Chapter 1
Introduction
1.1Anatomy of the Anterior Abdominal Wall
1.4The History of Hernia Surgery
1.5Repair Principles and Materials
1 Introduction
1.1 Anatomy of the Anterior Abdominal Wall
A large gap exists in the human skeleton between the lower border of the thorax and the upper border of the bony pelvis. This extensive gap is closed by the multilayered abdominal wall, which consists of broad muscles, fasciae, aponeuroses, and peritoneum. The soft abdominal wall allows the thorax and entire trunk to move freely. It provides less protection to the intra-abdominal organs than the bony skeleton, but this is compensated by pronounced abdominal muscle reflexes.
The muscle layers of the abdominal wall consist of intrinsic muscles, namely the external oblique, internal oblique, and transversus abdominis laterally and the rectus abdominis and pyramidalis anteriorly. These muscles are fixed within the bony frame formed by the thorax, pelvis, and costal processes of the lumbar vertebrae and are completed by characteristic fasciae and connective tissue systems.
At certain typical sites, the abdominal wall contains no muscle and consists only of connective tissue. These anatomical sites of lower resistance are the hernial orifices that warrant surgical attention.
1.1.1 Muscles of the Abdominal Wall
Refer to22,30 and78 for related literature.
The Rectus Abdominis Muscle
![]() Origin. It originates by three slips from the anterior surface of the fifth to seventh costal cartilage. Near the midline, it forms the entire thickness of the anterior abdominal wall with the insignificant pyramidalis anterior to its lower end. The lateral slip is the widest and arises from the anterior surface of the fifth costal cartilage as far as the osteochondral junction. In many cases, the fibers of this muscle slip pass obliquely in an inferomedial direction. The intermediate slip originates from the anterior surface of the sixth costal cartilage, and the medial slip from the anterior surface of the seventh costal cartilage and anterior surface of the xiphoid process. Furthermore, the medial slip extends around the ascending border of the seventh costal cartilage to attach to its posterior surface. The fibers of the intermediate and medial slips pass in purely longitudinal direction as far as the first tendinous intersection.
Origin. It originates by three slips from the anterior surface of the fifth to seventh costal cartilage. Near the midline, it forms the entire thickness of the anterior abdominal wall with the insignificant pyramidalis anterior to its lower end. The lateral slip is the widest and arises from the anterior surface of the fifth costal cartilage as far as the osteochondral junction. In many cases, the fibers of this muscle slip pass obliquely in an inferomedial direction. The intermediate slip originates from the anterior surface of the sixth costal cartilage, and the medial slip from the anterior surface of the seventh costal cartilage and anterior surface of the xiphoid process. Furthermore, the medial slip extends around the ascending border of the seventh costal cartilage to attach to its posterior surface. The fibers of the intermediate and medial slips pass in purely longitudinal direction as far as the first tendinous intersection.
![]() Insertion. The rectus abdominis muscle is inserted by a strong flat tendon on the upper border of the pubic symphysis and adjacent parts of the superior pubic ramus. The lateral and medial parts of the tendon are quite different: the average length of the tendon is 4 to 5 cm laterally but only 2 to 3 cm medially. The junction does not form a continuous line from lateral to medial but occurs abruptly at one point (
Insertion. The rectus abdominis muscle is inserted by a strong flat tendon on the upper border of the pubic symphysis and adjacent parts of the superior pubic ramus. The lateral and medial parts of the tendon are quite different: the average length of the tendon is 4 to 5 cm laterally but only 2 to 3 cm medially. The junction does not form a continuous line from lateral to medial but occurs abruptly at one point ( Fig. 1.1). Lateral to this point, the rectus sheath is inserted on the anterior border of the superior pubic ramus, while medially the tendon is inserted on the medial surface of the pubic tubercle and extends onto the anterior surface of the pubic symphysis.
Fig. 1.1). Lateral to this point, the rectus sheath is inserted on the anterior border of the superior pubic ramus, while medially the tendon is inserted on the medial surface of the pubic tubercle and extends onto the anterior surface of the pubic symphysis.
Some of the fibers cross the midline to the contralateral pubic tubercle, where they mingle and cross at an acute angle. A few aberrant fibers pass to the suspensory ligament of the penis. In addition to extending between fixed cranial and caudal bony points, the medial border of the rectus abdominis is also inserted in the linea alba. This “medial insertion” is particularly prominent below the umbilicus; it becomes stronger inferiorly, forming the adminiculum lineae albae. The firm attachment of the rectus abdominis to the linea alba prevents the two rectus muscles from diverging, a condition known as diastasis of the recti.
![]() Tendinous intersections. The entire rectus abdominis structure is intersected by tendinous bands, resulting in a muscle with four bellies.
Tendinous intersections. The entire rectus abdominis structure is intersected by tendinous bands, resulting in a muscle with four bellies.
The tendinous intersections are true tendons with longitudinal fibers, which are firmly adherent to the anterior layer of the rectus sheath but are mobile over the posterior layer. The anterior adhesions prevent the muscle from moving as a whole within the rectus sheath, while allowing the individual sections to move in isolation.
On average, there are four intersections at the following positions:
• First intersection: at the level of the tip of the eighth rib.
• Second intersection: at the level of the lower border of the 10th rib.
• Third intersection: at the level of the umbilicus.
• Fourth intersection: inconstant, at the level of the arcuate line.
The tendinous intersections are up to 1 cm wide, have a zigzag or oblique course, and are firmly adherent medially to the linea alba and anteriorly to the anterior layer of the rectus sheath.
![]() Neurovascular supply. The arterial supply to the rectus abdominis muscle is from the superior and inferior epigastric arteries. These vessels lie in an obvious groove on the posterior surface of the muscle and extend lengthwise on the muscle. A continuous large-lumen connection between the two arteries, as shown in many atlases of anatomy, does not usually exist.
Neurovascular supply. The arterial supply to the rectus abdominis muscle is from the superior and inferior epigastric arteries. These vessels lie in an obvious groove on the posterior surface of the muscle and extend lengthwise on the muscle. A continuous large-lumen connection between the two arteries, as shown in many atlases of anatomy, does not usually exist.
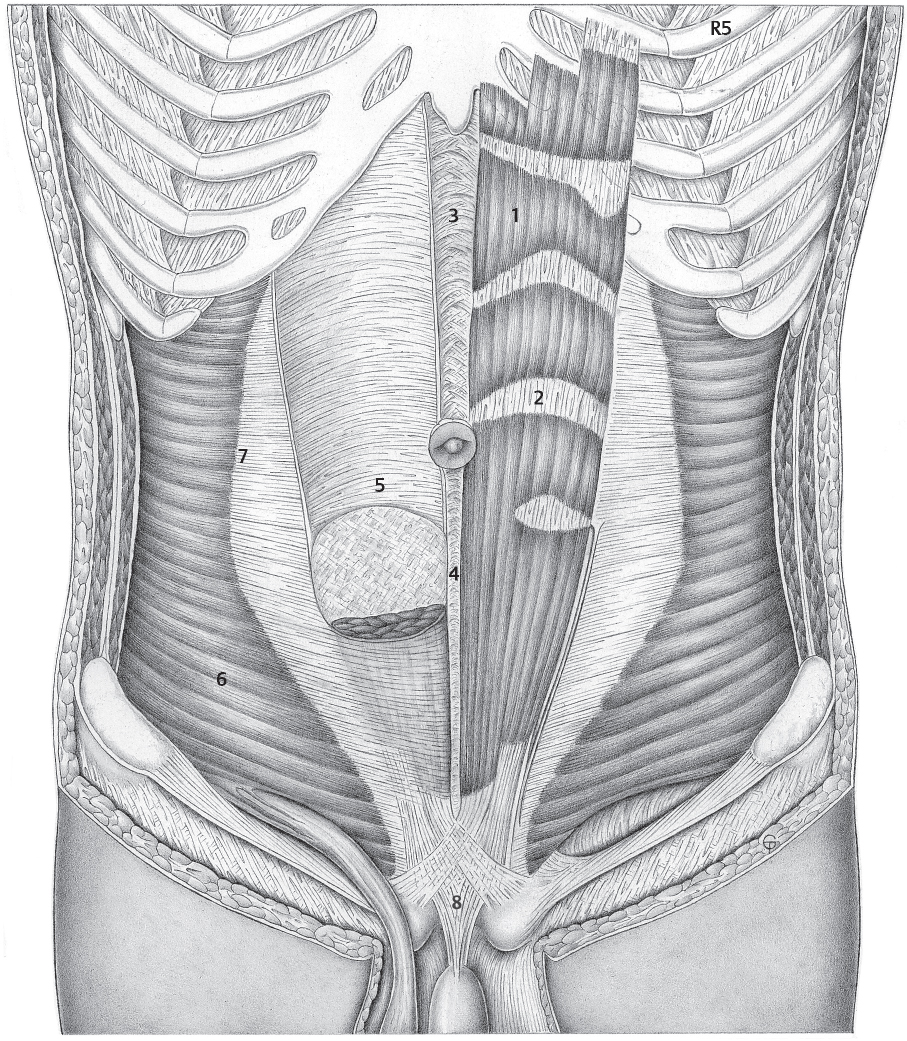
Fig. 1.1 Rectus abdominis and transversus abdominis (R5 = fifth rib).
1 Rectus abdominis.
2 Tendinous intersection.
3 Linea alba: broad part.
4 Linea alba: narrow part.
5 Posterior layer of the rectus sheath with arcuate line (of Douglas).
6 Transversus abdominis.
7 Linea semilunaris (Spieghel line).
8 Suspensory ligament of the penis.
The nerve supply is through the anterior rami of T7 to T12, often supplemented by accessory branches from T6 and L1.62 The muscular branches enter the lateral border and posterior surface of the muscle in 12 to 25 separate branches. Because of this position, the innervation is destroyed by a lateral incision.30
The External Oblique Muscle
![]() Origin. The external oblique muscle arises from the 5th to the 12th rib, forming a characteristic line that runs from the costochondral junction of the 5th rib to the rudimentary cartilage of the 12th rib. The muscle origin consists of slips that interdigitate superiorly with serratus anterior and inferiorly with latissimus dorsi. The resulting jagged line, which is clearly visible in the living, is called Gerdy’s line (Pierre Nicolas Gerdy, 1797–1856, anatomy and physiology prosector and later professor of surgery in Paris).
Origin. The external oblique muscle arises from the 5th to the 12th rib, forming a characteristic line that runs from the costochondral junction of the 5th rib to the rudimentary cartilage of the 12th rib. The muscle origin consists of slips that interdigitate superiorly with serratus anterior and inferiorly with latissimus dorsi. The resulting jagged line, which is clearly visible in the living, is called Gerdy’s line (Pierre Nicolas Gerdy, 1797–1856, anatomy and physiology prosector and later professor of surgery in Paris).
The dentations of the external oblique muscle increase in size from above as far as the 8th rib and then become smaller but thicker. The slips of the muscle’s origin overlap like roof tiles. The anterior boundary is smooth superiorly but often wavy inferiorly ( Fig. 1.2). At about the level of the anterior superior iliac spine, it turns at a right angle to become the muscle’s inferior border, which follows the iliac crest, thereby forming the Gaupp muscle corner (Ernst Gaupp, 1865–1916, professor of anatomy in Freiburg, Königsberg and Breslau;
Fig. 1.2). At about the level of the anterior superior iliac spine, it turns at a right angle to become the muscle’s inferior border, which follows the iliac crest, thereby forming the Gaupp muscle corner (Ernst Gaupp, 1865–1916, professor of anatomy in Freiburg, Königsberg and Breslau;  Fig. 1.2,
Fig. 1.2,  Fig. 1.3), which will be discussed further in connection with the inguinal canal.
Fig. 1.3), which will be discussed further in connection with the inguinal canal.
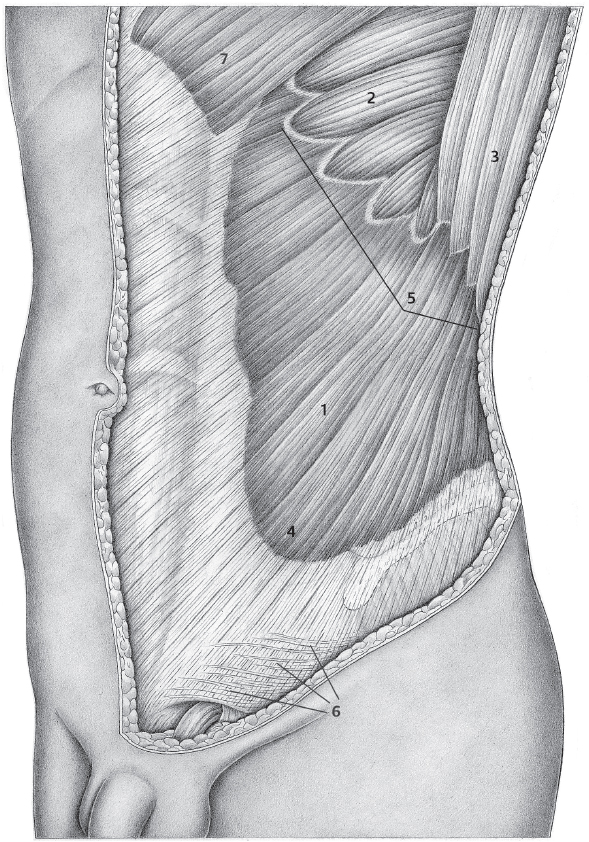
Fig. 1.2 External oblique muscle.
