Kidney Transplantation in the Obese Recipient
Randall S. Sung
DEFINITION
Kidney transplantation is the preferred method of renal replacement therapy for obese patients with end-stage renal disease (ESRD).1 Compared to dialysis, advantages of kidney transplant include prolonged survival and improved quality of life. Kidney transplant outcomes are inferior to nonobese recipients, which not only provide incentives for weight modification but also challenge optimal recipient selection practices.2
PATIENT HISTORY AND PHYSICAL FINDINGS
As with other types of kidney transplants, those in the obese can only be performed at accredited transplant centers.
The history is similar to other kidney transplant candidates. A thorough history should be performed. With respect to obesity, the history of weight gain and loss should be elicited. Previous weight reduction efforts, particularly recent efforts, should be recorded. Evidence of recent success in weight reduction or recent weight gain may provide insight as to the success of future efforts. Weight may be affected by the fluid retention associated with ESRD onset or by recent initiation of dialysis.
Selection criteria vary widely, and there is no body mass index (BMI) beyond which transplantation does not provide a survival benefit compared with dialysis. Selected individuals with BMI greater than 50 have been successfully transplanted.
Obesity is a risk factor for adverse transplant outcomes. These include short-term outcomes such as surgical site infection (which carries a high risk for graft failure3) and long-term outcomes such as cardiovascular disease. As such, from a risk perspective, it should be considered along with other comorbidities when determining transplant candidacy.
For candidates with multiple comorbidities and risk factors in addition to obesity, lesser degrees of morbid obesity may confer added risk that makes transplantation inadvisable.
Conversely, morbidly obese candidates without significant comorbidities may be considered candidates provided the surgical or technical risk is not prohibitive.
All obese candidates should be counseled with respect to options for weight reduction including dietary, pharmacologic, and surgical modalities.
A full physical should be performed, with particular attention to weight distribution.
With respect to surgical difficulty, BMI is a poor indicator of risk because weight distribution varies considerably.
Assessment of the difficulty of surgery is mostly focused on the size and shape of the abdomen, particularly the lower abdomen, and the degree to which abdominal contents can be retracted away from the expected transplant site. Simulation of retraction of the abdomen provides valuable information.
In general, patients with flatter abdomens who carry excess weight elsewhere are less problematic than those who carry excess weight intraabdominally.
The anticipated depth from skin incision to iliac vessels is relevant as well, so that larger recipients are more difficult than smaller recipients at any given BMI. It should be recognized, however, that iliac artery depth cannot be reliably assessed by physical exam.
Patients with significant obesity who are considered to be candidates should be encouraged in weight reduction and have their weight monitored to ensure that no further weight is gained that might jeopardize transplant candidacy.
Any patient judged to not be a kidney transplant candidate on the basis of obesity, whether in whole or in part, should have the opportunity for reassessment in the event of successful weight reduction. Goals for weight reduction should be provided by the transplant team.
IMAGING AND OTHER DIAGNOSTIC STUDIES
There are no diagnostic studies that are specific to the obese transplant candidate. Morbid obesity may impair the ability to evaluate femoral pulses on physical exam, which is an important part of assessment for iliac arterial disease. In this case, other diagnostic studies to evaluate iliac arterial flow may be warranted. Otherwise, preoperative workup is similar to other kidney transplant candidates.
SURGICAL MANAGEMENT
Preoperative Planning
Operative planning is focused on preparation for difficulties unique to obese transplant recipients. Availability of long instruments and retractor blades (FIG 1); careful attention to cleansing and preparing the operative area thoroughly; and having sufficient personnel to be able to move and position the patient, place the Foley catheter, and so forth are all important.
 FIG 1 • Long right-angle blade for Bookwalter retractor compared with longest standard blade. |
Positioning
Positioning is supine and similar to other kidney transplant recipients.
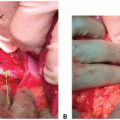
If the recipient has significant pannus even when supine, the location of the incision on the abdomen may require some deliberation, and the abdomen should be inspected with the pannus both in its natural position and retracted cephalad (FIG 2A). One option is to locate the incision inferior to the pannus. In this setting, the pannus may require retraction and fixation by adhesive tape or other measure. Alternatively, if the pannus is more mobile, the incision may be made through the pannus—this may result in a less deep incision and also carries the advantage of being located in an area of skin where hygiene is likely to be better (FIG 2B).
Although preferences vary, many surgeons prefer to place the kidney on the right side in obese recipients, as the right external iliac vein is sometimes less deep in the pelvis compared with the left external iliac vein.
Standard skin preparation should be used. Cefazolin is appropriate for preoperative antibiotics.
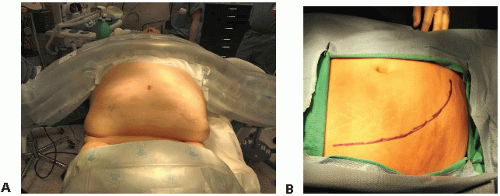 FIG 2 • A. The pannus can be left in place or retracted superior and medial. In this case, the pannus is not retracted to make the incision. B. The incision length required depends on the depth of the iliac vessels and the pelvis, the width of the pelvic brim, and the mobility of the abdominal wall and peritoneal contents. |
TECHNIQUES
BACKBENCH OF THE KIDNEY
Backbench preparation of the kidney is similar to that for nonobese recipients.
The kidney is prepared under sterile conditions on ice.
The perinephric fat is removed and the parenchyma inspected.
The artery and veins are inspected and are cleared of surrounding tissue, with ligation and division of nonrenal branches.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree