Key points
- •
Recently, lasers have been adapted for the removal of localized adipose tissue.
- •
Careful patient selection, technical knowledge and skill as well as proper subject orientation are essential for the success and safety of the laser-assisted lipolysis.
- •
Laser-assisted lipolysis with a 1064 nm pulsed Nd:YAG laser can be used in the treatment of localized adipose tissue and flaccidity in the face and body in patients with normal body weight. It is not indicated for the treatment of obesity.
- •
The activity of the laser throughout the photomechanical and thermal effects leads to cell disruption (laser lipolysis) and the stimulation of new collagen formation with a consequent tightening effect.
- •
Histological studies have shown positive effects as in the coagulation of small blood vessels, rupture of adipocytes, reorganization of reticular dermis and new collagen production.
- •
Very recent indications of Nd:YAG laser lipolysis include cellulite, axillary hyperhidrosis, bromidrosis, osmidrosis, and lipoma.
Background
Liposuction has become increasingly popular. Currently, it is the most common cosmetic surgical procedure. Laser technique can be used to disrupt the fat. Indeed, laser–fat interaction was initially published in 1992 using a 40 W Nd:YAG laser ( ). Carbon dioxide laser and diode laser were also reported for neck rejuvenation and fat disruption. Recently, several studies demonstrated the beneficial use of the internal 1064 nm Nd:YAG laser acting directly not only on adipose tissue, but also on vessels and dermis. The main effects are adipocyte cell disruption, coagulation of small blood vessels, collagen stimulation, and thereby skin retraction.
Patient selection
The careful and judicious selection and preparation of patients, technical knowledge and skill as well as proper subject orientation are essential for the success and safety of the procedure. Adequate patient selection and managing patient expectations are most important in order to achieve an effective result and patient satisfaction. A complete history and physical and psychosocial evaluation play a fundamental role in the success and safety of each laser-assisted liposuction (LAL) treatment. Physical evaluation includes assessment of the general physical health and body mass index (BMI). Appropriate laboratory studies must be performed on all candidates. Appropriate patients include subjects with localized subcutaneous adipose tissue deposits. Pre-existing medical conditions need to be under control.
Laser lipolysis is not an adequate treatment for obesity. Laser-assisted liposuction is contraindicated in pregnancy, in patients suffering from either severe cardiovascular disease or coagulation disorders, recent abdominal surgery, acute infections, and thrombophilia. Special attention must be paid to drug history because of bleeding risks (e.g., aspirin, non-steroidal anti-inflammatory agents, vitamin E, high-dose vitamin C, anticoagulants, and Ginkgo biloba ). In summary, the ideal candidate for the procedure is a healthy, non-obese, non-smoking patient without significant skin flaccidity such as cutis laxa.
Indications
The indication for laser-assisted liposuction is similar to that of traditional liposuction. The primary aim is body contouring by removal of localized lipodystrophy of subcutaneous adipose tissue of face and body in patients with realistic expectations for treatment outcomes. The method should not be considered for body weight reduction or in the treatment of obesity. Even patients presenting a certain degree of skin laxity are candidates for the treatment.
Irregularities of the adipose tissue in previously treated areas, gynecomastia, cellulite and skin flaccidity represent useful indications for the Nd:YAG laser-assisted liposuction as well. The laser can be used in combination with traditional surgical techniques such abdominoplasty, lipoabdominoplasty, cruroplasty, rhytidectomy or brachioplasty. In selected cases, the procedure can be use in patients without lipodystrophy for the purpose of skin tightening.
Operative technique
Pre-operative preparation
Similar to traditional (suction-assisted), power-assisted or ultrasound-assisted liposuction, the first step is the demarcation of the areas to be treated with the patient in the standing position. Informed consent and standardized high-quality photographic documentation is required for all patients. Relevant aspects such as previous treatments, presence of scars, skin texture and elasticity, as well as the amount, consistency and distribution of localized adipose tissue must be evaluated before the treatment and discussed with the patient. The placement and number of incisions has to be determined with the patient prior to surgery, avoiding symmetric scars. If using local anesthesia only, these incisions are reinfiltrated with lidocaine prior to making the incision. The position of the patients during the procedure depends on the areas to be treated. Special attention should be paid to the potential hemodynamic reperfusion when changing the patient’s position during the procedure.
