Laser Hair Removal in Darker Racial Ethnic Groups
Teresa Soriano
David Beynet
Dafnis C. Carranza
Laser-assisted hair removal (LHR) is a commonly performed cosmetic procedure today. Initially, LHR was reserved for patients with lighter skin types (Fitzpatrick I–III) because of the increased incidence of adverse effects in patients with darker skin. Over the last decade, with the advent of lasers with longer wavelengths, longer pulse durations, and improved cooling mechanisms, LHR can be safely performed in all skin types, including Fitzpatrick types IV to VI. It has the ability to significantly reduce the number of hairs and their rate of growth while maintaining a low incidence of side effects.1,2,3
LHR is of special importance in ethnic skin types for several reasons. Darker-skinned patients often have darker, coarser, and thus more noticeable hair than lighter-skinned patients. This may lead to increased cosmetic concern of unwanted hair in darker-skinned patients. In addition, certain diseases that are more prevalent in patients of color—such as hirsutism, pseudofolliculitis barbae, and acne keloidalis—can be improved with laser therapy.4
Laser Choices
The mechanism of LHR is based on the theory of selective photothermolysis. In selective photothermolysis, heat is released by a target chromophore, which has absorbed photons from the laser. This heat destroys neighboring structures, causing permanent damage.5 In LHR, the target chromophore is melanin, which is primarily found in the hair bulb and hair shaft. After photon absorption, heat is released by the hair shaft and hair bulb, causing permanent thermal destruction of the surrounding follicular structures.
The higher concentration of melanin in the epidermis of darker skin types presents a challenge in LHR treatment of this population compared with lighter skin types. There are two unwanted outcomes. The first is that less photons ultimately reach their intended site, the follicular structures, which results in decreased efficacy. The second is that there is increased heating of the epidermis.6 This can lead to side effects, such as hyperpigmentation, hypopigmentation, blistering, and scarring.
The melanin absorption spectrum ranges from approximately 300 to 1,200 nm, with absorption decreasing as wavelength increases. Follicular structures are located to a depth of 2 to 4 mm within the dermis. The ideal laser thus should have a wavelength that can provide adequate photon absorption by melanin, as well as penetration into the dermis. Wavelengths between 600 and 1100 nm are capable of this.7
In addition to wavelength, pulse duration is an important consideration in LHR. Relatively long pulse durations are necessary. Long pulse duration results in slow heating of the follicular unit and greater diffusion of heat from the hair shaft and bulb during the pulse. This allows for destruction of the entire follicular unit, not only the pigmented components.8
There has been a marked increase in the number of lasers for LHR since the first lasers were approved in 1996.9 LHR has primarily been done with the following light sources: the ruby laser (694 nm), the alexandrite laser (755 nm), the diode laser (810 nm), the neodymium:yttruium-aluminum-garnet laser (Nd:YAG) (1,064 nm), intense pulsed light (IPL), and IPL with radiofrequency (IPL/RF) (Table 32-1). The ruby laser is the most selective for melanin absorption but has short penetration depth and a higher incidence of side effects. The Nd:YAG laser has the deepest penetration but the least specificity for absorption by melanin.8 This may result in decreased efficacy; however, it lends itself to fewer adverse effects. The alexandrite and the diode lasers have benefits of both of these extremes. IPL works by using noncoherent light with wavelengths ranging from 515 to 1,200 nm. By using different cutoff filters, treatment parameters can be adjusted to allow safer treatment for patients with different skin types. In addition, devices combining radiofrequency with an intense pulsed light have been used for LHR. It has been proposed that lower fluences can achieve hair reduction in these devices, thus making IPL/RF a safe alternative of LHR for darker-skinned patients.10
Table 32-1 Lasers and light sources for hair removal | |||||||
|---|---|---|---|---|---|---|---|
|
In ethnic skin, the safest lasers are those with longer wavelengths, longer pulse durations, and optimal cooling devices. The longer wavelength diode and Nd:YAG are the preferred devices to safely perform LHR in ethnic skin. (Table 32-2) (Figs. 32-1 and 32-2).3,11 The increased wavelength allows for decreased epidermal melanin absorption and increased penetration depth. The long pulse duration causes slower heating and results in a lower incidence of dyspigmentation. Between the two laser systems, the longer-wavelength 1,064-nm Nd:YAG laser is generally safer, particularly for very dark skin types, however, the diode laser may be more effective because of greater melanin absorption.9 A mean hair reduction ranging from 58% to 62% on facial sites and 66% to 69% on nonfacial sites has been reported after three treatments with the long-pulsed Nd:YAG compared with 74% to 84% hair reduction with the diode laser 6 months after the final laser treatment.8 Both long-pulsed Nd:YAG and diode devices are FDA approved for LHR in darker skin types.
