Jejunum Flap for Pharyngeal Reconstruction
Farooq Shahzad
Babak J. Mehrara
DEFINITION
The free jejunal flap is a workhorse for reconstruction of the hypopharynx and cervical esophagus.
A flap of up to 20 cm can be harvested on a single jejunal vessel and its vascular arcade. This length limits the use of this flap for reconstruction of subtotal or total esophageal defects.
For subtotal or total esophageal reconstruction, pedicled colon or gastric pull-up procedures are more appropriate in most cases.
However, both of these options have limited reach cephalad and may not extend all the way to the pharynx. In this situation, they can be combined with a free jejunal flap for the pharyngeal and cervical esophageal part of the reconstruction.
Alternatively, total esophageal reconstruction can also be performed with a pedicled jejunal flap (pedicled in the abdominal donor site) with supercharging the distal flap arcade in the neck or chest.1
ANATOMY
The jejunum is the second part of the small intestine. It starts from the ligament of Treitz and extends to the ileum.
The lumen of the jejunum contains circular mucosal folds called plicae circulares.
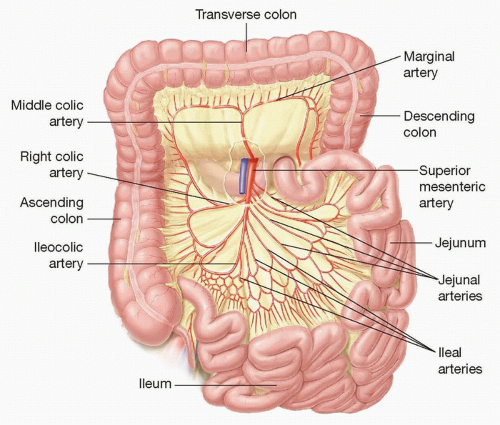
FIG 1 • Anatomy of the jejunum and intestines.
These folds slow down the passage of food and increase the surface area for absorption.
They decrease in size and number distally along the small bowel.
The blood supply of the small bowel is via the superior mesenteric artery. It gives rise to multiple jejunal and ileal branches (FIG 1).
These branches divide and form vascular loops called arcades.
These arcades further divide to form secondary and tertiary arcades.
The terminal vessels that supply the small bowel area are called the vasa recta.
The veins accompany the arteries.
A jejunal flap can be based on any jejunal artery and its accompanying vascular arcade. Free jejunal flaps are typically based on the ideal vascular arcade as defined by the recipient site needs (see below).
PATIENT HISTORY AND PHYSICAL FINDINGS
The history and physical exam should identify those patients who are not eligible for the operation.
Contraindications include chronic intestinal disease (eg, Crohn disease), ascites, and grave medical condition precluding a long operation.
Relative contraindications include multiple previous abdominal surgeries and limited pulmonary reserve.
Other donor sites are assessed for potential backup options, including the pectoralis flap, internal mammary artery perforator (IMAP) flap, deltopectoral flap, supraclavicular flap, radial or ulnar forearm flaps, and anterolateral thigh (ALT) flap.
Patients with thrombotic tendencies should be identified. This includes a history of deep vein thrombosis (DVT) or miscarriages or family history of thromboembolism.
A hypercoagulability workup and hematology consult can be obtained if necessary.
IMAGING
In general, no specific imaging is needed.
A mesenteric angiogram can be performed to evaluate the patency of the vascular pedicle in patients suspected of having atherosclerotic occlusive disease. However, this is rarely done as the superior mesenteric artery is typically spared from atherosclerosis.
SURGICAL MANAGEMENT
Jejunal free flap is most commonly used for circumferential defects of the cervical esophagus.
It can also be used to patch smaller defects or repair incomplete defects, but in these situations, we prefer the radial forearm or ALT flaps.
The ALT free flap is also a good option for circumferential pharyngoesophageal defects.
The donor site for this flap usually requires a split-thickness skin graft, however, and is, in our opinion, more morbid than a jejunum flap. In addition, tubing an ALT flap results in an extra suture line (in addition to the proximal and distal pharyngeal anastomosis) requiring more surgical time and potentially increasing the risk of leak.
As a result, we use this flap as a second-line option when the jejunum cannot be used. However, this idea is heavily debated.
In patients who are not free flap candidates (medical condition necessitating a short operation or no available recipient neck vessels), regional pedicled flaps like the pectoralis major myocutaneous flap or supraclavicular flap are more commonly used.
