Chapter 2
Adult Inguinal Hernia
2.1Indications and Choice of Procedure
2 Adult Inguinal Hernia
2.1 Indications and Choice of Procedure
As in the past, discussion continues to focus on the choice of inguinal hernia repair procedure, but the indications themselves are now the topic about which opinions vary widely.
2.1.1 Indications
Only a few years ago, the finding of an inguinal hernia was an undisputed indication for surgery. The main argument was the risk of incarceration, which was estimated at 10% in the natural course of the condition. This was not confirmed by any studies, however, and has not been borne out by more recent studies, which reported the incidence of incarceration as less than 1% with a watch-and-wait approach. In addition, it was apparent that, apart from incarceration, the potential risk of an inguinal hernia in terms of morbidity and mortality is extremely low. The admonishments of surgeons in the past to operate early are thus no longer justified.
When an inguinal hernia is diagnosed, the surgeon can suggest the patient to undergo surgery at a time that suits him if and when the hernia bothers him. This decision should be guided by his personal situation and without any compulsion. The timing should be sooner for patients with greater risk, general physical weakness, and troublesome comorbidities than for physically fit and athletic patients. This applies especially to patients with risk features such as iatrogenic or spontaneous blood clotting disorders, immune suppression, or other hazardous comorbidities. Patients with cardiovascular risk factors, diabetes, renal impairment, or previous abdominal surgery should undergo surgery when optimal preparation is possible; that is, they should have early elective surgery. It does not make sense to operate on these patients only when complications occur. This rule has not changed in the more recent era of watch-and-wait studies, where an early elective procedure continues to be the best approach. The same applies for giant hernias, recurrences, and inguinal hernias with detectable skin damage. Emergency surgery in these situations may be life-threatening and should therefore be avoided wherever possible by a well-timed elective procedure. Furthermore, operation is indicated when the patient desires it because the hernia is physically annoying or interferes with sporting activities, and also when the patient is concerned about it aesthetically. Even if the risk of incarceration is low, the body-conscious patient can be extremely bothered by the hernia swelling with the need for manual reduction after physical effort and his wish provides sufficient indication.
![]() Absolute indications
Absolute indications
• Incarcerated, nonreducible hernia.
• Incarcerated hernia with peritonitis or suspected bowel necrosis.
• Recurrent incarceration.
![]() Relative indication
Relative indication
• Impaired general operability in elderly or severely ill patients.
![]() Contraindications
Contraindications
• Incurable intra-abdominal conditions (e.g., peritoneal carcinomatosis).
• General and local inoperability (maximum 1% of all inguinal hernias).
![]() Preparation
Preparation
• Bowel cleansing by enema or laxatives the night before surgery.
• Shaving or chemical depilation of the operation area on the day of surgery.
• Topical disinfection of the operation area with conventional skin disinfectants.
• Transurethral catheter if necessary (e.g., in the case of prostatic hyperplasia).
• Medications can be given safely during inguinal hernia surgery, with the exception of anticoagulant drugs. Patients on warfarin should be switched to heparin. Patients on aspirin can be operated on safely at a dose of 100 mg per day but at higher doses this should be discontinued at least a week before the operation and these patients may need to be switched to heparin.
![]() Position
Position
• Supine position with the hips extended, and the head lowered if necessary.
![]() Anesthesia
Anesthesia
• Local anesthesia: optional depending on hospital practice, advantageous especially for anterior sutured and patch and plug procedures and in elderly patients with cardiopulmonary disorders having outpatient surgery.
• Regional anesthesia: optional depending on hospital practice, advantageous especially for posterior mesh procedures without opening of the abdominal cavity.
• General anesthesia: optional depending on hospital practice, obligatory especially for laparoscopic techniques and complicated recurrent hernias.
Choice of Procedure
This is currently the most controversial issue, with surgeons divided into different groups. Inguinal hernia repair procedures can be classified systematically into anterior and posterior approaches and into sutured and mesh procedures. The anterior sutured repairs include the Bassini, Zimmerman, Lotheissen/McVay, and Shouldice methods, and the anterior mesh techniques include the mesh and plug techniques of Lichtenstein, Kugel, Rutkow, and others, such as the transinguinal preperitoneal technique (TIPP). The posterior approaches include the Nyhus technique with and without mesh, the Wantz, Stoppa, and Ugahary methods, and the laparoscopic totally extraperitoneal mesh repair (TEP), transabdominal preperitoneal mesh repair (TAPP), and intraperitoneal onlay mesh (IPOM). The decision is often made by the book and is more a matter of belief than factually grounded. This explains the regional, national, and international differences.
2.2 Open Suture Techniques
2.2.1 Approach and Dissection
Indication
![]() Relative. Proven inguinal hernia. Timing: soon after diagnosis and as an emergency if incarceration is present.
Relative. Proven inguinal hernia. Timing: soon after diagnosis and as an emergency if incarceration is present.
![]() Contraindications. None apart from absolute general inoperability or absence of consent.
Contraindications. None apart from absolute general inoperability or absence of consent.
![]() Alternative procedures. Many, see below.
Alternative procedures. Many, see below.
Operation Preparation
![]() Preoperative diagnostics.
Preoperative diagnostics.
• Ultrasonography.
• Doppler ultrasound of testis before surgery of recurrence.
Special Risks, Informed Consent
• Spermatic cord injury (1%).
• Wound infection (2%).
• Chronic groin pain (< 5%).
• Recurrence (1–10%).
• Mortality (< 0.2%).
Anesthesia
Local anesthesia is preferable in cooperative patients; otherwise, spinal/epidural anesthesia or general anesthesia is used.
Position
Supine.
Access
Transverse or slightly oblique incision above the inguinal crease.
Relevant Anatomy, Dangers, and Tricks
• The transversalis fascia is the crucial plane for successful surgery so exposure and reconstruction must be anatomically exact.
• In routine cases, repair with reconstruction of the anatomy continues to be preferable to repair with introduction of alloplastic material.
Management of Special Complications
• Vascular injury: suture under vision (5/0 to 7/0 polypropylene).
• Vas deferens injury: direct suture (7/0 PDS).
Postoperative Management
![]() Medical care. If a drain is placed then it is removed on day 2. Male patients should wear close fitting underpants in the first few days. The patient should be provided with an information leaflet on gradual resumption of physical effort and sports activities.