Table 32-2 Optimal lasers for darker racial ethnic groups | ||||||
|---|---|---|---|---|---|---|
|
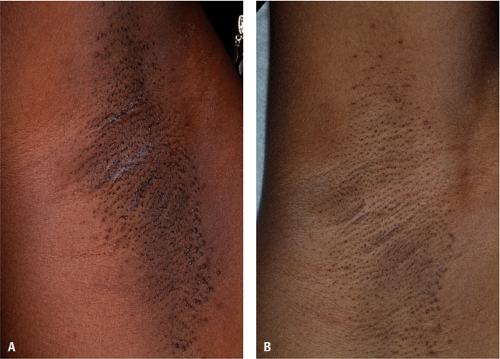 Figure 32-1 Axillary hair, skin type V: baseline (A), after five long-pulsed 1064 nm Nd:YAG treatments (B). (Courtesy of Pearl E. Grimes, MD.) |
Efficient cooling devices provide added benefit for LHR, especially in ethnic skin. Cooling devices function to cool the epidermis and prevent laser-induced thermal damage. Epidermal thermal damage can result in dyspigmentation, scarring, and blistering, especially in darker skin types. Cooling devices also have the added benefit of
decreasing pain associated with the procedure. Current cooling devices use both evaporative and conductive mechanisms. These tend to provide more efficient epidermal cooling than older techniques of using ice or water-based gel. Dynamic cooling devices function by using a cryogen spray immediately before the laser pulse, which evaporates and instantaneously cools the epidermis.12 Conductive cooling devices include cooled sapphire laser windows, which cool the epidermis by conductive heat transfer. Conductive devices also lead to dermal compression, which has two benefits: It brings follicular structures closer to the area of maximal dermal laser penetration, and it compresses blood vessels, thereby decreasing the concentration of the hemoglobin.6
decreasing pain associated with the procedure. Current cooling devices use both evaporative and conductive mechanisms. These tend to provide more efficient epidermal cooling than older techniques of using ice or water-based gel. Dynamic cooling devices function by using a cryogen spray immediately before the laser pulse, which evaporates and instantaneously cools the epidermis.12 Conductive cooling devices include cooled sapphire laser windows, which cool the epidermis by conductive heat transfer. Conductive devices also lead to dermal compression, which has two benefits: It brings follicular structures closer to the area of maximal dermal laser penetration, and it compresses blood vessels, thereby decreasing the concentration of the hemoglobin.6
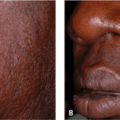
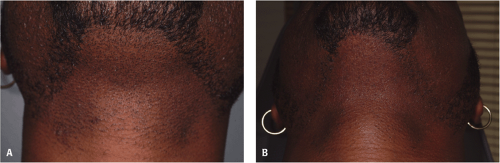 Figure 32-2 Unwanted facial hair, skin type V: baseline (A), after four long-pulsed 1064 nm Nd:YAG treatments (B). (Courtesy of Pearl E. Grimes, MD.) |
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