Preoperative Planning
The plan for resection and neck dissection should be discussed with the ablative head and neck surgeon. This allows for a better understanding of the anticipated surgical defect so that a reconstructive plan can be developed. Furthermore, an informed discussion can be held with the patient, and appropriate consent can be obtained.
It is also important to discuss the need for preservation of recipient vessels with the ablative surgeon.
Preoperative bowel preparation can be performed. Often, a simplified bowel prep with clear liquid diet for 24 hours and a bottle of magnesium citrate the day before surgery is all that is necessary.
Positioning
The patient is placed in the supine position for the duration of the case.
Perioperative antibiotic prophylaxis is performed. We use cefazolin and metronidazole for head and neck cases.
Sequential compression devices are used for DVT prophylaxis. Underbody warming device is used to prevent hypothermia during the case.
The face and neck are prepped with an iodine-based solution.
The chest and abdomen are prepped with a chlorhexidine-based or iodine-based solution.
The entire field is draped as one for convenience.
The chest can be covered with a drape or towel to prevent heat loss.
Approach
The jejunal flap can be harvested via an open or a laparoscopic approach.
Open harvest of the jejunal flap is our preferred method. It is performed via a midline epigastric incision. Generally, we make an 8-cm incision above the umbilicus.
This technique is technically easier and expeditious and allows direct visualization of the flap and pedicle.
Moreover, the pedicle can be separated in situ prior to flap harvest, which is easier to perform than after pedicle division and cuts down on ischemia time.
Laparoscopic-assisted harvest of the jejunal flap is performed via multiple small laparoscopic incisions.2 It requires expertise in minimally invasive techniques.
This usually means that the assistance of a general surgeon is required for flap harvest.
The advantage is decreased abdominal wall morbidity.
The jejunum tolerates ischemia for approximately 2 to 2.5 hours. Thus, meticulous planning and expeditious execution are critical for a successful outcome.
Hypothermia increases the ischemic tolerance of jejunal flaps, and some experts have described improved ischemic tolerance with cooling the flaps to 5°C,3 6°C to 12°C,4 and 10°C.5 This is generally not necessary, as ischemia times are kept less than 2 hours if the recipient vessels are prepared and the team is ready to perform microsurgical anastomosis when the flap is harvested. In fact, some suggest that 2 hours of euthermic ischemia time is beneficial for postoperative outcomes as this approach may decrease mucous production.6
TECHNIQUES
▪ Free Jejunum Reconstruction After Laryngopharyngectomy
Preparation of Recipient Area
The extirpative defect is analyzed.
The length of the hypopharyngeal/esophageal defect is measured, and a determination is made whether it is amenable to reconstruction with free jejunal flap (TECH FIG 1).
If not, an alternate method of reconstruction is chosen.
Recipient vessels in the neck are dissected and prepared.
The recipient artery and vein should be located close to each other because the donor vessels in a jejunal flap cannot be very widely separated.
The recipient artery is usually the superior thyroid, facial, or lingual artery.
The recipient vein is usually a branch of the internal jugular vein, the main trunk of the internal jugular vein (end to side), or the external jugular vein.
However, any suitable artery or vein situated close together may be used.
It is important to dissect the recipient vessels first (ie, prior to flap dissection) because the location of the vessels in relation to the defect determines flap design (see below).
If there is pedicle bleeding or other problems during flap harvest, the flap can be immediately harvested, inset, and revascularized without additional increases in ischemia time.
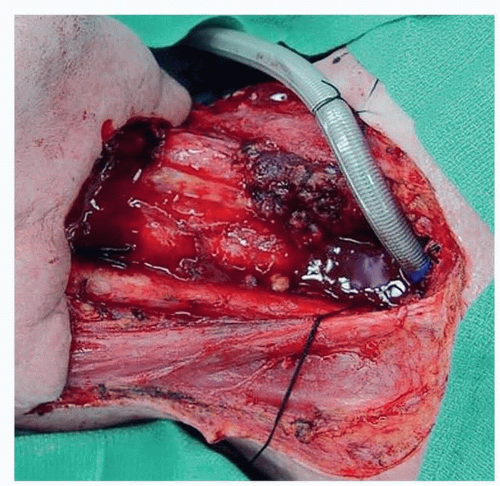 TECH FIG 1 • Defect after laryngopharyngectomy. Note wide skin excision and resection of the pharynx. |
▪ Jejunal Flap Harvest
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