Medical care. If a drain is placed then it is removed on day 2. Male patients should wear close fitting underpants in the first few days. The patient should be provided with an information leaflet on gradual resumption of physical effort and sports activities.
![]() Diet. Immediately.
Diet. Immediately.
![]() Bowels. Enema if necessary.
Bowels. Enema if necessary.
![]() Mobilization. Immediately.
Mobilization. Immediately.
![]() Physical therapy. None required.
Physical therapy. None required.
![]() Incapacity for work. One to two weeks.
Incapacity for work. One to two weeks.
Operation Techniques
Access
See  Fig. 2.1
Fig. 2.1
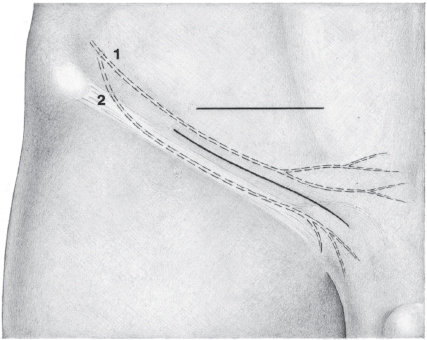
Fig. 2.1 Access is through a transverse skin incision in the lower groin crease; an oblique inguinal incision is an alternative. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.) 1 Iliohypogastric nerve. 2 Ilioinguinal nerve.
Splitting the External Oblique Aponeurosis I
See  Fig. 2.2.
Fig. 2.2.
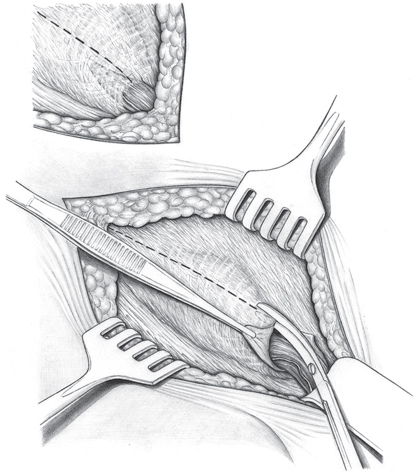
Fig. 2.2 After opening the subcutaneous tissue, the external oblique aponeurosis with the superficial inguinal ring is exposed. It is split superiorly, starting at the superficial ring. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.)
Splitting the External Oblique Aponeurosis II
See  Fig. 2.3.
Fig. 2.3.
Protecting the Nerves
See  Fig. 2.4.
Fig. 2.4.
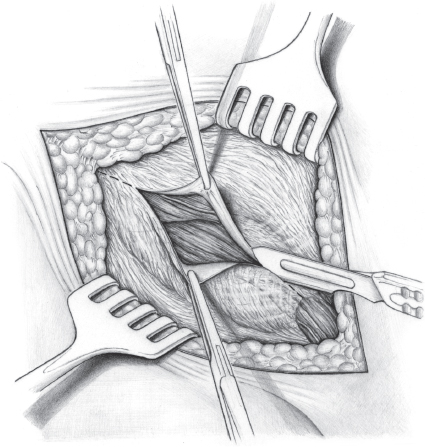
Fig. 2.3 If the superficial ring is difficult to identify, the external oblique aponeurosis can be divided with a scalpel in cranial to caudal direction toward the superficial ring. The fascial edges are grasped with sharp clamps to draw them apart. The external oblique aponeurosis must be opened fully, including the superficial inguinal ring. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.)
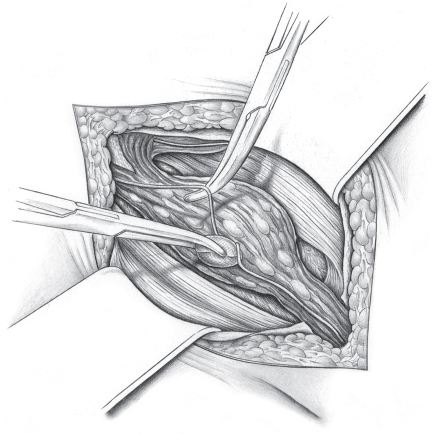
Fig. 2.4 After opening the inguinal canal, the internal oblique and cremaster muscles are exposed. The ilioinguinal nerve, which usually runs on the internal oblique, is identified, dissected bluntly, and moved under the cranial retractor. The genital branch of the genitofemoral nerve is rarely visible immediately, as shown here; it is usually more posterior and only becomes visible after the cremaster is divided. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.)
Splitting the Cremaster
See  Fig. 2.5.
Fig. 2.5.
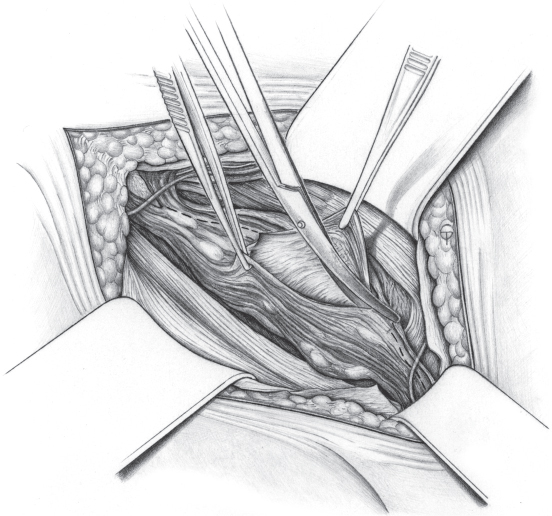
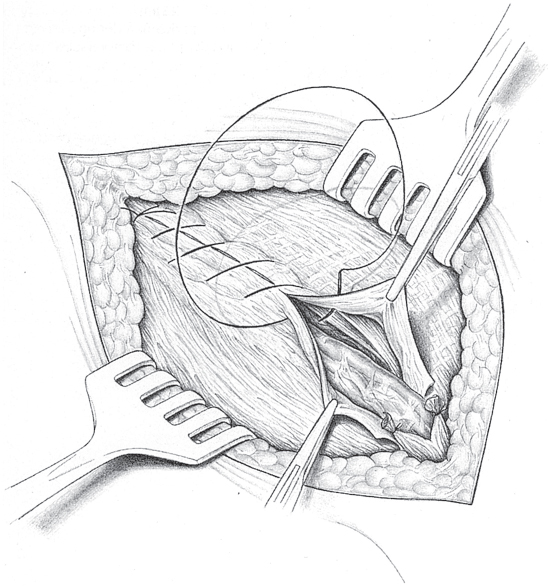
Fig. 2.5 The cremaster muscle is split with scissors, using 3 Roux hooks to expose the operation field. It is split down to the shiny internal cremasteric fascia, which can be separated easily from the spermatic cord beneath it. Injury to the spermatic cord structures is avoided by blunt dissection. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.)