In order to perform and communicate consistency of treatments and energy application, the liposuction area is also marked with 5 cm × 5 cm square sectors. Further recommendations are based upon these known areas and subsequent cubic volume. Laser-assisted liposuction procedures are usually performed using tumescent anesthesia. Usually, subcutaneous infiltration of Klein’s solution, Hunstad formula, or a similar solution containing normal saline, epinephrine and sodium bicarbonate (lidocaine, 500 mg; epinephrine, 1 mg (1 mL of 1 : 1000 dilution); and 12.5 mL of 8.4% sodium bicarbonate, 10 milliequivalents are added to each liter of normal saline) is performed. The total volume of the infiltration will vary according to the treated area and is affected also by the surgeon’s preference. Often, 75–100 mL of tumescent fluid is administered per sector. This amount provides enough anesthesia as well as a good fluid environment for the laser light to function optimally.
The procedure can be performed under local anesthesia with or without oral or IV sedation, general anesthesia or even epidural block. In order to decrease the pain or discomfort during the infiltration, we suggest the use of sodium bicarbonate in the solution which optimizes the pH of the solution and to inject slowly using a small needle or cannula with pumps or syringes. It is advisable to warm the tumescent solution in order to reduce perioperative hypothermia and to avoid thermal shock.
Technique
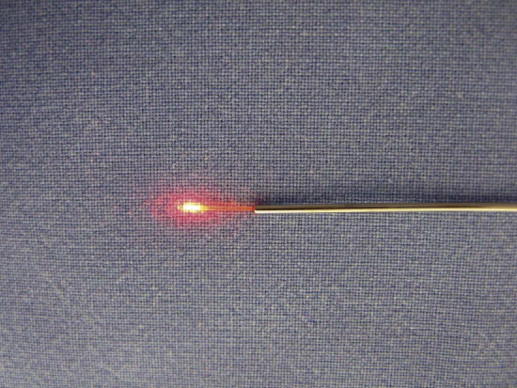
After adequate marking, the surgical regions are disinfected with antibacterial solution. The procedure is initiated following a 15–20 min delay, allowing diffusion of the infiltrate and appropriate vasoconstriction. The pulsed 1064 nm Nd:YAG laser system provides ultra short pulses and has extremely high peak powers (Smartlipo™, Deka, Italy, and Cynosure, USA). In this procedure, the laser energy is delivered to the subcutaneous tissue through a 300 µm or 600 µm fiber optic with a 1 µm or 1.2 µm diameter stainless steel micro-cannula of variable length connected to the tip of the fiber ( Figure 11.1 ). The total energy varies according to the area to be treated, the amount of fat, necessity for dermal stimulation and tightening effect as well as previous treatments. Rigid parameters must be avoided. Every patient and each area have to be carefully evaluated in order to select adequate energy and mainly the endpoint of the laser activity.
The following guidelines have been established based upon initial studies pending publication in the United States. After tumescent anesthesia is given, a three step treatment sequence follows: (1) laser treatment of deep fat (2) laser skin stimulation (temperature based), and (3) final aspiration. As work progesses in this area, other sequences or combinations may be preferable. When treating small or very superficial areas such as in the face, power and/or laser action time can be lowered. Learning curve and the accumulated experience of the surgeon will determine the optimum parameters in every situation. It is most important to be conservative in initial or reoperative cases and in the treatment of superficial areas, avoiding overcorrection, irregularities or skin lesions.
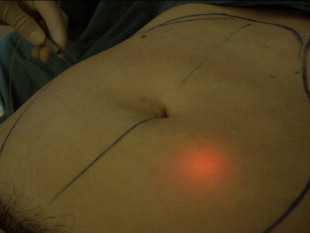
The distal portion of the fiber optic is extended 2 mm beyond the distal end of the cannula. A helium neon laser source is positioned within the beam path providing a precise localization of the laser tip using trans-illumination. The more intense the red light, the more superficially (subdermal) the laser is working ( Figures 11.1, 11.2 ). The 600 micron laser fiber is trimmed approximately every 25 000 joules to insure an even beam of light and fiber the integrity. This process includes stripping away the plastic collar followed by light pressure on the fiber itself with a cutter. The tip is gently moved to break it off resulting in a clean cut fiber tip. If the aiming beam is held up to to one’s glove, an even red circle of light should be seen.
A 1 mm incision is sufficient to introduce the cannula. This small incision can be made using a 40 G needle or even an 11 blade. The laser must be off while introducing it into the incision to avoid skin burning. The same care must be taken while the laser cannula is removed from the subcutaneous adipose tissue. Once inserted, the laser can be activated and then moved slowly forward into the fat tissue at various depths, including the sub-dermal layer. It is in the subdermal plane that skin irregularities such as dimpling, acne scarring, or scarring from previous liposuction may be treated and possibly improved. The 1 mm cannula and fiber size allows for work in this plane with less chance of grooving or furrows.
