels often disappear at the time of treatment, providing the patient and physician with a visual record of success. Larger telangiectasias and reticular veins typically do not disappear at the time of treatment, but will gradually improve over the course of several months. Selected vessels may clinically darken after treatment as the blood in the vessels coagulates. have compared laser therapy with a long pulsed Nd:YAG laser to foam sclerotherapy with 0.6% sodium tetradecyl sulfate in 20 patients with vessels ranging from 0.25–3.0 mm. The group found that mean clearance scores were a slightly better 2.5 out of 4.0 for laser treated veins compared to 2.3 out of 4.0 for sclerotherapy, however only 35% of the patient group said they preferred laser treatment to sclerotherapy. conducted another study comparing liquid sclerotherapy with 0.5% polidocanol to the long pulsed Nd:YAG laser for vessels ranging from 0.5–2.0 mm, and also found the two treatment methods to be equivalent with no statistical difference in outcome.
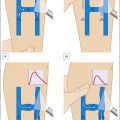
In a study by treating reticular and spider telangiectasias on the lower legs using the monomodal approach with the 1064 nm Nd:Yag laser and variable spot sizes and pulse width parameters, approximately 20% of treated vessels had a 50–75% improvement after three treatments spaced 1 month apart ( Fig. 7.4 ). Improvements continued over time, with 80% of vessels having greater than 75% clearing at 6 months follow up. Of the patients treated, 90% were highly satisfied with the treatment.






In a comparative study by Eremia and Umar of the 1064 nm Nd:Yag, 810 nm diode, and 755 nm Alexandrite lasers for the treatment of leg veins measuring 0.3–3 mm in diameter, the Nd:Yag laser was associated with the greatest percent improvement at 3 months’ follow up ( Table 7.1 ). Purpura and matting were problematic with the Alexandrite laser, and results with the long-pulsed diode were unpredictable among the 22 women in the study. No long-term controlled studies have been carried out regarding the persistence of vessel clearing after laser treatment of the legs.
| Laser | Patients achieving 75% clearance at 3 months |
|---|---|
| 1064 nm Nd:Yag | 88% |
| 810 nm diode | 29% |
| 755 nm Alexandrite | 33% |
Problems intrinsic to the use of lasers for the treatment of leg veins include the need for multiple treatments, patient discomfort, inconsistent results, and high equipment cost. Reported complications include transient hyperpigmentation, purpura, epidermal surface change, telangiectatic matting and thrombus formation. When a systematic approach is used, sclerotherapy can treat 80–90% of vessels in a single treatment. Because of the relatively low cost of venous surgery and sclerotherapy, lasers are generally not recommended as first-line treatment.
Overview of Treatment Strategy
•
Treatment approach
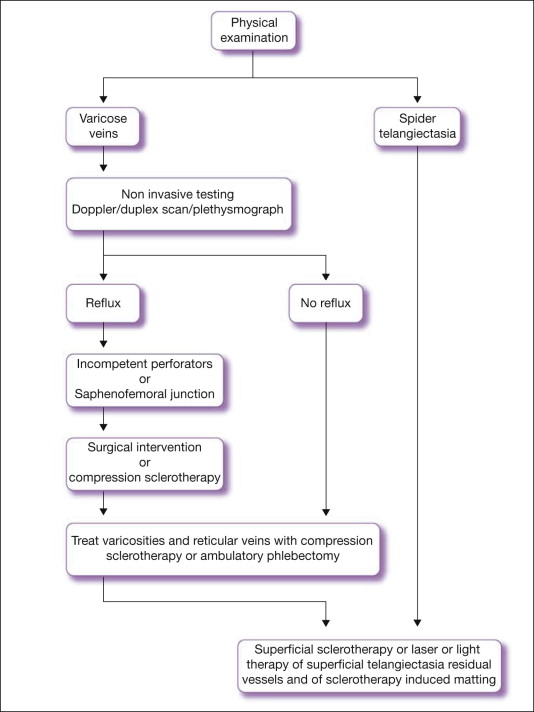
A detailed physical examination should be performed on all patients presenting for the treatment of leg veins to evaluate the type and size of venous pathology and the presence of reflux or incompetent valves. Large varicose veins showing reflux must be addressed first to avoid unsuccessful treatment of smaller telangiectasias and potential complications such as dyspigmentation and telangiectatic matting.
The treatment of leg veins should follow a systematic approach ( Fig. 7.5 ). First, varicosities and large feeder vessels should be surgically removed (by ligation, stripping, or ambulatory phlebectomy) or treated with endovenous ablation. Sclerotherapy should then be performed proceeding from large to small vessels. This will clear approximately 80–90% of vessels in a single treatment. Laser and light therapy should be used to treat any remaining vessels and those that are too small to reasonably undergo sclerotherapy with a 30–32 gauge needle.
•
Major determinants
Lasers in the treatment of leg veins follow the principles of selective photothermolysis ( Box 7.2 ). The major parameters that must be chosen to treat an individual vessel include wavelength, pulse duration, and spot size ( Table 7.2 ).
- •
The ideal laser must have a wavelength proportionately better absorbed by hemoglobin than the surrounding tissue
- •
Penetration should reach the full depth of the target vessel
- •
Sufficient energy must be delivered to damage the vessel without damaging the overlying skin
- •
Energy must be delivered over an exposure time long enough to slowly coagulate the vessel without damaging surrounding tissue
| Wavelength | 530–1064 nm |
| Pulse duration | 2–100 ms |
| Fluence | 30–150 J/cm 2 |
| Spot size | 1.5–10 mm |
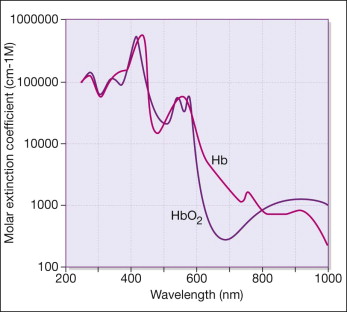
The absorption spectrum of hemoglobin has major peaks at 410, 540, and 577 nm, with smaller peaks at 920–940 nm. Blue veins respond better to wavelengths targeting the deoxyhemoglobin spectrum and red veins respond better to wavelengths targeting the oxyhemoglobin spectrum ( Fig. 7.6 ). Absorption by hemoglobin in the long visible to near infrared range is important for vessels >0.5 mm in diameter and at least 0.5 mm below the skin surface.