Dissection of the Cremaster Muscle
See  Fig. 2.6.
Fig. 2.6.
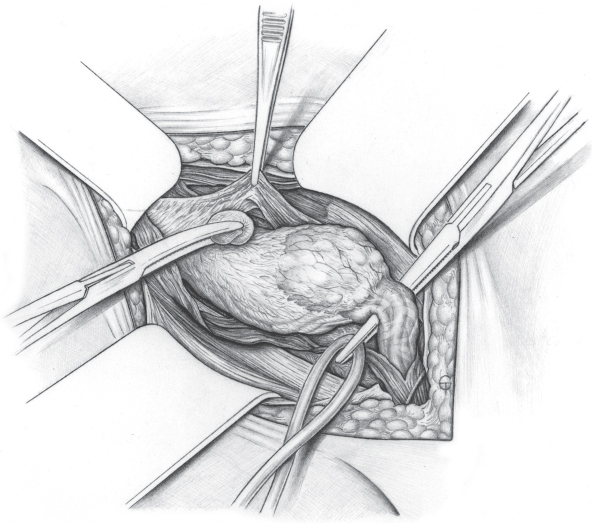
Fig. 2.6 The spermatic cord is dissected from the cremaster by a combination of blunt and sharp dissection. The genital branch of the genitofemoral nerve in the posterior part must be protected carefully and preserved. It often runs jointly with the external cremasteric vessels in the deep inguinal ring. The spermatic cord is snared with a loop and the two parts of the cremaster are pushed away bluntly in cranial and caudal direction. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.)
Resection of the Cremaster Muscle
See  Fig. 2.7.
Fig. 2.7.
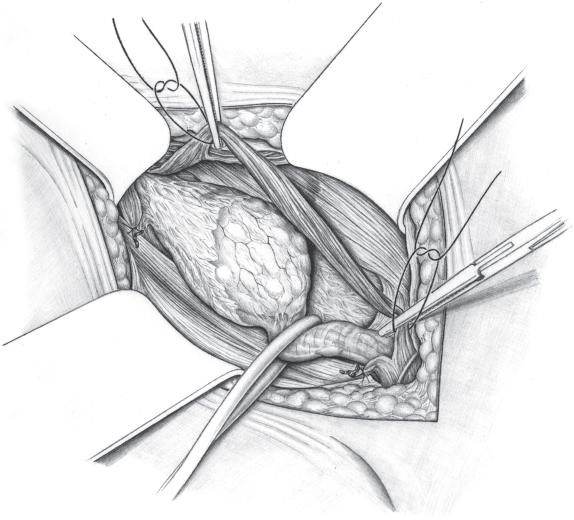
Fig. 2.7 The cremaster muscle can be divided between clamps and resected, and the stumps can be ligated. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.)
Dissection of the Hernial Sac
See  Fig. 2.8.
Fig. 2.8.
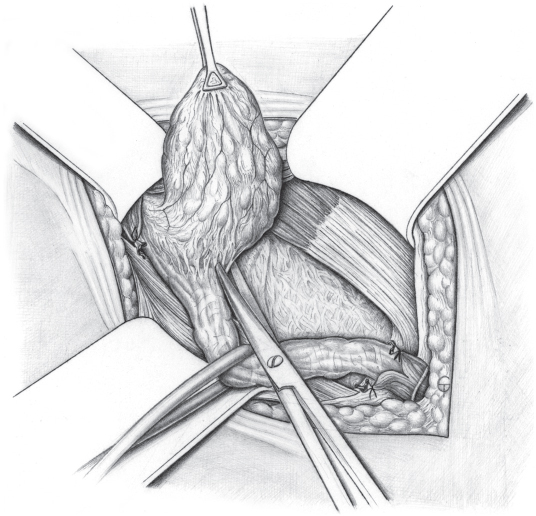
Fig. 2.8 By pulling gently on the rubber snare around the spermatic cord and, if necessary, grasping the sac with Duval forceps, the sac can be detached gradually from the spermatic cord and transversalis fascia by blunt and sharp dissection. If it is highly adherent and its course is unclear, it can sometimes be helpful to open the sac at this stage of the dissection to expose the structures more clearly. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.)
Dissection of the Neck of the Sac
See  Fig. 2.9.
Fig. 2.9.
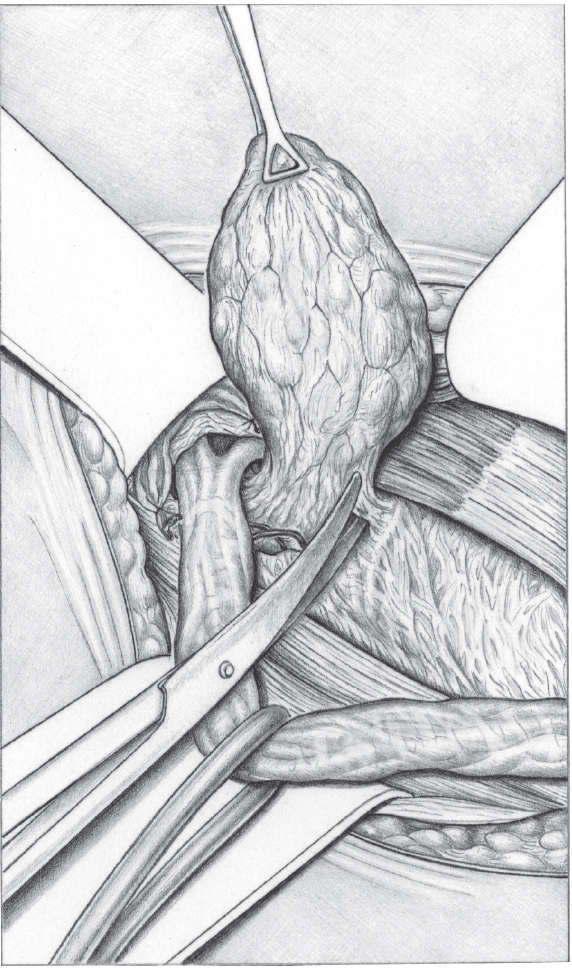
Fig. 2.9 Dissection of the sac must extend to the gap in the transversalis fascia. If this is at the deep inguinal ring, in the case of an indirect hernia, the deep ring must be exposed completely. The spermatic cord must be dissected at the deep ring to expose the bifurcation of the vas deferens and spermatic vessels clearly. The hernial sac must be dissected on all sides at the deep ring and detached from all adhesions to the transversalis fascia. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.)