In our practice, associated procedures are often avoided. In isolated and selected cases, some minor associated procedures can be performed. The total accumulated energy used in specific regions varies. The energy should be sufficient to overcome resistance of the cannula in its movement against the tissue. If the 5 cm × 5 cm sector is measured by caliper, the thickness of the deep fat should be estimated. This thickness represents the cubic volume requiring laser energy. Guidelines of 1000–2000 J of energy per 1 cm of thickness of adipose tissue is usually sufficient: less in softer areas, more in fibrous tissue or scars. With increasing experience of the operator, more of this layer can be done by feel or forward pressure sensation. The tissue consistency should be evaluated by the pinch test. Usually the tissue will feel less dense than before. Skin calipers can be used to get a more exact measure of the skin and fat thickness both before and after treatment. Significant histological findings following laser lipolysis include adipose tissue lysis with the formation of small channels, coagulation of small blood vessels in the fatty tissue, coagulation of collagen and reorganization of reticular dermis.
Tissue tightening
With increasing clinical experience of the subdermal application of laser energy, there has been an obvious effect on the skin laxity evident clinically and in photographs. Previous in vitro and in vivo studies have indicated a relationship of increasing dermal temperature and stimulation of fibroblasts resulting in increased production of collagen and elastin. The goal temperature is 42°C as measured on the skin surface. Correlation of skin surface temperature, deep temperature 5 mm below the skin and corresponding histology have shown 42°C to be a safe upper limit for dermal stimulation (DiBernardo, unpublished).
This represents the second step of the procedure. After deep laser energy application, the laser fiber is introduced under the dermis with a steady movement of the aiming beam within the 5 cm × 5 cm square. An assistant frequently measures skin surface temperature using a handheld laser guided thermometer to insure evenness of the heat application as well as the upper limit surface heat (42°C). Caution should be used in thinner skin since it can heat up more quickly. Insufficient energy or advanced age can result in inadequate skin tightening. It typically requires 100–150 J of energy to raise the skin temperature by 1°C. Excessive tumescent fluid can also make it difficult to achieve these goals. More recent methods of temperature measurement are thermal cameras and thermistors incorporated into the laser canula.
Aspiration
In small areas, with an estimated amount of fat of up to approximately 50 g, it is not necessary to remove the oily solution, which is a product of the adipocyte disruption. In cases where the main indication is skin tightening, it is not necessary to aspirate tissue where the intention is only dermal stimulation and coagulation. The product of the cellular lysis is usually removed from the treated region by aspiration using negative pressure of around 0.5 atm in conjunction with a 2.5 mm or 3 mm suction cannula. The authors recommend syringes, pumps or aspirators.
Closure
No drains are used in this procedure. It is not necessary to use sutures for the small incisions, thereby allowing for a natural drainage of the infiltrated solution, blood and the oily debris produced by the laser action. A smooth compression garment is used for 7–10 days after the procedure. This garment should not be very compressive to allow adequate lymphatic drainage. Smooth compression garments are usually comfortable for patients and are effective in helping to reduce bruising, hematomas, seromas, and pain. Early progressive return to exercise is recommended at 7 days post-operatively.
Operative steps
- •
The procedure is initiated following a 15–20 min delay after subcutaneous infiltration, allowing for diffusion of the anesthesia and appropriate vasoconstriction.
- •
All medical staff and patients must wear protective glasses.
- •
Once inserted through the 1 mm incision, the laser cannula is moved slowly in the fat tissue at various depths, including the sub-dermal layer. The more superficial the laser action (subdermal), the more intense the tightening effect.
- •
Observe the endpoint to the laser action represented mainly by the overcoming of resistance of the cannula in its movement against the tissue or estimated Joules. A reddish trans-illumination from the aiming beam will assist in locating and directing the laser tip.
- •
The product of the cellular lysis is removed under negative pressure of around 350–450 mmHg in conjunction with a 2.5 mm or 3 mm suction cannula using syringes, pumps or aspirators. It is not necessary to suture the small incisions.
- •
Smooth compression garments (not very elasticized or compressive) allow a normal lymphatic drainage and can help in reduction of bruising, hematomas, seromas, and pain.
- •
Early ambulation of patients is advisable to avoid venous stasis.
Related posts:
 CO 2laser applications: new fractional and traditional CO 2laser resurfacing and CO 2laser blepharoplasty
CO 2laser applications: new fractional and traditional CO 2laser resurfacing and CO 2laser blepharoplasty
 Aging skin: intrinsic aging and chronic photoaging
Aging skin: intrinsic aging and chronic photoaging
 Laser hair removal
Laser hair removal
 Advances in light-emitting diodes (LED) technology and therapy
Advances in light-emitting diodes (LED) technology and therapy
 Low level laser therapy in hair loss
Low level laser therapy in hair loss
 Clinical photography for laser and light-based therapies
Clinical photography for laser and light-based therapies
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