1 External oblique muscle.
2 Serratus anterior.
3 Latissimus dorsi.
4 Gaupp muscle corner.
5 Gerdy’s line.
6 Intercrural fibers.
7 Pectoralis major.
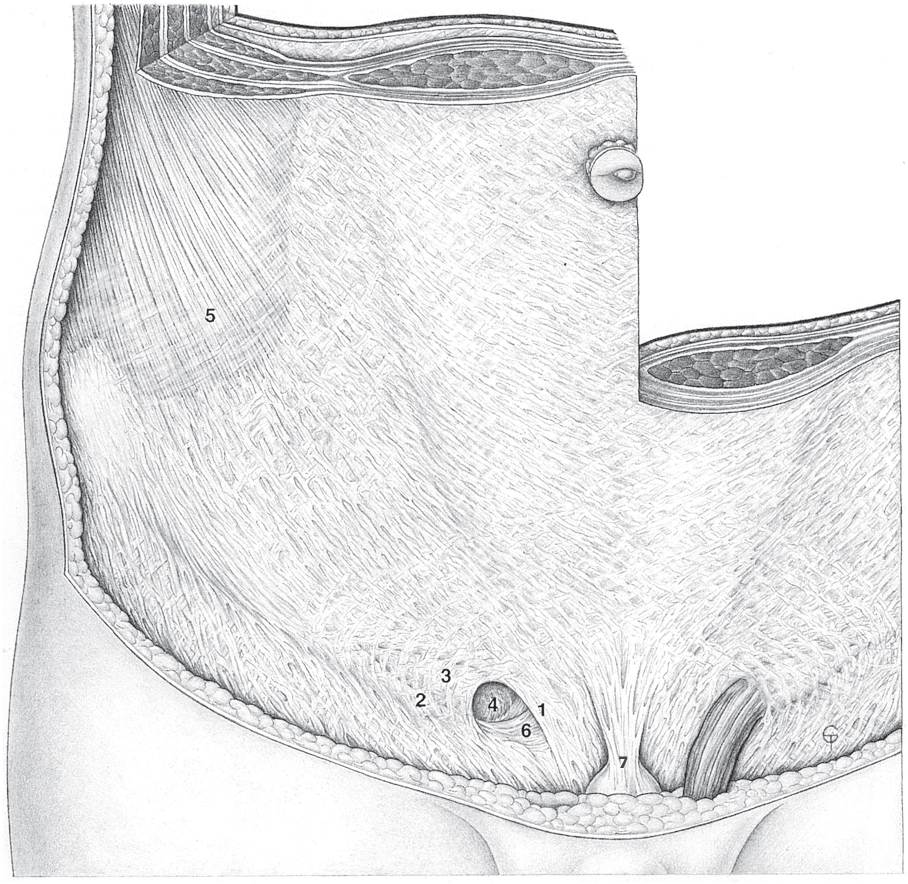
Fig. 1.3 Anatomy of the lower abdominal wall in the plane of the external oblique.
1 Medial crus.
2 Lateral crus.
3 Intercrural fibers.
4 Superficial inguinal ring.
5 External oblique muscle (Gaupp muscle corner).
6 Lacunar (Gimbernat) ligament.
7 Suspensory ligament of the penis.
![]() Insertion. The external oblique muscle is inserted on the outer lip of the iliac crest, pubic tubercle, and linea alba. It inserts in the iliac crest through a short strong tendon. Anteriorly, the muscle is continuous with its extensive aponeurosis, the inferior border of which forms the inguinal ligament. This ligament extends from the anterior superior iliac spine to the pubic tubercle, becoming wider from lateral to medial portion (
Insertion. The external oblique muscle is inserted on the outer lip of the iliac crest, pubic tubercle, and linea alba. It inserts in the iliac crest through a short strong tendon. Anteriorly, the muscle is continuous with its extensive aponeurosis, the inferior border of which forms the inguinal ligament. This ligament extends from the anterior superior iliac spine to the pubic tubercle, becoming wider from lateral to medial portion ( Fig. 1.11).
Fig. 1.11).
![]() Direction of fibers. In the upper part of the muscle, the fibers run almost horizontally but slant increasingly downward in the inferior portion. This fiber direction (
Direction of fibers. In the upper part of the muscle, the fibers run almost horizontally but slant increasingly downward in the inferior portion. This fiber direction ( Fig. 1.2) continues in the connective tissue fibers of the aponeurosis. These aponeurotic fibers cross the midline and interlace with the contralateral fibers. In the inferior part of the linea alba, they form two layers on the opposite side: the superficial layer radiates into the fascia lata through the adductor longus muscle, whereas the deep layer is inserted on the pubic tubercle, forming the reflected inguinal ligament (Colles’ ligament; after Abraham Colles, 1773–1843, professor of anatomy and surgery in Dublin; see also inguinal canal and inguinal ligament).
Fig. 1.2) continues in the connective tissue fibers of the aponeurosis. These aponeurotic fibers cross the midline and interlace with the contralateral fibers. In the inferior part of the linea alba, they form two layers on the opposite side: the superficial layer radiates into the fascia lata through the adductor longus muscle, whereas the deep layer is inserted on the pubic tubercle, forming the reflected inguinal ligament (Colles’ ligament; after Abraham Colles, 1773–1843, professor of anatomy and surgery in Dublin; see also inguinal canal and inguinal ligament).
The fibers that pass in the inferior muscle border from the anterior superior iliac spine to the muscle corner merit attention as they form the inguinal ligament (Poupart ligament; after François Poupart, 1616–1708, surgeon in Reims and Paris). Above the iliopsoas muscle, this ligament constitutes a stronger band within the iliac fascia, because of which it cannot be separated from the iliopsoas muscle fascia (see inguinal ligament).
![]() Neurovascular supply. The muscle is innervated by anterior branches of T5 to T12 and sometimes also L1. The blood supply comes from the deep circumflex iliac artery, the inferior and superior epigastric arteries, the musculophrenic artery, and the lateral thoracic artery.
Neurovascular supply. The muscle is innervated by anterior branches of T5 to T12 and sometimes also L1. The blood supply comes from the deep circumflex iliac artery, the inferior and superior epigastric arteries, the musculophrenic artery, and the lateral thoracic artery.
The Internal Oblique Muscle
![]() Origin. The internal oblique muscle arises from the intermediate line of the iliac crest, from the superficial layer of the thoracolumbar fascia, and from the lateral part of the inguinal ligament. The muscle can be described as a five-sided curved sheet (
Origin. The internal oblique muscle arises from the intermediate line of the iliac crest, from the superficial layer of the thoracolumbar fascia, and from the lateral part of the inguinal ligament. The muscle can be described as a five-sided curved sheet ( Fig. 1.4). The origin is typically S-shaped with its main bend at the anterior superior iliac spine.
Fig. 1.4). The origin is typically S-shaped with its main bend at the anterior superior iliac spine.
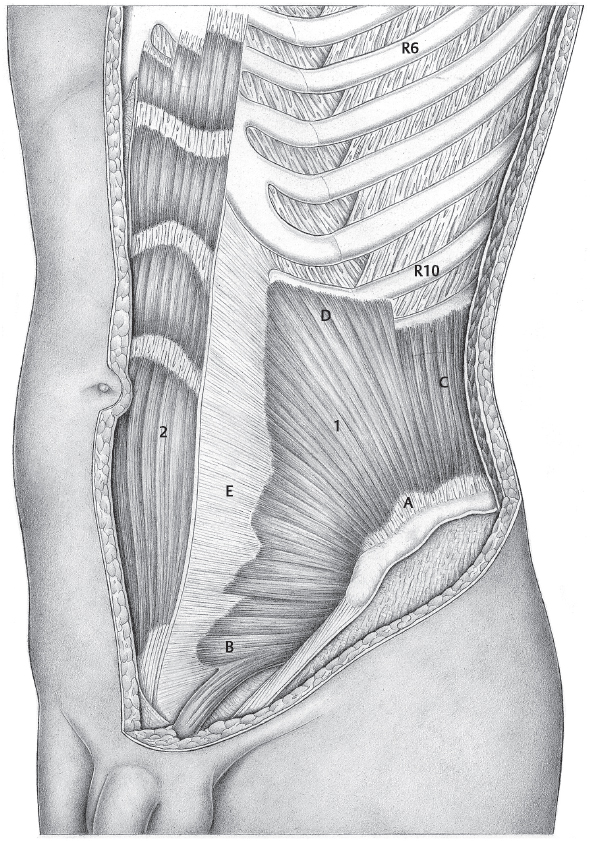
Fig. 1.4 Internal oblique muscle with its five borders.
1 Internal oblique muscle.
A S-shaped origin.
B Inferior border with diverging fibers.
C Vertically ascending posterior border. D Stepped superior border.
E Medial border with inferior dentations.
2 Rectus abdominis muscle.
The posterior border passes vertically upward from the iliac crest to the superior border, where it is inserted.
![]() Insertion. The internal oblique muscle is inserted superiorly and anteriorly:
Insertion. The internal oblique muscle is inserted superiorly and anteriorly:
• The superior border extends from the tip of the 10th costal cartilage to the tip of the 12th costal cartilage and has a variable course depending on the shape of the ribs ( Fig. 1.4).
Fig. 1.4).
• The anterior border forms the longest side of the muscle and describes a line that extends from the pubic tubercle to the tip of the 10th rib. In its inferior part, it typically has small dentations, the lowest of which projects furthest medially ( Fig. 1.4).
Fig. 1.4).
![]() Direction of fibers. This varies between the individual parts of the muscle. The fibers that originate between the anterior superior iliac spine and the gluteal tubercle diverge greatly. The fibers of the adjacent inferior part of the muscle have a parallel course, whereas the fibers arising from the lateral inguinal ligament run almost horizontally but possibly irregularly.
Direction of fibers. This varies between the individual parts of the muscle. The fibers that originate between the anterior superior iliac spine and the gluteal tubercle diverge greatly. The fibers of the adjacent inferior part of the muscle have a parallel course, whereas the fibers arising from the lateral inguinal ligament run almost horizontally but possibly irregularly.
The insertion of the internal oblique muscle is through a short flat tendon. The anterior border merges with the broad aponeurosis of the internal oblique muscle. It is important to note that the collagen fibers of the aponeurosis maintain the direction of the muscle fibers and therefore have three sections, like the muscle. At the lateral border of the rectus abdominis the aponeurosis forms the rectus sheath, which will be described in more detail in section The Rectus Sheath (page 9).
The internal oblique muscle is enclosed between a thin superficial fascia and a thick, feltlike, deep fascia. The superficial fascia is clearly distinct from the muscle and can also be separated from the deep fascia of the external oblique. The deep fascia of the internal oblique is very difficult to distinguish as a separate layer and merges with the superficial fascia of the transversus abdominis muscle. Sometimes, the two layers can be separated close to the inguinal canal. The superficial internal oblique fascia forms the middle spermatic fascia. When the inguinal part of the internal oblique muscle is particularly bulky, these fibers are forced apart when a hernia is present. Some of these fibers then extend inferiorly on the hernial sac.
![]() Neurovascular supply. The segmental nerves (T8–L1) and vessels (especially branches of the deep circumflex iliac artery and vein) run in the deep and thick connective tissue layer. This structural arrangement is altered in the inguinal part, where the segmental nerves and vessels perforate the internal oblique muscle and run on its surface in inferomedial direction. According to Eisler,62 the internal oblique is supplied by T10–L2. The nerves enter the muscle from its underside.
Neurovascular supply. The segmental nerves (T8–L1) and vessels (especially branches of the deep circumflex iliac artery and vein) run in the deep and thick connective tissue layer. This structural arrangement is altered in the inguinal part, where the segmental nerves and vessels perforate the internal oblique muscle and run on its surface in inferomedial direction. According to Eisler,62 the internal oblique is supplied by T10–L2. The nerves enter the muscle from its underside.
The Transversus Abdominis Muscle
![]() Origin. The transversus abdominis muscle originates from the six lower ribs as well as from the deep layer of the thoracolumbar fascia, the inner lip of the iliac crest, and the psoas fascia. It also regularly extends to the lateral part of the inguinal ligament.
Origin. The transversus abdominis muscle originates from the six lower ribs as well as from the deep layer of the thoracolumbar fascia, the inner lip of the iliac crest, and the psoas fascia. It also regularly extends to the lateral part of the inguinal ligament.
![]() Insertion. The transversus abdominis is inserted in the linea alba, the xiphoid process, the cranial border of the pubic symphysis, and the adjacent medial part of the pecten pubis.
Insertion. The transversus abdominis is inserted in the linea alba, the xiphoid process, the cranial border of the pubic symphysis, and the adjacent medial part of the pecten pubis.
The transversus abdominis can be regarded as a direct inferior continuation of the transversus thoracis muscle. It is therefore not surprising that variations in the origin of the transversus abdominis are closely linked with variations in the prominence of the transversus thoracis. When the inferior part of the transversus thoracis is less developed, the origin of the transversus abdominis is correspondingly higher and vice versa.
![]() Direction of fibers. The fibers run parallelly and horizontally, with the anterior segments curving downward in the inferior region. According to Eisler,62 the overall shape of the transversus abdominis can be compared with a crescent moon, with its concavity facing anteriorly. At this muscle border, the transversus abdominis is continuous with its aponeurosis, which forms part of the rectus sheath, discussed in section The Rectus Sheath (page 9).
Direction of fibers. The fibers run parallelly and horizontally, with the anterior segments curving downward in the inferior region. According to Eisler,62 the overall shape of the transversus abdominis can be compared with a crescent moon, with its concavity facing anteriorly. At this muscle border, the transversus abdominis is continuous with its aponeurosis, which forms part of the rectus sheath, discussed in section The Rectus Sheath (page 9).
The junction between the muscle and its connective tissue aponeurosis is called the semilunar (spigelian) line (after Adriaan van den Spieghel, Spigelius in Latin, 1578–1625, professor of anatomy in Venice and Padua; see  Fig. 1.1). It is important to note that the horizontal direction of the muscle fibers continues in the horizontal fibers of the aponeurosis. Cranially, the aponeurosis crosses the anterior surface of the xiphoid process to which it is partly adherent, but also passes to the contralateral side, leading to the interlacing of the fibers.
Fig. 1.1). It is important to note that the horizontal direction of the muscle fibers continues in the horizontal fibers of the aponeurosis. Cranially, the aponeurosis crosses the anterior surface of the xiphoid process to which it is partly adherent, but also passes to the contralateral side, leading to the interlacing of the fibers.
Another group of fibers is inserted anterior to the transversus thoracis on the lateral segments of the root of the xiphoid process. The inferior muscle fibers that pass downward continue into the corresponding tendon fibers that pass almost parallel to the lateral border of the rectus abdominis behind the reflected inguinal (Colles) ligament to the pecten pubis. According to Eisler,62 three layers of fibers can be detected in this region of the transversus abdominis:
• Superficial layer: passes anteriorly over the rectus abdominis and pyramidalis and is inserted in the linea alba and pubic symphysis.
• Middle layer: between pyramidalis and rectus abdominis.
• Deep layer: passes with its fibers beside the rectus abdominis to the pecten pubis.
The outer surface of the muscle is covered by its fascia and by a thick connective tissue layer, and the inner surface is covered by its posterior muscle fascia and the strong transversalis fascia.
![]() Neurovascular supply. The transversus abdominis is innervated by the branches of T530 with an occasional contribution from the iliohypogastric and ilioinguinal nerves. The nerves supplying the muscle are on its outer surface initially and form looping anastomoses during their intramuscular course. The blood supply is provided by the deep circumflex iliac artery, the inferior and superior epigastric arteries, and by the musculophrenic artery.
Neurovascular supply. The transversus abdominis is innervated by the branches of T530 with an occasional contribution from the iliohypogastric and ilioinguinal nerves. The nerves supplying the muscle are on its outer surface initially and form looping anastomoses during their intramuscular course. The blood supply is provided by the deep circumflex iliac artery, the inferior and superior epigastric arteries, and by the musculophrenic artery.
1.1.2 Fasciae and Fascial Structures
The division, in the older nomenclature, of the superficial abdominal fascia into a superficial layer (subcutaneous fascia or Camper fascia, after Peter Camper, 1722–1789, professor of anatomy, surgery and medicine in Amsterdam and Groningen) and a deep layer, the actual superficial abdominal fascia (or Scarpa fascia, after Antonio Scarpa, 1747–1832, professor of anatomy and surgery in Modena and Padua), will continue to be used here, although it is no longer given in the new Terminologia Anatomica.221
The terms “fatty layer of the abdomen” and “membranous layer of the abdomen,” introduced in place of the previous names for the fascial structures, have not yet entered the clinical parlance and are rather confusing. “Fatty layer of the abdomen” does not at all reflect the obvious structure of the connective tissue framework of the subcutaneous fat layer. This is not a simple fat pad; moreover, in quadrupeds this structural layer forms a thick elastic fascia (“yellow abdominal skin”). So comparative anatomy also argues for the retention of the term “fascia.”
Subcutaneous (Camper) Fascia or Fatty Layer of the Abdomen
Below the umbilicus in the aponeurotic region of the anterior abdominal wall and on the rectus sheath, there is a dense structure of elastic tissue, perforated like a honeycomb, which becomes visible only when the fat within it is expressed.180 This formation, part of the subcutaneous tissue, is called the subcutaneous fascia (Camper) or fatty layer of the abdomen.
Cranially, this fascia is gradually dissipated and disappears. Laterally, it is firmly connected to the fascia of the external oblique muscle and terminates in this. Inferiorly, by contrast, it splits into a superficial and a deep layer. These layers behave differently: the superficial layer merges with the fascia lata and the deep layer terminates in the inguinal ligament.
The structure is also noteworthy medially, where again the fascia splits into several layers. The deep layers become adherent with the linea alba while the superficial layers cross to the contralateral side and connect to the skin, which appears retracted along the midline, especially in obese persons. In front of the pubic symphysis, the subcutaneous fascia forms the elastic fundiform ligament of the penis or clitoris. An important topographical feature of this ligament is its presence in front of the linea alba, the insertion of the rectus muscles, and the suspensory ligament of the penis.
Superficial Abdominal Fascia (Scarpa fascia) or Membranous Layer of the Abdomen
The superficial abdominal fascia is the name given to the tough connective tissue layer containing numerous elastic fibers that lies on the external oblique muscle. This fascia continues on the aponeurosis but here it becomes thin and nonmobile. Typical fiber directions can be identified within the abdominal fascia. Fibers coming from the anterior superior iliac spine run concentrically around the corner of the external oblique muscle, pass upward parallel to the border of the rectus, and then turn medially to terminate on the rectus sheath.8,9,10,11,12,50,78,145,222,235
At the costal margin, strong fiber systems form, which pass over the xiphoid process to terminate on the contralateral side. The fibers arising from the lateral part of the inguinal ligament constitute a system that fans out over the slit formed by the inferior and superior crura and terminates on the rectus sheath. These fibers are termed intercrural fibers. These are usually very poorly developed in women and are otherwise very variable. The intercrural fibers are not involved in forming the superficial inguinal ring. Rather, this is closed laterally by fascial fibers arising from the medial part of the inguinal ligament.
It is important to note that the superficial abdominal fascia continues as a thin layer on the spermatic cord, thus forming the external spermatic fascia (cremasteric fascia, Cooper fascia, after Sir Astley Paston Cooper, 1768–1841, professor of anatomy and surgery in London).
Below the inguinal ligament, the superficial abdominal fascia is continuous with the fascia lata. The fascia lata divides into two layers over the femoral vessels, which lie in the iliopectineal fossa. The deeper layer corresponds to the iliopectineal fascia on the lateral side of the (superficial) femoral artery. The superficial layer forms the lateral, curved border of the fossa ovalis through which the great saphenous vein passes (falciform margin with superior and inferior horns). Because of the doubling of the fascia lata, the superficial layer forms the cranial limb and the inferior curved margin of the fossa ovalis and is inserted with the deep layer on the pectineal fascia and pecten pubis. This deep portion of the fascia lata helps strengthen the medial wall of the femoral canal.
In the author’s opinion, there is no need or anatomical justification for distinguishing another connective tissue layer from the superficial abdominal (Scarpa) fascia, named the Gallaudet fascia.73,180,209
The Rectus Sheath
The rectus sheath is a flat connective tissue tube containing the rectus abdominis muscle. This sheath consists of anterior and posterior laminae that are adherent with one another medially and laterally (see  Fig. 1.6,
Fig. 1.6,  Fig. 1.10).62
Fig. 1.10).62
The posterior layer is absent superiorly, where the rectus abdominis lies on the thorax. As far as the ninth costal cartilage, the posterior layer consists essentially of the aponeurosis of the transversus abdominis as the posterior layer of the internal oblique aponeurosis is extremely thin. The typical structure of the posterior layer only forms below the level of the ninth costal cartilage, where the rectus sheath consists of the posterior layer of the internal oblique aponeurosis, the transversus abdominis aponeurosis, and the transversalis fascia.
The posterior lamina occupies the upper two-thirds of the rectus sheath and then undergoes a major transformation: roughly 4 to 6 cm below the umbilicus, the posterior layer of the internal oblique aponeurosis and the transversus abdominis aponeurosis pass into the anterior lamina of the sheath. The transition area is marked by the inferior concave border of the aponeurosis where it passes forward and is known as the arcuate line or semicircular line of Douglas (after James Douglas, 1675–1742, anatomist and gynecologist in London). The arcuate line is classically described as situated 4 to 5 cm inferior to the umbilicus but it may be encountered as far as 9 cm below it.
The aponeurotic fibers often do not switch abruptly from posterior to anterior but form a transitional zone so the arcuate line can also be regarded as an area. Spigelian hernias are found where the arcuate line crosses the semilunar (Spieghel) line. Below the arcuate line, the posterior lamina consists only of transversalis fascia and is therefore very thin and delicate. It should also be noted that the inferior part, consisting only of transversalis fascia, is firmly adherent to the linea alba and therefore continues onto the posterior surface of the adminiculum lineae albae, finally inserting in the pubic bone. Because of this, the posterior lamina is approximately 1 cm from the posterior surface of the rectus abdominis inferiorly, with development of a fat-filled submuscular space (the Charpy retromuscular fossa, after Adrien Charpy, 1848–1911, professor of anatomy in Toulouse).
The anterior lamina of the rectus sheath comprises two segments with differing structure. As far as the arcuate line the anterior lamina consists of the external oblique aponeurosis and the anterior layer of the internal oblique aponeurosis. Below the arcuate line, it is joined by the posterior layer of the internal oblique aponeurosis and the aponeurosis of the transversus abdominis.
It is noteworthy that the external oblique aponeurosis does not merge with the anterior layer of the internal oblique aponeurosis immediately at the lateral border of the rectus sheath, but this fusion takes place more medially on the rectus sheath. The area where they merge moves more medially in inferior direction and finally almost coincides with the linea alba.
The space within the rectus sheath is divided into anterior and posterior parts. The anterior part is in front of the rectus abdominis and is further divided by adhesion of the tendinous intersections to the anterior lamina. The anterior space does not communicate with the space behind the muscle at the lateral border of the rectus muscle as connective tissue fibers from the lateral border of the muscle attach firmly to the lateral area where the anterior and posterior laminae fuse, thereby completing the separation. This subdivision of the space within the rectus sheath is important for the spread of pathological processes and effusions.
The Linea Alba
The linea alba (see  Fig. 1.1) is a connective tissue raphe formed by the aponeuroses of the abdominal muscles where they meet in the midline. It is approximately 35 to 40 cm in length. The linea alba starts on the anterior surface of the xiphoid process with the interlacing of the cranial fibers of the transversus abdominis and local fascia. Inferiorly, the linea alba is inserted on the pubic tubercle and many of its fibers merge with the adductor fascia. Two large segments of differing texture can be distinguished in the linea alba:62
Fig. 1.1) is a connective tissue raphe formed by the aponeuroses of the abdominal muscles where they meet in the midline. It is approximately 35 to 40 cm in length. The linea alba starts on the anterior surface of the xiphoid process with the interlacing of the cranial fibers of the transversus abdominis and local fascia. Inferiorly, the linea alba is inserted on the pubic tubercle and many of its fibers merge with the adductor fascia. Two large segments of differing texture can be distinguished in the linea alba:62
• The cranial part, extending to about 4 to 5 cm below the umbilicus, consists of a very thin band, roughly 1 to 2.5 cm wide, where the aponeurotic fibers interlace in both sagittal and frontal direction.
• The inferior part, which extends to the symphysis, is characterized by an absence of the sagittal fiber component. So, it appears as a very narrow but thick band.
The adminiculum lineae albae is at the lower end of the linea alba. This structure begins at the arcuate line and becomes wider inferiorly, resulting in a triangular lamella, formerly termed the triangular ligament. The adminiculum lineae albae is posterior to the rectus abdominis muscles and is attached to the superior ramus of the pubic bone posterior to the rectus tendons. The anteromedial ridge of the adminiculum lineae albae passes between the two rectus muscles and is connected to the visible anterior band of the linea alba.
The broad superior part of the linea alba contains the umbilicus and accessory openings may also be present. These openings arise due to divergence of the fibers, with the small rectangular openings become rounded owing to the circular extension of the fibers. The accessory openings, found only above the umbilicus, contain a fat plug which is connected to the subperitoneal fat tissue. These accessory gaps and the umbilicus are potential sites for linea alba and umbilical hernias.
The complex architecture of the linea alba fibers can be divided into three distinct layers, from anterior to posterior:13,14
• Oblique fibers.
• Transverse fibers.
• Irregular fibers.
Unlike previous researchers, the authors have not found any separate areas of interlacing of fibers. It is also interesting that sexual dimorphism is found in the fibrous architecture of the linea alba:14 there are considerably more transverse fibers in the infraumbilical region in women than in men. This can probably be regarded as a functional adaptation.
The topography of the superior linea alba insertion on the xiphoid process is of particular surgical importance. Incision of the posterior lamina of the rectus sheath beside the xiphoid provides access to the retroxiphoid space. This space contains loose, delicate preperitoneal fat limited superiorly by the diaphragm, which can be readily extended by blunt dissection to enable combined retromuscular and retroxiphoid positioning of a sublay mesh.46
When the posterior layer of the rectus sheath is opened more inferiorly directly beside the linea alba, the preperitoneal fat space is reached. This space appears as a fat-filled triangular area described by Conze et al47 as the fatty triangle. The fatty triangle likewise allows retromuscular mesh positioning with adequate overlapping areas.
The Transversalis Fascia
The transversalis or endoabdominal fascia (of Luschka, after Hubert von Luschka, 1820–1875, initially an apothecary, then a general physician, and finally professor of anatomy in Tübingen), which covers the entire inner surface of the anterior abdominal wall, is an important structure in the abdominal wall and inguinal and femoral regions ( Fig. 1.5). In the inguinal region, it consists of a series of arches that extend up to the arcuate line and are bounded inferiorly by the femoral vessels. The transversalis fascia is a connective tissue layer of greatly variable thickness, which is difficult to demonstrate by dissection.
Fig. 1.5). In the inguinal region, it consists of a series of arches that extend up to the arcuate line and are bounded inferiorly by the femoral vessels. The transversalis fascia is a connective tissue layer of greatly variable thickness, which is difficult to demonstrate by dissection.
The transversalis fascia is firmly adherent to the subserous connective tissue of the peritoneum and lies on the transversus muscle and its aponeurosis. (Note: the transversalis fascia is not the same as the transversus aponeurosis.) A little above the umbilicus, the transversalis fascia forms the thicker, stronger, and denser umbilical fascia.166 The umbilical fascia is thus a special part of the transversalis fascia, where the fibers run horizontally. The umbilical fascia disappears gradually superiorly, whereas its inferior margin often has a sharp curved margin that is concave inferiorly. The peritoneum is immovable on the umbilical fascia.
The inferior part of the transversalis fascia has special relations. It is reinforced here by the iliopubic tract and attaches to the entire posterior surface of the inguinal ligament, where it helps to form the posterior wall of the inguinal canal, the deep inguinal ring, and the femoral ring. The position where the spermatic cord enters the inguinal canal, the transversalis fascia is continuous with the delicate spermatic fascia, thereby forming the processus vaginalis of the transversalis fascia. The medial border of this fascial funnel is usually sharp, whereas the superolateral margin is more rounded and concave. The sharp medial border is also called the Krause semilunar fold of the transversalis fascia (after Wilhelm Johann Friedrich Krause, 1833–1910, professor of anatomy in Göttingen and Berlin). On the lateral third of the inguinal ligament, the transversalis fascia is continuous with the iliac part of the iliopsoas fascia.
It is generally accepted that only the transversalis fascia separates the dorsum of the rectus muscles from the peritoneum. The transversalis fascia is variously described as:
• Aponeurosis.
• Membrane.
• Thickened fat layer.
• Extraperitoneal boundary layer.
The transversalis fascia is the deep layer that forms the boundary with the peritoneum and also covers the abdominal surface of the transversus abdominis and its aponeurosis. It lies on the fascia of the rectus abdominis, quadratus lumborum, and iliopsoas muscles and of the diaphragm. With these muscle fasciae, it forms a large sac that completely underlies the peritoneum. Close to the kidneys, this fascial tissue contains abundant perirenal fat. Within the pelvis, it is called the paracolpium, paraproctium, paracystium, and parametrium.84 There is very little fat around the umbilicus and on the diaphragm; the fascia is loose and vascular in the inguinal canal, where it contains the blood vessels and nerves lying on the internal spermatic fascia.
Since the structure of the transversalis fascia differs greatly in different regions, the abdominal wall and inguinal regions are discussed separately below.
Transversalis Fascia on the Abdominal Wall
The transversalis fascia varies in firmness and thickness both inter- and intra-individually. In general, the transversalis fascia is particularly thin in the upper abdomen and particularly thick on the lateral abdominal wall. However, it is most pronounced in the inguinal region. According to Velpeau, two layers can be distinguished in the transversalis fascia. The deep layer corresponds to the peritoneal lamella and the superficial layer to the transversus fascia, which cannot always be demonstrated.
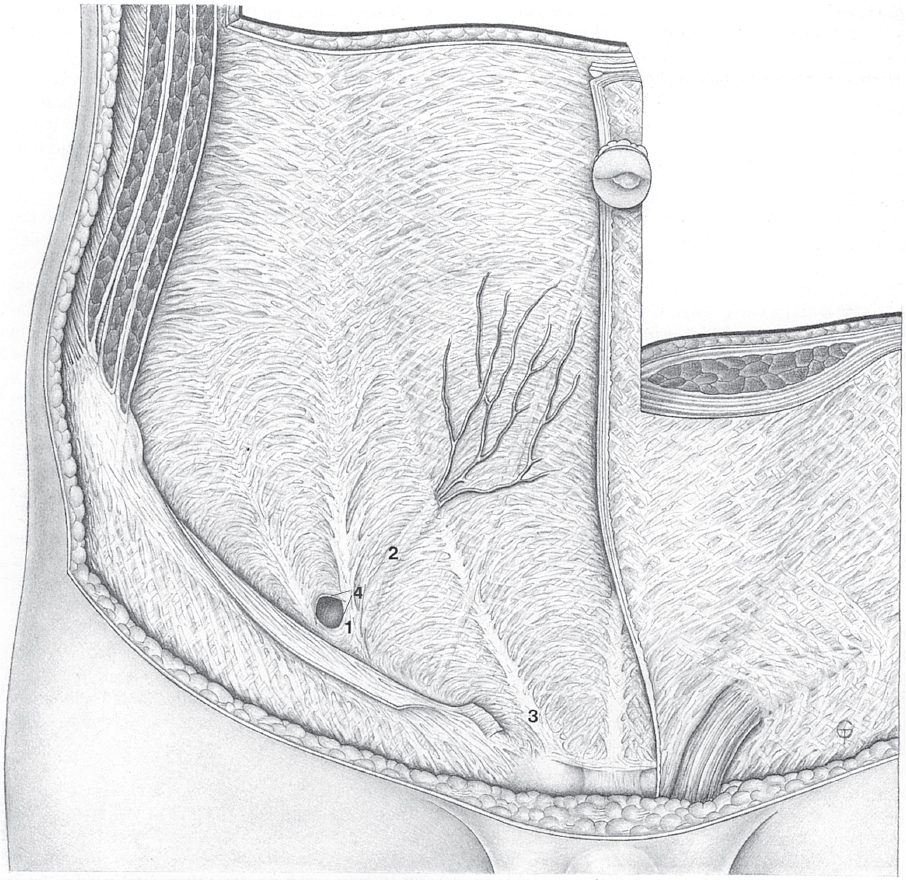
Fig. 1.5 Anatomy of the lower abdominal wall in the transversalis fascia plane. The Hesselbach triangle between 1, 2 and 3 has a lattice-like structure.
1 Henle loop.
2 Interfoveolar (Hesselbach) ligament.
3 Curved rectus margin.
4 Semilunar line.
The superficial layer is “soldered” to the transversus abdominis aponeurosis and passes with this in front of the rectus abdominis. Here, it further divides into two layers to enclose the pyramidalis muscle. The deep layer (Velpeau lamina propria, after Alfred Armand Louis Marie Velpeau, 1795–1867, renowned French surgeon) of the transversalis fascia constitutes a mobile layer between the pure muscle fascia and the (peritoneal) fascia. This layer (the peritoneal lamella) remains behind the rectus abdominis and forms the posterior lamella of the rectus sheath ( Fig. 1.5). Medially, the interfoveolar ligament of Hesselbach (after Franz Kaspar Hesselbach, 1759–1816, prosector at the Juliusspital in Würzburg) provides an obvious boundary to the Velpeau lamina propria. Medial to this ligament, it is no longer possible to dissect any continuous fascia.
Fig. 1.5). Medially, the interfoveolar ligament of Hesselbach (after Franz Kaspar Hesselbach, 1759–1816, prosector at the Juliusspital in Würzburg) provides an obvious boundary to the Velpeau lamina propria. Medial to this ligament, it is no longer possible to dissect any continuous fascia.
Transversalis Fascia in the Inguinal Region
The transversalis fascia forms a posterior lining for the entire inguinal region.8,9,10,12,34,50,78,145,222 At the deep inguinal ring, it continues on the spermatic cord as the internal spermatic fascia. Certain transversalis fascia structures are distinguished in the inguinal region:
• The transversalis fascia loops at the deep inguinal ring (Henle loop, after Friedrich Gustav Jakob Henle, 1809–1885, professor of anatomy in Zürich, Heidelberg, and Göttingen).
• Internal spermatic fascia, the continuation on the spermatic cord.
• The vascular sheath of the inferior epigastric artery and vein.
• The area in the linea alba where it is interlaced with fibers from the contralateral side.
• The iliopubic tract (Thomson ligament, after Allen Thomson, 1809–1884, professor of anatomy in Aberdeen and Glasgow, and for a time professor of physiology in Edinburgh).
The spermatic cord or round ligament of the uterus passes through the abdominal wall lateral to the interfoveolar (Hesselbach) ligament. These structures are enclosed by a U-shaped loop that opens superiorly (the transversalis loop;  Fig. 1.5,
Fig. 1.5,  Fig. 1.6). Curved fibers pass laterally and medially from this transversalis loop. Contraction of the transversalis loop is believed to close the deep inguinal ring. This contraction depends on the functional status of the musculature. Paralysis or insufficiency, e.g., following trauma or surgery, opens the deep inguinal ring and fosters hernia development. The loop is continuous superiorly with an upper limb and inferiorly with a lower limb, which lies above the iliopubic tract.
Fig. 1.6). Curved fibers pass laterally and medially from this transversalis loop. Contraction of the transversalis loop is believed to close the deep inguinal ring. This contraction depends on the functional status of the musculature. Paralysis or insufficiency, e.g., following trauma or surgery, opens the deep inguinal ring and fosters hernia development. The loop is continuous superiorly with an upper limb and inferiorly with a lower limb, which lies above the iliopubic tract.
The iliopubic tract (Thomson ligament) only becomes visible from the front following division of the inguinal ligament. Its fibers run parallel to those of the inguinal ligament initially and then continue inferiorly into the femoral vascular sheath.
The transversalis fascia extends upward from the inguinal region in four groups of fibers (columns):
• First column: The connective tissue fibers cross in the linea alba and attach to the pubic symphysis at the adminiculum lineae albae. Fibers branch off from the linea alba to form arches in the posterior layer of the rectus sheath, passing in convex curves from this column into the rectus sheath. It is clear from these fibers that the transversalis fascia, and not the transversus abdominis aponeurosis, is involved ( Fig. 1.5).
Fig. 1.5).
• Second column: This is at the lateral border of the rectus abdominis. Curved fibers pass laterally and medially, thereby forming a mesh between adjacent vertical columns.
• Third column: This sometimes contains the epigastric vessels. Curved bundles of fibers also branch off from it, passing laterally and medially and forming a vaulted lattice.
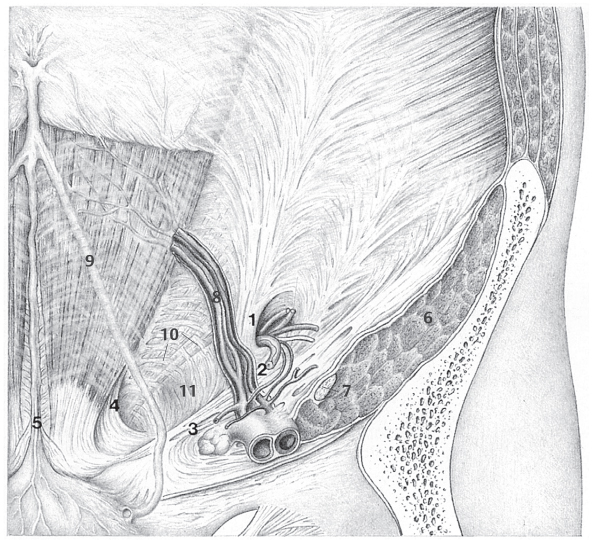
Fig. 1.6 Anatomy of the inguinal and femoral regions from behind including potential hernial orifices, the vertical columns, and the Hesselbach triangle.
1 Henle loop at the spermatic cord and deep inguinal ring.
2 Interfoveolar (Hesselbach) ligament.
3 Inguinal (Poupart) ligament.
4 Inguinal falx and rectus border.
5 Linea alba and medial umbilical fold.
6 Iliopsoas muscle.
7 Femoral nerve.
8 Inferior epigastric vessels.
9 Lateral umbilical fold.
10 Transversus border, the “white line.”
11 The Hesselbach triangle.
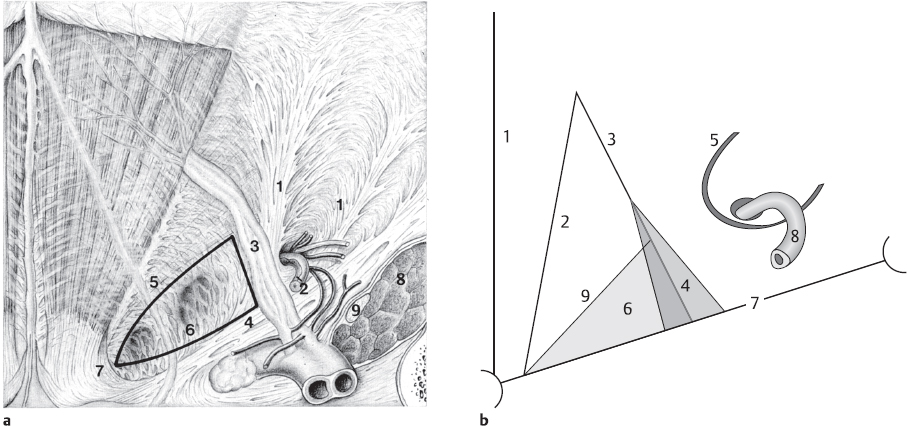
Fig. 1.7 a and b.
a Anatomical location of a direct (= medial) inguinal hernia in the Hesselbach triangle.
1 Henle loop.
2 Vas deferens.
3 Interfoveolar ligament.
4 Inguinal ligament.
5 Transversus border.
6 Hesselbach triangle.
7 Inguinal falx and rectus margin.
8 Iliopsoas muscle.
9 Femoral nerve.
b Diagram of the Hesselbach triangle.
1 Linea alba.
2 Lateral rectus margin, inguinal falx.
3 Epigastric vessels.
4 Interfoveolar ligament.
5 Henle loop.
6 The Hesselbach triangle.
7 Inguinal ligament.
8 Vas deferens.
9 Transversus muscle border.
• Fourth column: This contains the Henle (transversalis) loop at the deep inguinal ring.
The second and third columns are the boundaries of the Hesselbach triangle ( Fig. 1.6,
Fig. 1.6,  Fig. 1.7, and section
Fig. 1.7, and section  1.1.3.1).
1.1.3.1).
Peritoneum
The peritoneum is a serous membrane. Its parietal layer lines the entire abdominal and pelvic cavity, while the visceral layer is reflected over the surface of the intraperitoneal organs. The peritoneum consists of three layers:
• Mesothelium: This consists of a single layer of transformed connective tissue cells that behave like epithelium (with desmosomes, basal membrane, and microvilli). The mesothelium has fibrinolytic properties240 that can prevent the formation of peritoneal adhesions. Traumatized mesothelial cells lose their fibrinolytic activity; so, the feared postoperative adhesions cannot be effectively prevented.
• Lamina propria (or serosa): It contains collagenous and reticular connective tissue, along with numerous blood vessels, lymphatic capillaries, mechanoreceptors, and free nerve endings.
• Subserosa (preperitoneal connective tissue or preperitoneal fat tissue; see  Fig. 1.3): Subserosa contains many elastic fibers, can contain variable quantities of fat, and varies greatly in its orientation, firmness, and fiber content. The subserosa is separated from the firm or loose connective tissue of the abdominal wall fascia or retroperitoneal tissue by the transversalis fascia. The subserous layer confers mobility on the peritoneum.
Fig. 1.3): Subserosa contains many elastic fibers, can contain variable quantities of fat, and varies greatly in its orientation, firmness, and fiber content. The subserosa is separated from the firm or loose connective tissue of the abdominal wall fascia or retroperitoneal tissue by the transversalis fascia. The subserous layer confers mobility on the peritoneum.
• Parietal layer (periorchium).
• Visceral layer (epiorchium): covers all parts of the testis apart from the posterior surface and is inseparable from the tunica albuginea.
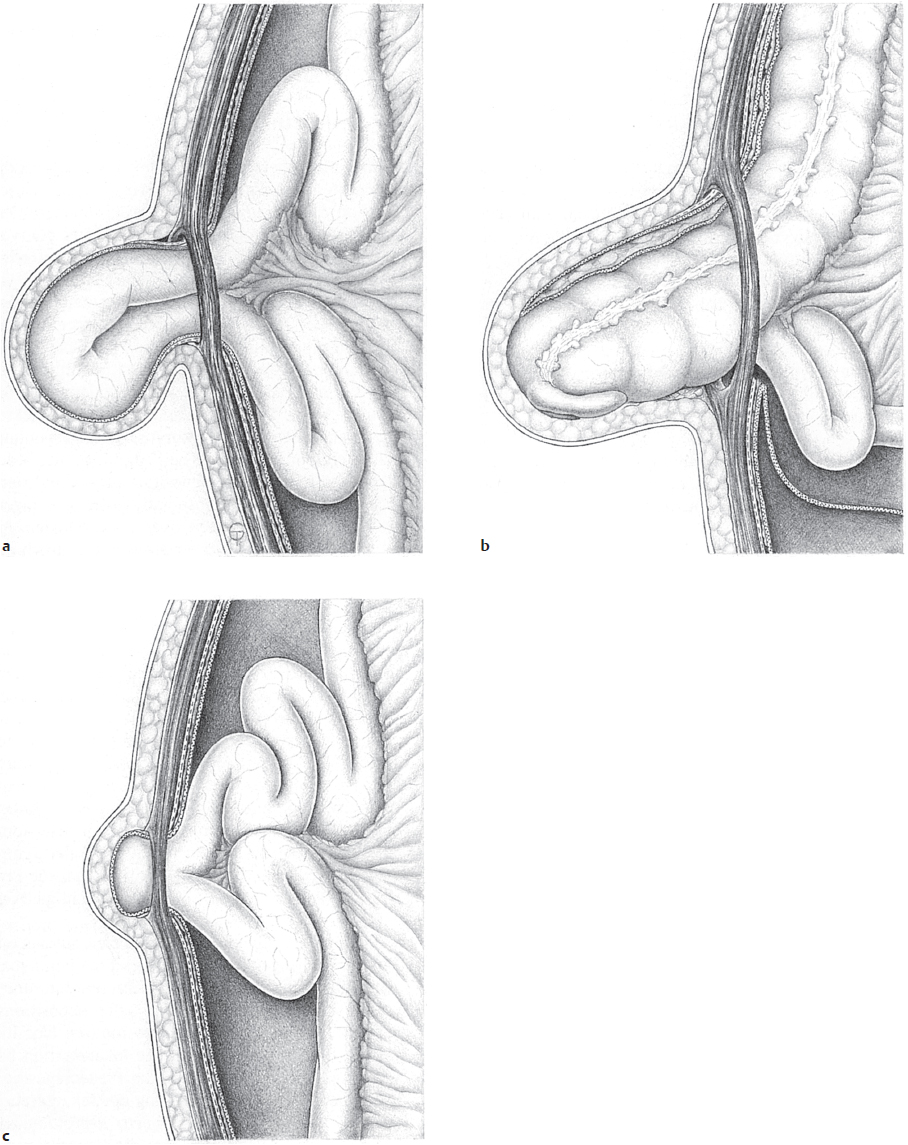
Between these two layers is the serous cavity of the scrotum, which surrounds the front and sides of the testis and contains small amounts of fluid. The connection between the scrotal and the peritoneal cavities is generally lost; so, the abdominal cavity is closed at the entrance to the inguinal canal. Persistence of the processus vaginalis can be manifested variously as:
• Congenital inguinal hernia: The hernia contents slide into the patent persistent processus vaginalis and are separated from the testis only by the visceral layer (epiorchium).
• Hydrocele of the spermatic cord: Part of the processus vaginalis persists within the spermatic cord. The secretory activity of the persistent mesothelium then results in a fluid-filled cyst.
The small physiological thimble-shaped outpouching of peritoneum into the female inguinal canal is called the canal or diverticulum of Nuck (after Anton Nuck, 1650–1692, professor of anatomy in Leiden), while the equivalent outpouching in the male fetus, which represents the start of processus vaginalis development, is called the Seiler pouch (after Burkhard Wilhelm Seiler, 1779–1843, professor of anatomy and surgery in Wittenberg).
Inguinal Ligament

Background
The nomenclature used here is guided by the precise studies of this region by Eisler62 and it was also used by Braus and Elze.30 It differs from the Terminologia Anatomica. Unfortunately, the nomenclature of many anatomical and surgical descriptions now varies greatly and is sometimes incorrect due to misunderstandings and redefinitions. So clear communication between researchers of this region encounters considerable difficulties, making further misunderstanding inevitable. To provide clarity at this point,  Table 1.1 contains a synopsis of the terms used.
Table 1.1 contains a synopsis of the terms used.
Hardly any anatomical structure has been treated as variously and contradictorily in the literature as the inguinal (Poupart) ligament (see  Fig. 1.11). Strictly speaking, this connective tissue structure is not a ligament, but a complex entity consisting of different components. The ligament is the inferior border of the external oblique aponeurosis and is in the same plane. It has an oblique course that varies between 35 and 40° to the horizontal axis of the abdomen. It is 12 to 14 cm long. Two distinct sections can be identified:
Fig. 1.11). Strictly speaking, this connective tissue structure is not a ligament, but a complex entity consisting of different components. The ligament is the inferior border of the external oblique aponeurosis and is in the same plane. It has an oblique course that varies between 35 and 40° to the horizontal axis of the abdomen. It is 12 to 14 cm long. Two distinct sections can be identified:
• Lateral one-third: This is formed by particularly dense parts of the iliopsoas fascia such that this part of the ligament is generally inseparable from the iliopsoas fascia. The fibers do not run directly medially but run more vertically and obliquely down to the iliopectineal fascia. In addition, the lateral one-third contains aponeurotic fibers from the internal oblique and transversus abdominis.
• Medial two-thirds: This is formed by the lower border of the external oblique aponeurosis, which is folded backward.
The bone fixation points are lateral to the anterior superior iliac spine (ASIS) and medial to the pubic tubercle. Spatial understanding of the “folded border” is essential, as this arises from the architecture of the lateral crus of the superficial inguinal ring: the superior fibers of the lateral crus are attached anteriorly to the pubic tubercle while the inferior fibers are shifted posteriorly. Since these fibers do not end on bone but pass briefly on and in the periosteum before separating from this, a groove open superiorly is formed. The fibers that pass cranially from the bone form the lacunar (Gimbernat) ligament (after Antonio Don de Gimbernat, 1734–1816, professor of anatomy in Barcelona and later professor of surgery in Madrid) or reflected (Colles) ligament.
The inguinal ligament is reinforced and stabilized by anterior and posterior groups of fibers:
• Anteriorly by the Scarpa fascia and its inferior continuation, the fascia lata.
• Posteriorly by the iliopubic tract (a reinforcement of the transversalis fascia, see section The Transversalis Fascia (page 10)), which extends from the ASIS to the pubic bone.
The fibers of the external oblique aponeurosis do not run strictly parallel to the inguinal ligament. The angle between them is often 10 to 20°. Every oblique fiber that enters the ligament passes medially and runs longitudinally within the ligament. Close to the ASIS, the aponeurotic fibers continue directly into the fascia lata. In the rest of the ligament, the fibers pass medially to the pubic tubercle.
Reinforced fibers from the iliopsoas fascia on the medial surface of the iliopsoas muscle leave the lateral one-third of the inguinal ligament and pass in a laterally concave curve to the iliopubic eminence. This band of fascia is called the iliopectineal arch; it separates the muscular from the vascular lacuna.
Table 1.1 Nomenclature of the ligaments in the inguinal ligament region
Structure | Eisler nomenclature62 | Terminologia Anatomica221 |
Ipsilateral fibers diverging cranially from the inguinal ligament | Lacunar ligament (Gimbernat ligament) | Reflected ligament (Colles ligament) |
Fibers of the contralateral external oblique aponeurosis | Reflected ligament (Colles ligament) | No name assigned |
Fibers diverging caudally from the inguinal ligament and forming the medial boundary of the vascular compartment | Falciform lacunar process | Lacunar ligament (Gimbernat ligament) |
The formation of the superficial inguinal ring is closely linked to the anatomy of the inguinal ligament. The fibers of the external oblique aponeurosis coming from the Gaupp muscle corner form two bands that diverge from one another inferomedially (see  Fig. 1.3). The inferior band is called the lateral crus and the superior band is the medial crus. The fibers of the lateral crus were described above; those of the medial crus terminate at the pubic tubercle.
Fig. 1.3). The inferior band is called the lateral crus and the superior band is the medial crus. The fibers of the lateral crus were described above; those of the medial crus terminate at the pubic tubercle.
It is important to note that the bony insertion of the lacunar ligament includes fibers from the contralateral external oblique, some of which enter the lacunar ligament, forming a groove in which the spermatic cord is embedded. The contralateral fibers are known as the reflected (Colles) ligament. In many nomenclatures, including the Terminologia Anatomica, no distinction is made between the ipsilateral and contralateral groups of fibers and the entire band of fibers is called the reflected ligament. Since this is a reduction of the anatomical situation as confirmed by dissection, the Eisler nomenclature will be followed at this point.
From the inferomedial end of the inguinal ligament, fibers pass caudally, forming a small connective tissue plate with a laterally concave border. Because of its half-moon shape, this structure is very accurately termed the falciform process of the lacunar ligament; it continues on the upper surface of the superior ramus of the pubis. The lacunar falciform process rounds the medial border of the vascular lacuna (or femoral ring). The lacunar falciform process is part of the inguinal ligament and therefore part of the external oblique aponeurosis. It is attached to the iliopectineal line. According to some authors,145 the lacunar falciform process (or lacunar ligament) does not form the medial border of the femoral ring. In this interpretation, the anterior border of the femoral ring is formed by the anterior layer of the fascia lata and not by the inguinal ligament.
Inguinal Falx (Conjoint Tendon)
Removal of the transversalis fascia reveals two highly variable structures, which are treated very differently and superficially in the literature. These are the inguinal falx and the interfoveolar (Hesselbach) ligament, which are discussed below. The inguinal falx is part of the transversus abdominis aponeurosis and lies on the posterior surface of the aponeurosis, which is thereby strengthened.
The inguinal falx is a triangular gusset of connective tissue with a sickle-shaped lateral border, which fuses medially with the lateral border of the rectus sheath and inserts widely on the inguinal ligament at its base. This insertion continues over the pectineal (Cooper) ligament onto the surface of the superior ramus of the pubis. According to Eisler’s studies, the term “ligament of Henle” introduced by K. M. Douglas59 designates an aberrant, tendinous strip of the transversus muscle that is inserted on the pecten pubis. The term should therefore not be used when referring to the inguinal falx.
Interfoveolar Ligament (of Hesselbach)
The interfoveolar (Hesselbach) ligament is a fibrous sheet that branches off the posterior surface of the transversus abdominis aponeurosis in the arcuate region, passes caudally and inserts in the inguinal ligament at the pecten pubis and on the lacunar ligament. The interfoveolar ligament separates the laterally situated deep inguinal ring from the medial inguinal fossa. The inferior epigastric vessels lie on the posterior surface. When well developed, fibers of the interfoveolar ligament can continue into the posterior rectus sheath.
The development of the interfoveolar ligament is linked with that of the inguinal falx and the iliopubic tract. When these two structures are very strongly established, they replace the interfoveolar ligament and vice versa. Both the inguinal falx and the interfoveolar ligament can be regarded as the pelvic insertion of the transversus abdominis. So it is not surprising that variable amounts of striated muscle fibers can be present within these structures. If muscle is visible macroscopically in the interfoveolar ligament, it is also referred to as the interfoveolar (Hesselbach) muscle.
1.1.3 Anatomical Regions and Hernial Orifices
Inguinal Canal with Superficial and Deep Inguinal Rings
The topographical connections between the structures described systematically and separately above will be discussed below. The inguinal canal, located above the inguinal ligament, is an artificial product of dissection created by removal of the spermatic cord or the round ligament of the uterus. It is a typical site of lower resistance in the abdominal wall.
The inguinal canal is 4 to 5 cm long (somewhat longer in women than in men) and crosses the abdominal wall obliquely from behind and above in front and below, at an angle of about 15° to the inguinal ligament. The “canal” starts inside at the deep inguinal ring and opens at the superficial inguinal ring (see  Fig. 1.3,
Fig. 1.3,  Fig. 1.6,
Fig. 1.6,  Fig. 1.8,
Fig. 1.8,  Fig. 1.13). Four walls are described in the inguinal canal:
Fig. 1.13). Four walls are described in the inguinal canal:
• The broad, thick anterior wall is formed by the external oblique aponeurosis with the lateral crus and medial crus.
• The broad but thin posterior wall is provided exclusively by the transversalis fascia. The variable inguinal falx and interfoveolar ligament may be involved in strengthening the posterior wall.
• The narrow superior wall is formed by the lowest fibers of the internal oblique and transversus abdominis, often replaced by connective tissue.
• The narrow inferior wall is formed by the curved border of the external oblique aponeurosis, the lacunar ligament, and the reflected ligament in the form of a connective tissue groove.
The inner opening of the inguinal canal is about 1 cm above the middle of the inguinal ligament in the lateral inguinal fossa, which is lateral to the epigastric fold. As a result, the inferior epigastric vessels and the interfoveolar ligament form the medial boundary of the deep inguinal ring. The oval slit of the deep inguinal ring only becomes visible after removal of the peritoneum and division of the Nuhn fascial funnel of the transversalis fascia, which continues on the spermatic cord as the internal spermatic fascia.
The superficial inguinal ring lies ca. 1 to 1.5 cm above the pubic tubercle and is bounded by the medial (or superior) crus and the lateral (or inferior) crus, but not by the intercrural fibers. The superficial abdominal fascia is attached to the fascial margins of the superficial inguinal ring and continues in a funnel shape on the spermatic cord as the external spermatic fascia. The superficial inguinal ring only becomes visible after sharp dissection of this fascia.
The spermatic cord passes through the inguinal canal in men and the round ligament of the uterus in women. The complicated layers of the spermatic cord arise because all layers of the abdominal wall are borne along with passage of the peritoneal processus vaginalis and testis, like fingers of a glove.  Table 1.2 lists the layers of the abdominal wall against their derivatives in the spermatic cord.
Table 1.2 lists the layers of the abdominal wall against their derivatives in the spermatic cord.
The nerves that pass through the inguinal canal are also important surgically: These include the ilioinguinal nerve and genital branch of the genitofemoral nerve (or external spermatic nerve). The ilioinguinal nerve enters the inguinal canal through the deep inguinal ring, often runs below the spermatic cord and leaves the inguinal canal in the medial angle of the superficial inguinal ring or through a separate opening in the medial crus. It then crosses the spermatic cord or round ligament in lateral direction and divides into its scrotal or labial branches. Less often, the ilioinguinal nerve passes through the lateral angle of the superficial inguinal ring, and in some cases, it does not pass through the superficial inguinal ring at all but exits cranial to this. The course of the nerve is outside the coverings of the testis. The ilioinguinal nerve provides the sensory innervation of the skin at the root of the penis and scrotum or of the labia majora and adjacent parts of the inner thigh.
The mixed genital branch of the genitofemoral nerve lies on the spermatic cord or round ligament and provides motor innervation to the cremaster muscle and sensory innervation to the skin of the scrotum or labia majora. In addition, it supplies the skin on the upper medial side of the thigh next to the scrotum. It regularly emerges through the superficial inguinal ring on the medial side of the spermatic cord.
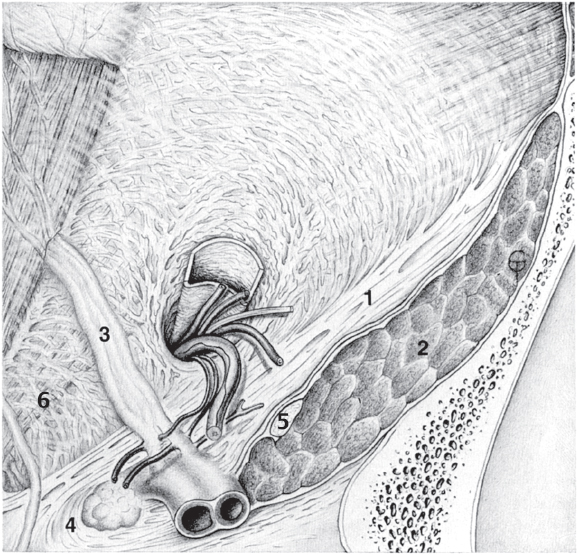
Fig. 1.8 Anatomical location of the indirect (lateral) inguinal hernia orifice (at the deep inguinal ring).
1 Inguinal ligament.
2 Iliopsoas muscle.
3 Inferior epigastric artery and vein.
4 Lacunar falciform process.
5 Femoral nerve.
6 Transversus border, the “white line.”
Table 1.2 Layers of the spermatic cord (from within outward)
Layers of the abdominal wall | Layers of the spermatic cord |
Peritoneum | Tunica vaginalis testis and vaginal ligament |
Extraperitoneal fat Transversalis fascia | Internal spermatic fascia (tunica vaginalis communis) |
Transversus abdominis Internal oblique | Cremaster |
Internal oblique fascia | Middle spermatic fascia |
External oblique fascia | External spermatic fascia (Cooper cremasteric fascia) |
Camper fascia | Dartos tunic |
Abdominal skin | Scrotal skin |
Anterior Abdominal Wall Relief
The topography of the inner surface of the anterior abdominal wall is important for understanding direct hernias, in particular. The relief of the inside of the abdominal wall is dominated by three cord-like structures (see  Fig. 1.6):
Fig. 1.6):
• Medial umbilical fold: It passes from the dome of the bladder to the umbilicus in the midline. It contains the obliterated urachus.
• Lateral umbilical fold: This is more lateral and contains the obliterated umbilical artery.
• Epigastric fold: This is even further laterally and contains the inferior epigastric vessels.
The nomenclature of these structures is not uniform and is summarized in  Table 1.3. Since “lateral umbilical fold,” the Terminologia Anatomica221 term for the fold raised by the epigastric vessels has nothing to do with the umbilicus, Thiel’s example224 is followed and the old term “epigastric fold” is retained, as this has the advantage of indicating the reason for its existence.
Table 1.3. Since “lateral umbilical fold,” the Terminologia Anatomica221 term for the fold raised by the epigastric vessels has nothing to do with the umbilicus, Thiel’s example224 is followed and the old term “epigastric fold” is retained, as this has the advantage of indicating the reason for its existence.
There are three more or less obvious depressions between the folds:
• Supravesical fossa between the middle umbilical fold and the lateral umbilical fold above the dome of the bladder.
• Medial inguinal fossa between the lateral umbilical fold and the epigastric fold.
• Lateral inguinal fossa lateral to the epigastric fold. This has already been mentioned as the location of the deep inguinal ring. Since indirect hernias enter the inguinal canal, it is clear that these hernias are lateral to the inferior epigastric vessels.
The medial inguinal fossa merits closer attention as it is the weakest part of the anterior abdominal wall. This weakness arises on the one hand because this site is muscle free but also because the external oblique aponeurosis outside it diverges in the form of the medial and lateral crus to form the superficial inguinal ring. This weak area above the inguinal ligament becomes a round to oval region with the addition of the weak vascular lacuna below the ligament, known in the literature as the myopectineal orifice of Fruchaud.
Table 1.3 Summary of umbilical fold nomenclature
Terminologia Anatomica 1998221 | Older nomenclature |
Median umbilical fold | Middle umbilical fold (unpaired) |
Medial umbilical fold | Lateral umbilical fold (paired) |
Lateral umbilical fold | Epigastric fold (paired) |
Strengthening of this important site of lower resistance can be achieved by the inguinal falx or interfoveolar ligament. The medial inguinal fossa is the internal orifice of direct hernias that appear externally at the superficial inguinal ring and are medial to the inferior epigastric vessels. The Hesselbach triangle (Hesselbach or inguinal trigone, after Franz Kaspar Hesselbach, 1759–1816, anatomist and surgeon in Würzburg), which is a key structure in understanding inguinal hernias and their surgical repair ( Fig. 1.6,
Fig. 1.6,  Fig. 1.7), is within the medial inguinal fossa. The Hesselbach triangle is bounded:
Fig. 1.7), is within the medial inguinal fossa. The Hesselbach triangle is bounded:
• Superiorly by the lower border of the transversus, which is often tendinous and thickened, forming the arch of the transversus aponeurosis, the surgeon’s “white line”.202
• Medially by the lateral border of the rectus abdominis (second vertical pillar).
• Laterally by the vascular sheath of the inferior epigastric artery and vein (third vertical pillar).
• Inferiorly by the inguinal ligament ( Fig. 1.7).
Fig. 1.7).
The apex of the triangle faces medially. The triangle is more obvious in men than in women, who have hardly any triangle on account of their shallow pelvis. This explains why direct inguinal hernias occur rarely in women.
Indirect hernias pass through the abdominal wall lateral to the epigastric vessels. Direct hernias pass through it medially in the center of the Hesselbach triangle. The aim of surgical repair is reconstruction of the lost fascial reinforcement of the posterior abdominal wall ( Fig. 1.8).
Fig. 1.8).
Muscular Lacuna
Unlike the inguinal canal, which lies above the inguinal ligament, the two orifices described below, the muscular and vascular lacunae, are present below the inguinal ligament.
The triangular space below the inguinal ligament but above the superior ramus of the pubis is divided into two segments by the iliopectineal arch (or ligament), which branches off the inguinal ligament and is inserted on the iliopubic ramus. The lateral segment is called the muscular lacuna and the medial is the vascular lacuna. The iliopectineal arch is a strip of the iliopsoas fascia, which must be demonstrated artificially; it may be reinforced by tendinous fibers of the inconstant psoas minor. The iliopsoas muscle passes through the muscular lacuna to the thigh together with the femoral nerve, which lies on the medial border of the iliopsoas.
The lateral cutaneous femoral nerve is in the upper lateral corner of the muscular lacuna. Since the iliopsoas fascia is firmly adherent to the inguinal ligament or is a separate component of the ligament, this means that the abdominal cavity is closed extremely strongly from the thigh at the muscular lacuna. Therefore, this orifice is rarely a site of hernia (e.g., the rare lateral Hesselbach femoral hernia,  Fig. 1.9).
Fig. 1.9).
Vascular Lacuna and Femoral Ring
The osteofibrous canal located medial to the iliopectineal arch below the inguinal ligament is called the femoral vascular lacuna (see  Fig. 1.6,
Fig. 1.6,  Fig. 1.13). The vascular lacuna is bounded superiorly and anteriorly by the inguinal ligament, inferoposteriorly by the pubic bone, and laterally by the iliopectineal arch. In the medial sharp angle between the insertion of the inguinal ligament on the pubic tubercle and the superior ramus of the pubis, the space is rounded off by the firm connective tissue lacunar falciform process. This structure is often termed the lacunar ligament of Gimbernat (
Fig. 1.13). The vascular lacuna is bounded superiorly and anteriorly by the inguinal ligament, inferoposteriorly by the pubic bone, and laterally by the iliopectineal arch. In the medial sharp angle between the insertion of the inguinal ligament on the pubic tubercle and the superior ramus of the pubis, the space is rounded off by the firm connective tissue lacunar falciform process. This structure is often termed the lacunar ligament of Gimbernat ( Fig. 1.10) but, as explained above, this should be reserved for a completely different structure.
Fig. 1.10) but, as explained above, this should be reserved for a completely different structure.
The lacunar falciform process has a laterally concave border and is associated both with the fascia of the pectineus muscle and the pectineal ligament (Cooper liga ment). This ligament, described by Sir Astley Paston Cooper in 1804,48 is an extremely firm band of fibers on the cranial surface of the superior ramus of the pubic bone, which runs parallel to the pecten pubis and is undermined anteriorly by the pectineus muscle. The true nature of this fibrous band remains uncertain, which has led to numerous interpretations. The following important opinions may be mentioned:
• It is the lateral continuation of the lacunar falciform process (or lacunar ligament of Gimbernat).97
• It is a three-layered structure, with the superficial layer consisting of pectineal fascia, the middle layer of the pectineus, and the deep layer consisting of thickened periosteum.157
• It is a fusion of the periosteum with the transversalis fascia and the iliopubic tract.164
The author is convinced that the three layers of the pectineal ligament can be dissected without difficulty; so, this view should be preferred. Even though an understanding of the development of the pectineal ligament is currently lacking, it is nevertheless important to be aware of its topographical relations. According to Skandalakis, the following relations are important:
• The iliopubic tract inserts superiorly on the pectineal ligament.
• The tendon of pectineus arises inferiorly from the pectineal ligament.
• Medially, the pectineal ligament meets the lacunar falciform process.
The external iliac artery and vein emerge from the abdominal cavity into the vascular lacuna, where these become the femoral artery and vein, respectively. In the lacuna, the femoral vein is always medial and the femoral artery lateral. A gap remains between the falciform process and the femoral vein, which is closed by the soft and flexible femoral septum (of Cloquet, after Jules Germain Cloquet, 1790–1883, professor of anatomy and surgery in Paris). This septum is attached both to the free border of the falciform process and to the femoral vein.
The resistance of the femoral septum is considerably weakened as it is perforated like a sieve to allow passage of lymphatics. Because of these numerous lymphatics, the passage between the falciform process and femoral vein is also called the lymphatic lacuna. A large lymph node is regularly found on the outside of the femoral septum, known as Rosenmüller lymph node (after Johann Christian Rosenmüller, 1771–1820, professor of anatomy and surgery in Leipzig) or Cloquet lymph node. In many cases, this lymph node also extends through the femoral septum; so, the node is both external and internal.
Since the lymphatic lacuna is the weak site where femoral hernias emerge, it has become known in surgery as the femoral ring. The femoral ring is the internal femoral hernial orifice, while the external orifice is at the saphenous opening. Under normal anatomical conditions, a connecting “femoral canal” does not exist but only expands when a femoral hernia passes through it.
The Inguinofemoral Region
Although this region overlaps with the areas below the inguinal ligament described above, it is discussed separately as the surgically important junction with the lower extremity is located here.11,45,50,78,125,145,208,222 In applied anatomy, the region below the inguinal ligament is significant in two situations:
• Femoral hernia.
• Recurrent inguinal and femoral hernia ( Fig. 1.11).
Fig. 1.11).
The region has the following boundaries ( Fig. 1.12):
Fig. 1.12):
• The inguinal ligament superiorly.
• The pectineus muscle medially.
• Tensor fasciae latae laterally.
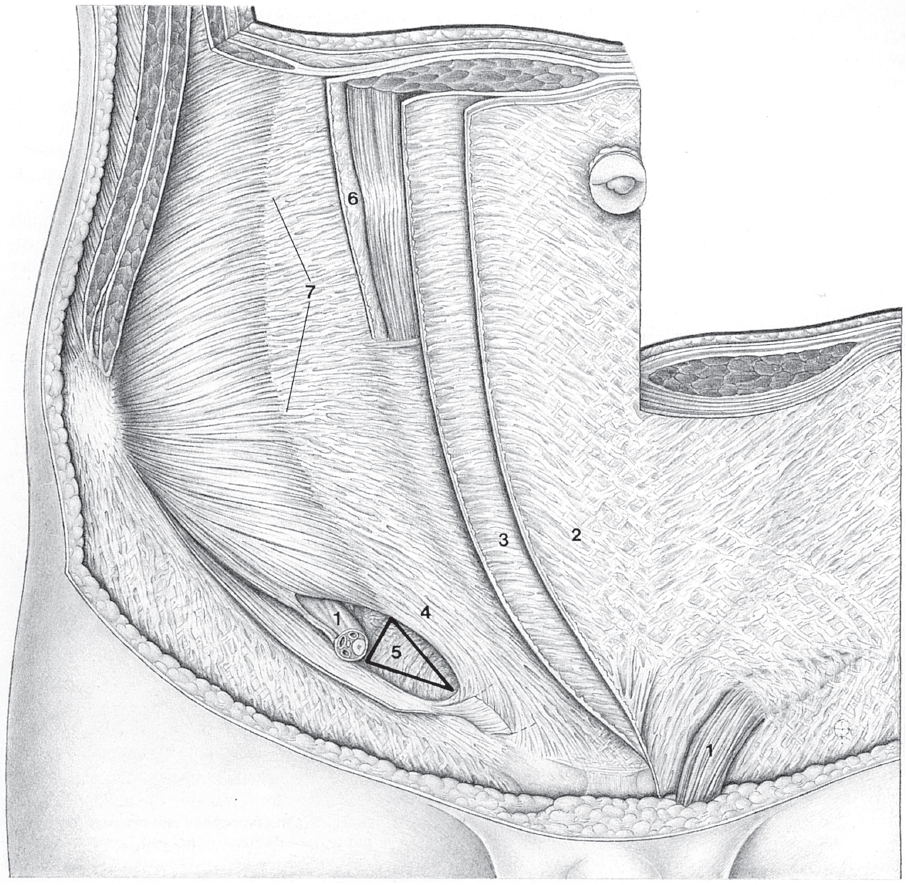
Fig. 1.9 Anatomy of the lower abdominal wall in the plane of the transversus abdominis showing the Hesselbach triangle.
1 Spermatic cord with cremaster muscle.
2 Rectus sheath, external oblique aponeurosis.
3 Rectus sheath, internal oblique aponeurosis.
4 Transversus border forming the upper boundary of the Hesselbach triangle.
5 Hesselbach triangle with transversalis fascia.
6 Rectus sheath, posterior layer of the internal oblique aponeurosis.
7 Linea semilunaris (Spieghel).
The femoral trigone (Scarpa triangle), a possible access route, is present in this region. It is limited:
• By the inguinal ligament superiorly.
• By adductor longus medially.
• By sartorius laterally.
The main superficial structures are the fibers of the fascia lata and the fossa ovalis with the saphenofemoral junction.

Caution
Varicosities of the great saphenous vein can be mistaken for a femoral hernia or can make surgery of a femoral hernia difficult.
The fossa ovalis contains the saphenofemoral junction, which is formed by the following superficial veins ( Fig. 1.12):
Fig. 1.12):
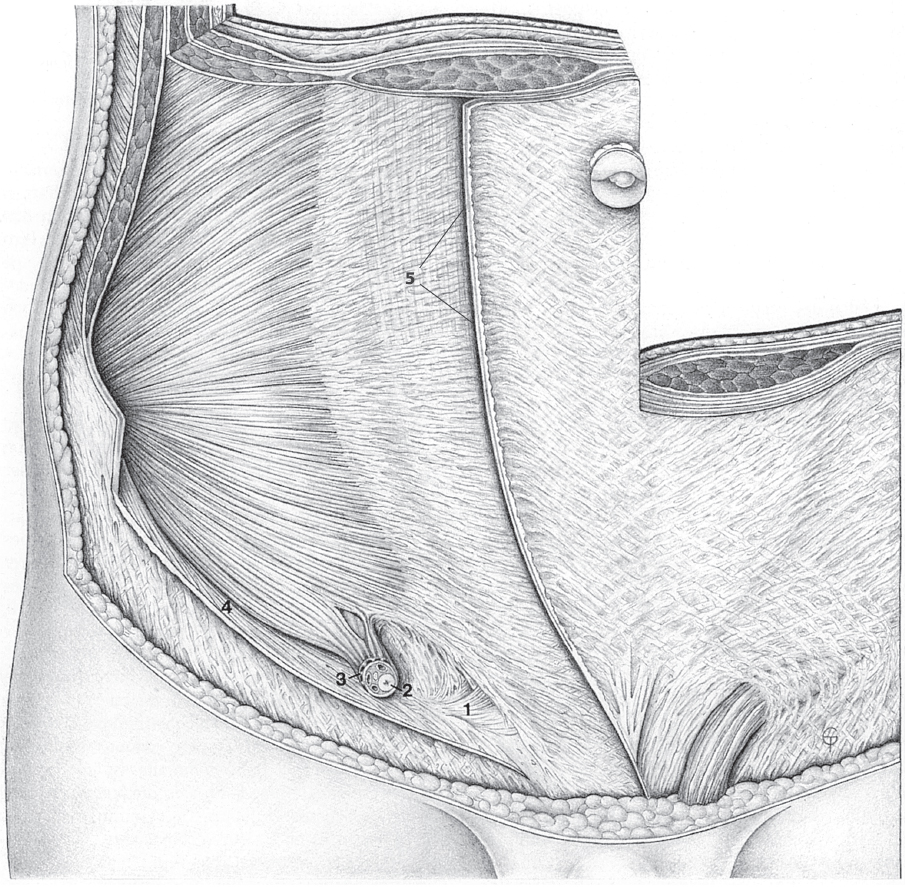
Fig. 1.10 Anatomy of the lower abdominal wall in the internal oblique plane.
1 Lacunar ligament.
2 Spermatic cord.
3 Cremaster muscle.
4 Inguinal ligament.
5 External oblique aponeurosis.
• Great saphenous vein with the saphenofemoral junction.
• External pudendal veins.
• Superficial epigastric vein.
• Superficial circumflex iliac vein.
These veins are very variable and can drain either into the great saphenous vein or else directly into the femoral vein.
A series of arteries, of variable caliber, arise in this region from the external iliac artery and its continuation, the femoral artery:
• The inferior epigastric artery arises from the external iliac artery just before it enters the vascular lacuna.
• The superficial epigastric artery arises from the femoral artery and passes superiorly in front of the inguinal ligament into the abdominal subcutaneous tissue.
• The deep circumflex iliac artery arises from the external iliac artery and runs upward parallel to the lateral part of the inguinal ligament. The vessel lies between the internal oblique and the transversus abdominis.
• The superficial circumflex iliac artery runs in lateral direction about 2 cm below and parallel to the inguinal ligament; its clinical significance is that it supplies the inguinal flap.
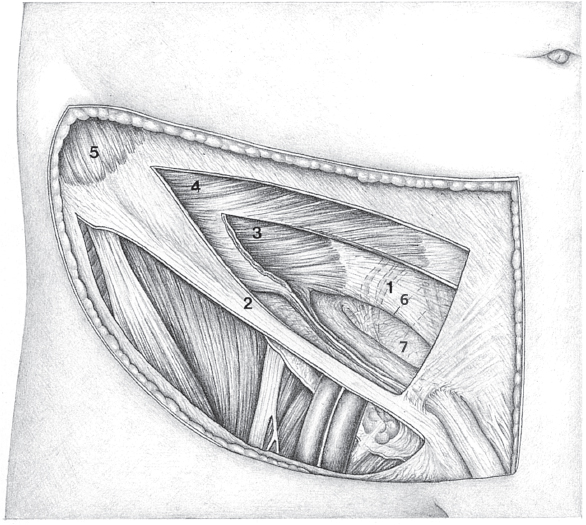
Fig. 1.11 Anatomic layers of the inguinofemoral region from front.
1 Epigastric vessels.
2 Inguinal ligament.
3 Transversus abdominis.
4 Internal oblique.
5 External oblique.
6 Transversus border, the “white line.”
7 Transversalis fascia.
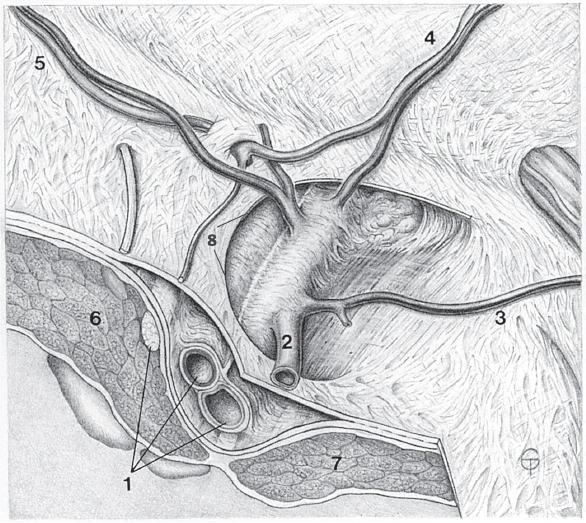
Fig. 1.12 Anatomy of the fossa ovalis.
1 Femoral vein, artery, and nerve (from medial).
2 Great saphenous vein.
3 External pudendal vein.
4 Superficial epigastric artery and vein.
5 Superficial circumflex iliac vein.
6 Iliopsoas muscle.
7 Pectineus.
8 Falciform margin with superior and inferior horns.
• The external pudendal arteries (usually two) pass medially to the scrotum and spermatic cord or to the labia.
In addition, there are two groups of lymphatics and lymph nodes in this region:
• The superficial lymph nodes are present beside the great saphenous vein.
• The deep lymph nodes are present beside the femoral vein so they are below the fascia lata. The Rosenmüller (or Cloquet) lymph node is a particularly large one located medial to the femoral vein on the femoral septum. It can also extend inward through the septum in an hourglass shape.
The femoral vessels and nerve and the iliopsoas muscle pass through the vascular or muscular lacuna below the inguinal ligament. The vascular lacuna is separated from the muscle lacuna by a thickened band of fascia, known as the iliopectineal arch. The femoral sheath starts here ( Fig. 1.12).
Fig. 1.12).
The anterior femoral sheath is the inferior continuation of the transversalis fascia onto the thigh; the iliac part of the iliopsoas fascia and the pectineal fascia constitute the posterior wall of the sheath. The femoral sheath ends inferiorly at the origin of the deep femoral artery and merges with the adventitia of the vessels. Septa within the sheath divide it into an arterial and a venous compartment. When a femoral hernia is present, it enters the vascular lacuna medial to the femoral vein and artery through the femoral ring ( Fig. 1.13).
Fig. 1.13).
The following topographical relations are important at the femoral ring:
• The anterior border is formed by the superficial part of the femoral sheath (derived from the transversalis fascia).
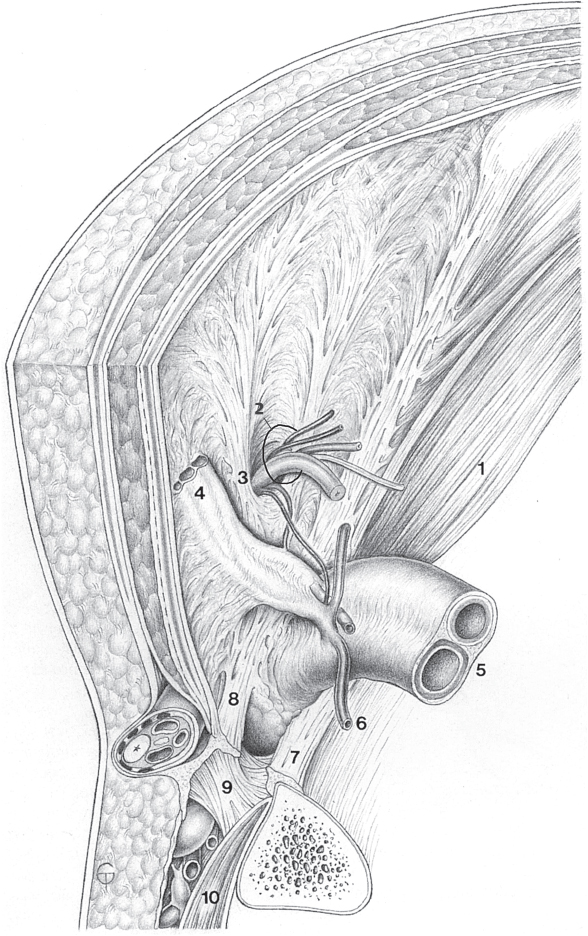
Fig. 1.13 Oblique anatomical cross-section through the inguinofemoral region.
1 Iliopsoas muscle.
2 Spermatic cord.
3 Henle loop.
4 Epigastric vessels.
5 Femoral artery and vein.
6 Pubic ramus.
7 Pectineal ligament.
8 Inguinal ligament.
9 Falciform process.
10 Pectineus muscle.
• The femoral vein and its adventitia form the lateral margin of the ring.
• The medial margin of the femoral ring consists of the border of the transversus abdominis insertion on the Cooper ligament.
• The inguinal ligament is more superficial than the transversalis fascia boundary of the femoral ring.
• The preperitoneal connective tissue (transversalis fascia) is attached to the adventitia of the femoral vein and constitutes the femoral septum, which lies in front of the femoral canal.
• The pectineal (Cooper) ligament on the superior ramus of the pubic bone consists of dense connective tissue fibers, the direction of which roughly follows that of the bone.
1.1.4 Laparoscopic Anatomy
The following four readily visible vertical lines provide orientation for laparoscopic hernia exploration:
• The linea alba.
• The lateral border of rectus abdominis crossed by the lateral umbilical fold.
• The vascular sheath of the epigastric vessels.
• The transversalis loop at the deep inguinal ring ( Fig. 1.7,
Fig. 1.7,  Fig. 1.14).
Fig. 1.14).
The lateral umbilical fold and the epigastric fold can be seen directly. The testicular vessels and vas deferens are often less visible behind the intact peritoneum.
The genitofemoral nerve and the testicular vessels lie beneath the parietal peritoneum. The genital branch of the genitofemoral nerve and the vas deferens enter the spermatic cord in the vicinity of the deep inguinal ring. The pubic branch, a communication between the epigastric vessels and the obturator vessels, is found on the medial part of the pectineal ligament. It crosses the periosteum on the inside of the superior pubic ramus, where it is at extreme risk of injury (the “corona mortis”). In 22% of cases, the obturator artery arises from the inferior epigastric artery129 and passes into the obturator canal over the back of the superior pubic ramus.
The lateral cutaneous femoral nerve with one or two sensory branches and the femoral branch of the genitofemoral nerve are located in the fat between the iliopsoas muscle and the parietal peritoneum. The ilioinguinal nerve enters the abdominal muscle lateral to this and the femoral nerve is medial to it, lying between iliacus and psoas major and protected only by the iliopsoas fascia. The nerve thus lies deep in the center of the operation region ( Fig. 1.14). In general, when sutures or staples are used to fix mesh laparoscopically, vessels and nerves are safe only when the fixation is above the iliopubic tract.
Fig. 1.14). In general, when sutures or staples are used to fix mesh laparoscopically, vessels and nerves are safe only when the fixation is above the iliopubic tract.
Lateral branches of the lateral cutaneous femoral nerve are an exception, as they can also run above the iliopubic tract. Below the iliopubic tract, the iliopectineal ligament is the only suitable fixation site provided there are no vascular connections to the obturator vessels and small side branches. Blind fixation without prior dissection must be avoided.
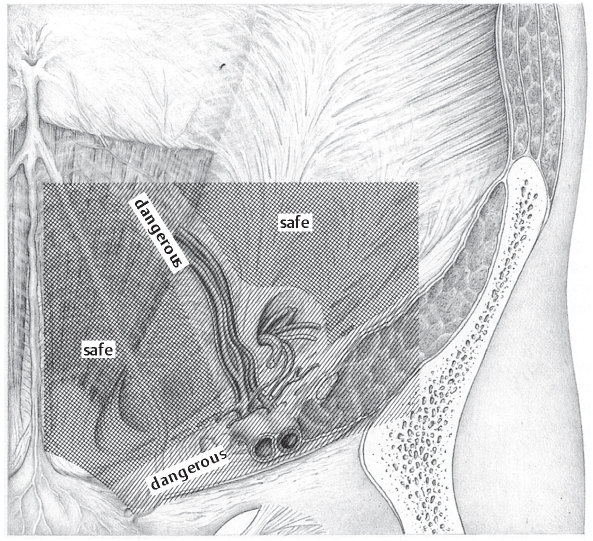
Fig. 1.14 Laparoscopic anatomy of the inguinofemoral region showing the safe areas (cross-hatched) for sutured or stapled mesh fixation.
1.2 Definition and Terminology
1.2.1 Hernia

Definition
The term hernia is derived from the Greek word ἓ ρνoζ meaning a young shoot. It denotes the protrusion of the parietal peritoneum through a preformed or secondary gap. An external hernia passes through the abdominal wall to become visible on the surface of the body, while an internal hernia results from protrusion into a peritoneal pocket. Interparietal hernias of the abdominal wall occupy an intermediate position. Intra- and retroperitoneal organs can be displaced constantly or intermittently with the hernia. Complete and incomplete (partial or Richter) hernias are distinguished, depending on the content of the sac ( Fig. 1.15).10,44,119,121,162,236,245
Fig. 1.15).10,44,119,121,162,236,245
Complete hernias are distinguished from sliding hernias depending on the completeness of the peritoneal covering. Sliding hernias contain retroperitoneal viscera (e.g., ascending or descending colon, bladder, cecum) and therefore the hernial sac is not completely covered by peritoneum. Thus, parts of retroperitoneal organs (e.g., bladder, cecum) sometimes form the wall of the hernial sac. These are easily injured if the actual anatomy is not recognized.205
As regards the time of origin, congenital hernias (e.g., umbilical hernia, indirect inguinal hernia due to patent processus vaginalis) are distinguished from acquired forms (e.g., direct inguinal hernia, femoral hernia).158 A further differentiation is between primary (pre-existing orifices) and secondary (orifices developing later).
1.2.2 Structure of a Hernia
The most important components of a hernia surgically are:77,121
• The hernial orifice.
• The hernial sac.
• The hernial contents.
• The hernial coverings.
![]() Hernial orifice. This is formed by the layers of the abdominal wall, i.e., muscle, tendon, aponeurosis, and scar tissue. In the pelvis, periosteum and bone can also be involved in the formation of hernial orifice (e.g., obturator hernia). The name of the hernia comes from the location of its orifice (e.g., inguinal, femoral, lumbar, or incisional hernia).
Hernial orifice. This is formed by the layers of the abdominal wall, i.e., muscle, tendon, aponeurosis, and scar tissue. In the pelvis, periosteum and bone can also be involved in the formation of hernial orifice (e.g., obturator hernia). The name of the hernia comes from the location of its orifice (e.g., inguinal, femoral, lumbar, or incisional hernia).
![]() Hernial sac. This is a pouch of varying size that contains the hernia. It is divided topographically into the neck, body, and fundus and is usually lined with reflected peritoneum. With inflammation or necrosis, the sac can adhere to the hernia contents so the contents are fixed within the sac.
Hernial sac. This is a pouch of varying size that contains the hernia. It is divided topographically into the neck, body, and fundus and is usually lined with reflected peritoneum. With inflammation or necrosis, the sac can adhere to the hernia contents so the contents are fixed within the sac.
![]() Hernial contents. This can comprise any of the abdominal contents, though the omentum and small bowel are most often involved. A giant hernia can contain large amounts of abdominal contents such that its reduction can be difficult due to lack of space within the abdomen. The hernial contents are normally bathed in a transudate and therefore can slide freely, but this can be lost during inflammation, incarceration, or necrosis when blood, bowel content, or pus can lead to adhesions or abscesses.
Hernial contents. This can comprise any of the abdominal contents, though the omentum and small bowel are most often involved. A giant hernia can contain large amounts of abdominal contents such that its reduction can be difficult due to lack of space within the abdomen. The hernial contents are normally bathed in a transudate and therefore can slide freely, but this can be lost during inflammation, incarceration, or necrosis when blood, bowel content, or pus can lead to adhesions or abscesses.
![]() Hernial coverings. These are the layers of tissue surrounding the hernial sac. Depending on hernia size, duration, and location, they can consist of either two layers (e.g., umbilical hernia, incisional hernia) or multiple layers (e.g., inguinal hernia). The number of layers is determined by the anatomical relations and the mechanism of development. For instance, an inguinal hernia has a five-layered structure consisting of peritoneum, preperitoneal fat, transversalis or cremasteric fascia, superficial abdominal fascia, and subcutaneous tissue and epidermis (see section
Hernial coverings. These are the layers of tissue surrounding the hernial sac. Depending on hernia size, duration, and location, they can consist of either two layers (e.g., umbilical hernia, incisional hernia) or multiple layers (e.g., inguinal hernia). The number of layers is determined by the anatomical relations and the mechanism of development. For instance, an inguinal hernia has a five-layered structure consisting of peritoneum, preperitoneal fat, transversalis or cremasteric fascia, superficial abdominal fascia, and subcutaneous tissue and epidermis (see section  1.1).
1.1).
1.2.3 Hernia Disease
The pathological significance of a hernia depends on how it affects the patient physically and psychologically after it is diagnosed. This ranges from subjective awareness of the hernia with consequent life-long avoidance of exertion on account of a “weak groin” to concealment of sometimes gigantic scrotal hernias. Objectively, hernias can have a direct effect, for instance, due to disability and ulceration with giant hernias, impairment of joint mobility, recurrent omental incarceration in small hernias, and for cosmetic reasons.
Hernia disease is more often caused by changes in the hernial contents. These may include:
• Interference with the blood supply of the bowel and omentum (incarceration, strangulation).
• Interference with intestinal passage (complete or incomplete obstruction).
• Complications of these disturbances.
Hernias are classified as reducible, irreducible, and incarcerated.
![]() Reducible hernia. A hernia in which the contents are freely mobile in the hernial sac and ring is termed reducible hernia. The hernia contents can return to the abdomen spontaneously or by manual reduction (taxis).
Reducible hernia. A hernia in which the contents are freely mobile in the hernial sac and ring is termed reducible hernia. The hernia contents can return to the abdomen spontaneously or by manual reduction (taxis).
![]() Irreducible hernia. A hernia is irreducible when the contents are fixed in the hernial sac and ring. Hernias are irreducible when incarcerated (see below), when there are adhesions between the sac and its contents, or when the hernia is so large that the contents no longer fit back in the abdomen. A non-incarcerated irreducible hernia is usually present for many years, causes little or no pain, and generally has not been reduced for a long time.
Irreducible hernia. A hernia is irreducible when the contents are fixed in the hernial sac and ring. Hernias are irreducible when incarcerated (see below), when there are adhesions between the sac and its contents, or when the hernia is so large that the contents no longer fit back in the abdomen. A non-incarcerated irreducible hernia is usually present for many years, causes little or no pain, and generally has not been reduced for a long time.