Management of the Hernial Sac
See  Fig. 2.10.
Fig. 2.10.
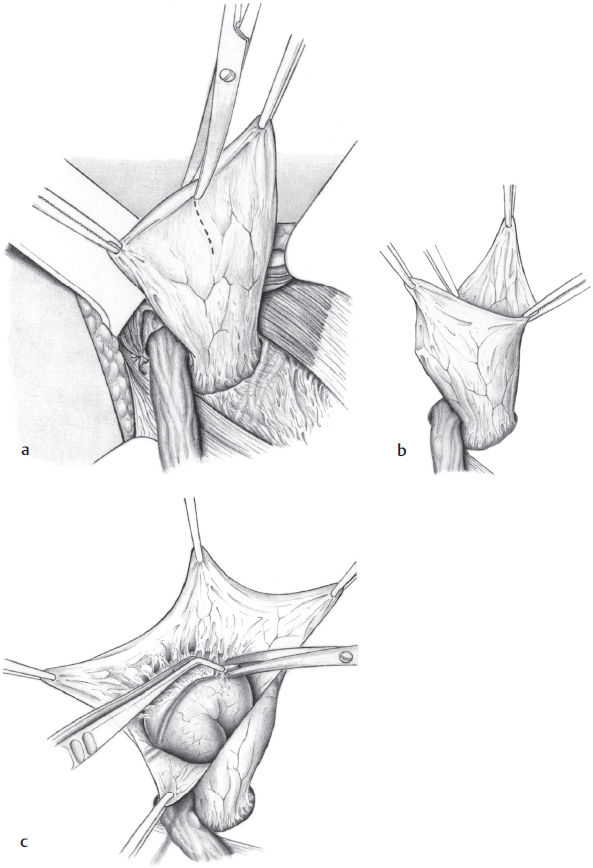
Fig. 2.10 If the sac contents cannot be reduced or intra-abdominal involvement (incarceration, metastases, etc.) is suspected, the sac must be opened. It is grasped between forceps, opened longitudinally, and stretched between four clamps (a and b). Adherent bowel can be dissected with scissors if it is not fixed too extensively (c). Otherwise, the bowel should not be detached widely but the sac should be closed and buried with a purse string suture. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.)
Division of the External Cremasteric Vessels
See  Fig. 2.11.
Fig. 2.11.
Direct Hernial Sac Dissection
See  Fig. 2.12.
Fig. 2.12.
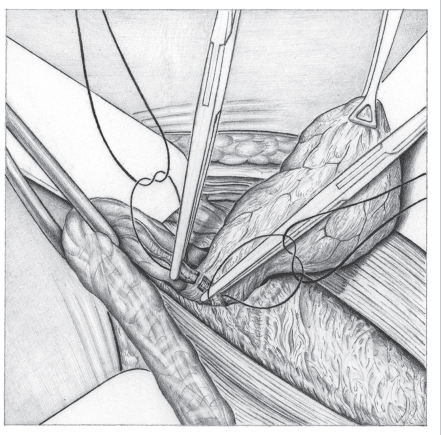
Fig. 2.11 The external cremasteric vessels, which arise from the inferior epigastric vessels, should be divided and ligated with a transfixion suture. The genital branch of the genitofemoral nerve regularly runs in this area and should be preserved where possible. It is not essential to divide the external cremasteric vessels but this provides clearer exposure at the deep ring. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.)
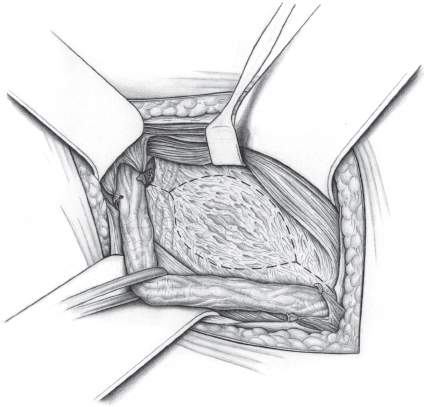
Fig. 2.12 With direct inguinal hernias, an incision is made in the transversalis fascia around the sac leaving superior and inferior fascial margins that can be sutured. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.)
Management of the Hernial Sac I
See  Fig. 2.13.
Fig. 2.13.
Management of the Hernial Sac II
See  Fig. 2.14.
Fig. 2.14.
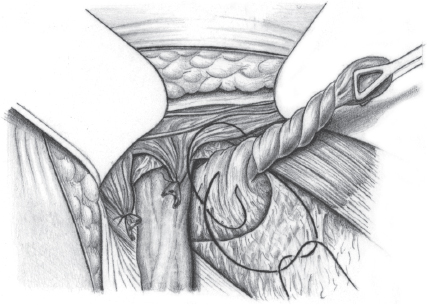
Fig. 2.13 The sac is managed in different ways. At the deep ring, it can be twisted, transfixed, and ligated. The protruding end is excised. This is the simplest and at the same time the most common method. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.)

Fig. 2.14 Direct inguinal hernial sacs, sacs containing adherent bowel that cannot be mobilized, and sliding hernias are buried with a purse string suture. The purse string suture must be placed without injuring any internal structures. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.)
Management of the Hernial Sac III
See  Fig. 2.15.
Fig. 2.15.
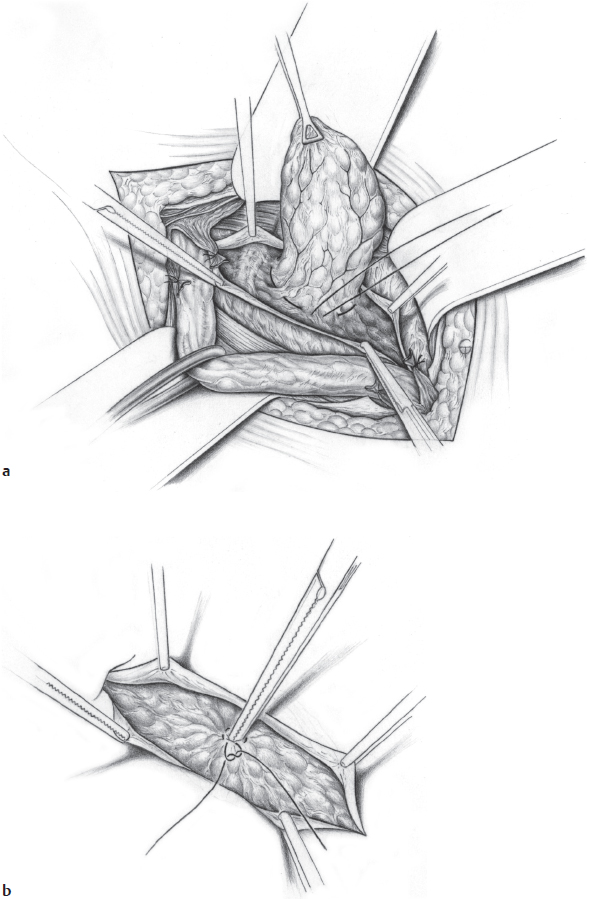
Fig. 2.15 Opening the sac of a direct hernia can usually be omitted. A purse string suture is placed and tightened after reducing the sac contents, and the sac is buried behind the fascia. When this method is used, it is important to split the transversalis fascia fully beforehand and hold it apart with clamps (a). This is the only way to ensure that the sac is buried without involving the transversalis fascia, which is later so important for the repair (b). (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.)
Removal of a Preperitoneal Lipoma
See  Fig. 2.16.
Fig. 2.16.
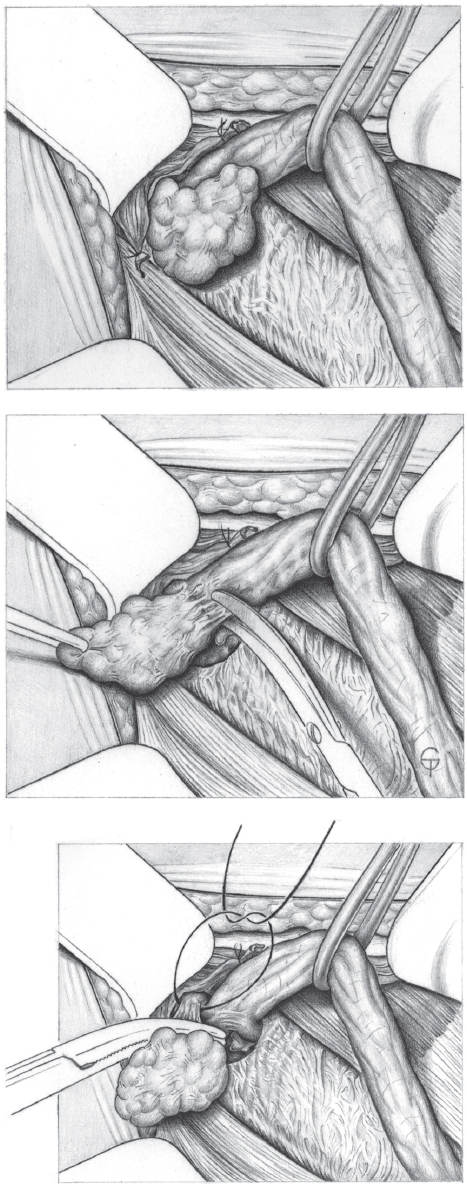
Fig. 2.16 After (and sometimes before) dealing with the hernial sac, the preperitoneal lipoma must be dissected sharply from the spermatic cord. It is then transfixed at its base, ligated, and excised. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.97)
Inspection of the Transversalis Fascia
See  Fig. 2.17.
Fig. 2.17.
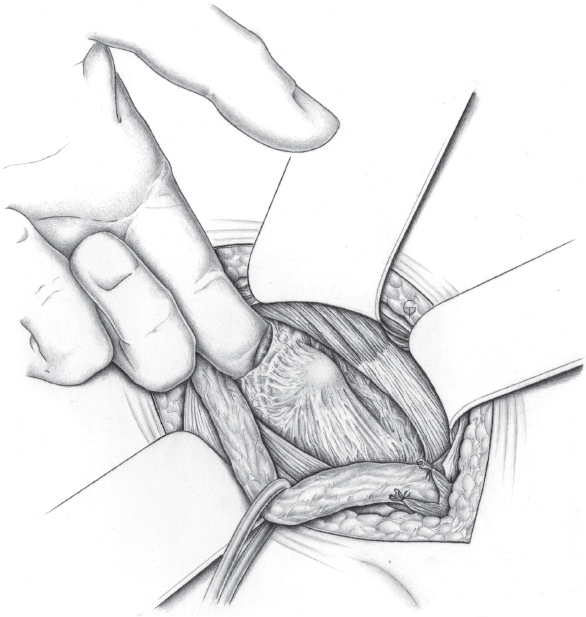
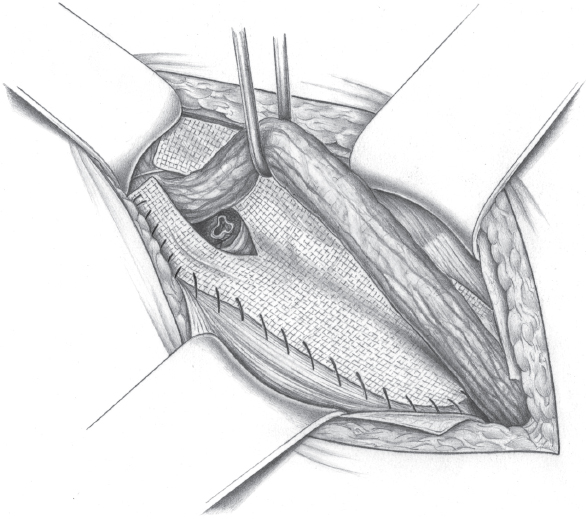
Fig. 2.17 After exposure of the posterior wall of the inguinal canal, the strength of the transversalis fascia is tested by inserting the index finger into the deep ring. If the fascia can be moved easily and is not highly resistant, complete posterior repair must be performed. The hernia type is then classified, distinguishing between lateral (L) = indirect and medial (M) = direct hernias, size I (< 1.5 cm), II (< 3 cm) and III (> 3 cm). LI and MI hernias can be sutured directly, LII and MII hernias can be repaired by complete fascial doubling, and larger hernias may be repaired with a polypropylene mesh. The most important methods, which are used for 85% of all inguinal hernias, will be shown. Small indirect hernias can be repaired by the Zimmerman method of isolated reconstruction of the deep ring. However, complete division of the transversalis fascia and repair by doubling it (the Shouldice method) is usually the procedure of choice. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.)
2.2.2 Hernia Repair
Bassini Repair
Indication
The Bassini repair is rarely indicated routinely nowadays. We have not performed this operation for many years as it has been replaced by the Shouldice repair. It should nevertheless be in every surgeon’s potential repertoire.
After excising the hernial sac, the posterior wall of the inguinal canal is exposed and the spermatic cord is snared and retracted laterally. The wall is palpated with a finger to detect any instability or defect.
Operation Techniques
Repair Principle
See  Fig. 2.18.
Fig. 2.18.
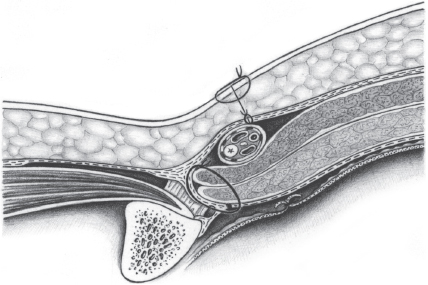
Fig. 2.18 The Bassini inguinal hernia repair consists of attachment of the three-layer abdominal wall to the inguinal ligament by a single row of interrupted sutures through the three layers. The spermatic cord is positioned in front of the muscle and behind the external oblique aponeurosis. (From Hollinshead WH. The abdominal wall and inguinal region. In: Anatomy for Surgeons: The Thorax, Abdomen and Pelvis. Vol. 2. New York, NY: Hoeber; 1956.)
Incision of the Transversalis Fascia
Although omission of this step is often advocated, splitting the transversalis fascia is an essential part of the Bassini repair. This is the only way to obtain the three layers for suturing. The fascia is split from the deep inguinal ring to the pubic tubercle ( Fig. 2.19). This includes the orifice of a medial hernia. As in the fascial splitting that forms part of the Shouldice repair, the epigastric vessels should be carefully preserved.
Fig. 2.19). This includes the orifice of a medial hernia. As in the fascial splitting that forms part of the Shouldice repair, the epigastric vessels should be carefully preserved.
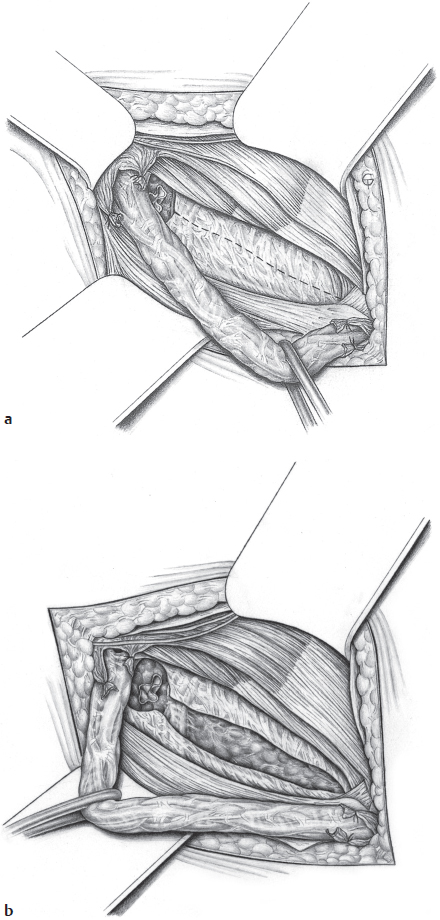
Fig. 2.19 a and b
a Direction and extent of the splitting of the transversalis fascia.
b Three layers of the abdominal wall after splitting the transversalis fascia on the posterior wall of the inguinal canal.
Splitting the transversalis fascia opens the hernial orifice. This exposes the tissue layers that will later be sutured: the transversalis fascia, the transversus abdominis and internal oblique muscles, and the inguinal ligament ( Fig. 2.19).
Fig. 2.19).
First Three-Layer Medial Bassini Suture
Closure of the hernial opening starts at the medial angle of the groin. Nonabsorbable (2/0 polypropylene) or slowly absorbable (2/0 PDS) suture material is used. The first suture passes through the junction of the internal oblique with the edge of the transversus abdominis (conjoint tendon or inguinal falx). This is followed by the two margins of the transversalis fascia and finally the reflected ligament and pubic periosteum. This is the actual Bassini suture ( Fig. 2.20). It is important that the stitch through the periosteum does not injure the bone (causing subsequent pain).
Fig. 2.20). It is important that the stitch through the periosteum does not injure the bone (causing subsequent pain).
Complete Row of Bassini Sutures Prior to Tying
Interrupted sutures are now placed at intervals of 0.6 cm as far as the deep inguinal ring, which catch the inferior border of the inguinal ligament tangentially instead of the periosteum. These can also be placed as U-sutures but must have wide bridges so as not to interfere with tissue perfusion. These are held with clamps ( Fig. 2.21). If the cremaster was not resected, it can be included to reinforce the posterior wall.18
Fig. 2.21). If the cremaster was not resected, it can be included to reinforce the posterior wall.18
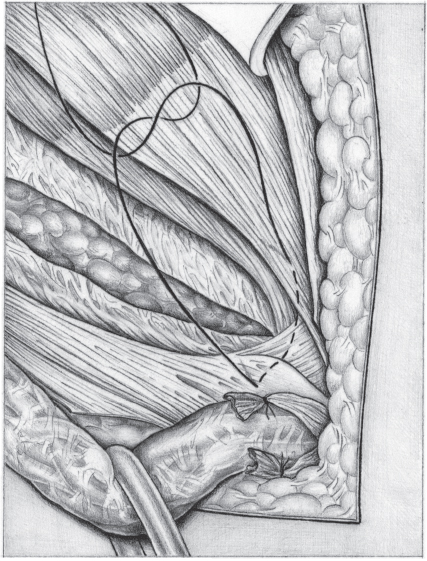
Fig. 2.20 Placement of the first suture, the actual Bassini suture, at the medial end of the wound, picking up the pubic periosteum.
Tying the Bassini Sutures
The Bassini sutures are tied individually to approximate the tissue, starting at the medial end. The newly constituted deep ring must admit the tip of the little finger or forceps to ensure that the spermatic cord has enough room. If the deep ring remains too large due to a high position of the internal oblique, a suture anterior to the spermatic cord can fix the internal oblique to the inguinal ligament ( Fig. 2.22). If the sutures are tense, a relieving incision in the rectus sheath may be indicated.
Fig. 2.22). If the sutures are tense, a relieving incision in the rectus sheath may be indicated.
Closure of the External Oblique Aponeurosis
The anterior wall of the inguinal canal is reconstructed by closing the external oblique aponeurosis with interrupted sutures of the same material (2/0 polypropylene or PDS;  Fig. 2.23). This allows a new superficial ring to be constructed, which should be reduced in size and located as far medially as possible.
Fig. 2.23). This allows a new superficial ring to be constructed, which should be reduced in size and located as far medially as possible.
Girard Variation
This suture can also be placed so that the aponeurosis forms a double layer, in the Girard or Halsted/Ferguson method ( Fig. 2.24).
Fig. 2.24).
Kirschner Variation
The Kirschner method is a modification of the Bassini procedure.49 In this, the split external oblique aponeurosis is sutured beneath the spermatic cord, making it subcutaneous in position ( Fig. 2.25). This should theoretically produce additional reinforcement of the posterior wall of the inguinal canal. In fact, however, moving the spermatic cord to a subcutaneous position abolishes the offset closure of the inguinal canal, which degenerates into a direct “hernial hole” due to superimposition of the deep and superficial rings, with an extremely high risk of recurrence.
Fig. 2.25). This should theoretically produce additional reinforcement of the posterior wall of the inguinal canal. In fact, however, moving the spermatic cord to a subcutaneous position abolishes the offset closure of the inguinal canal, which degenerates into a direct “hernial hole” due to superimposition of the deep and superficial rings, with an extremely high risk of recurrence.
The Hackenbruch Variation
Some surgeons prefer to combine Bassini hernia repair with the Hackenbruch doubling of the external oblique aponeurosis42 in the hope that this will further secure the hernial opening ( Fig. 2.26).
Fig. 2.26).
The operation concludes with a subcutaneous vacuum drain and skin suture.
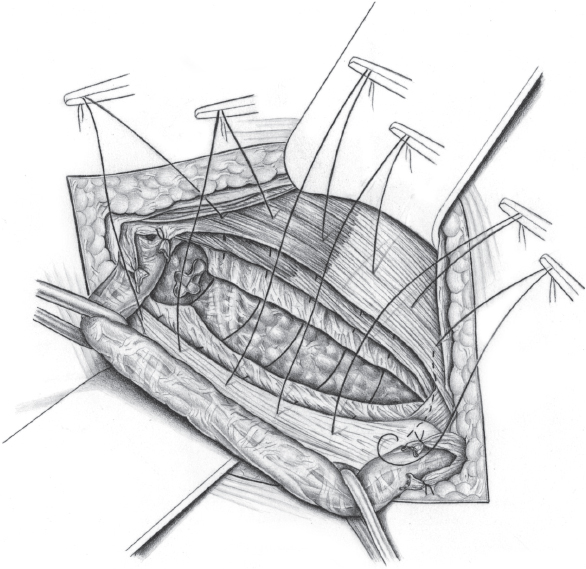
Fig. 2.21 Complete placement of 4–6 Bassini sutures, held with clamps.
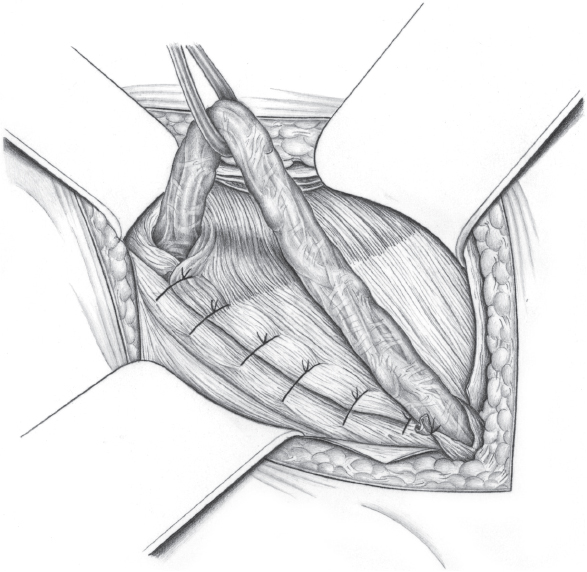
Fig. 2.22 Tying the Bassini sutures from medial to lateral. The deep ring is tightened so that it just admits the tip of a forceps or the tip of the little finger beside the spermatic cord.
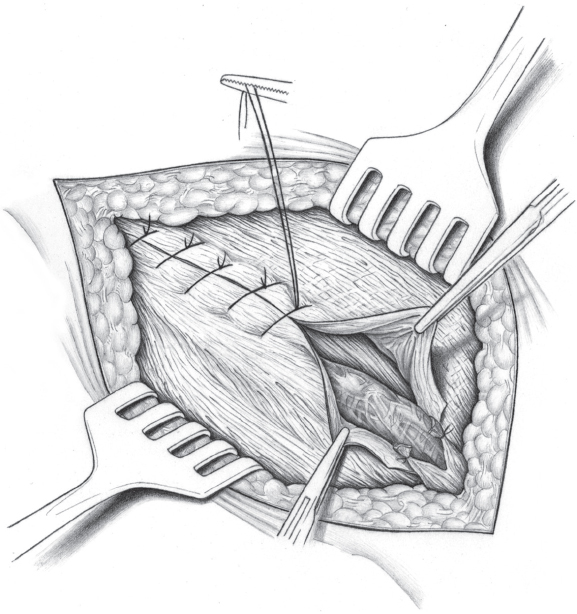
Fig. 2.23 Closure of the external oblique with interrupted or continuous sutures.
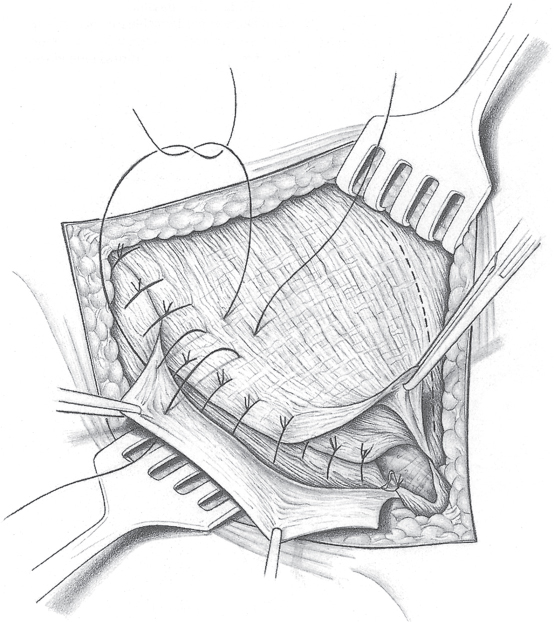
Fig. 2.24 Girard modification, doubling the external oblique aponeurosis in front of the spermatic cord.
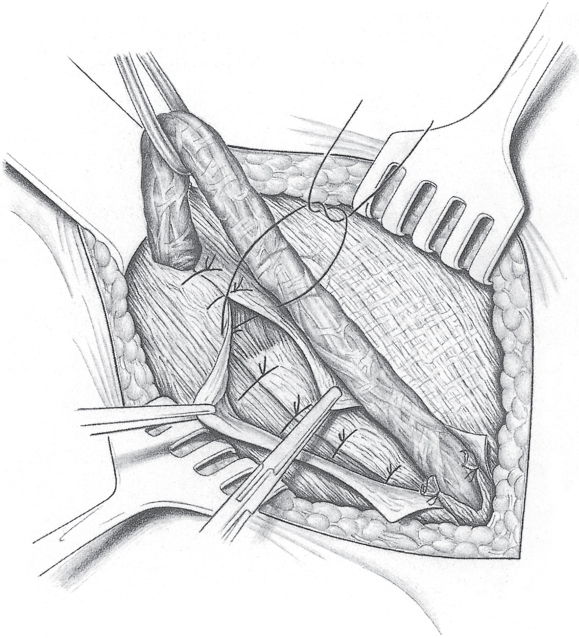
Fig. 2.25 The Kirschner modification of the external oblique aponeurosis closure by doubling it behind the spermatic cord.
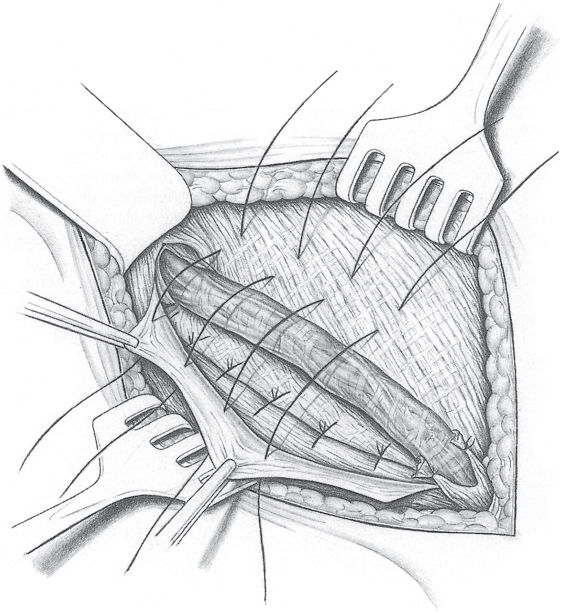
Fig. 2.26 The Hackenbruch modification of external oblique aponeurosis closure by doubling it and creating a new inguinal canal lined by fascia.
The Zimmerman Repair
Indication
The Zimmerman anterior sutured repair is suitable especially for small lateral hernias in young patients. It is indicated when the hernial opening at the deep inguinal ring (L1) is less than 1.5 cm in size following exposure of stable transversalis fascia with complete dissection of the spermatic cord from the deep ring. The deep ring is usually only moderately extended and irregular, and barely admits more than one fingertip ( Fig. 2.27).
Fig. 2.27).
Operation Preparation
• Preoperative diagnosis by clinical examination.
• Ultrasonography of the groin.
Special Risks
None apart from the usual complications of inguinal hernia repair:
• Spermatic cord injury (1%).
• Wound infection (2%).
• Chronic groin pain (< 5%).
• Recurrence (1–10%).
Anesthesia
Local anesthesia in cooperative patients, otherwise spinal or epidural anesthesia or general anesthesia.
Position
Supine.
Access
Transverse or slightly oblique incision above the inguinal crease.
Relevant Anatomy, Dangers, and Tricks
The crucial requirements for a successful outcome are medially stable transversalis fascia and accurate tightening of the deep ring without a risk of recurrence or strangulation.
Management of Special Complications
Ligature of epigastric vessels and suture of vas deferens if injured.
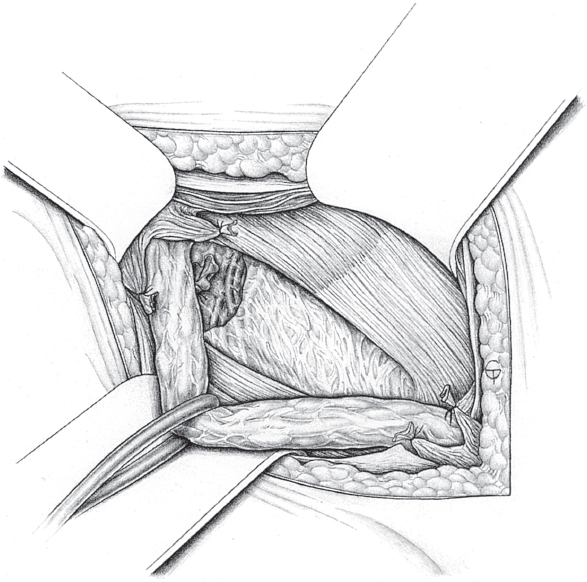
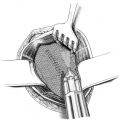
Fig. 2.27 Wide deep inguinal ring with the transversalis fascia otherwise strong as far as the pubic bone (L1): tightening of the deep ring by the Zimmerman method is indicated.
Postoperative Management
![]() Medical care.
Medical care.
• Male patients should wear close fitting underpants in the first few days.
• The patient should be provided with an information leaflet on gradual resumption of physical effort and sports activities.
![]() Diet. Immediately.
Diet. Immediately.
![]() Bowels. Enema if necessary.
Bowels. Enema if necessary.
![]() Mobilization. Immediately.
Mobilization. Immediately.
![]() Physical therapy. Not required.
Physical therapy. Not required.
Operation Techniques
Dissection of the preperitoneal fat is a precondition for safely tightening the deep inguinal ring. The spermatic cord is first snared and held under tension and the fat attached to the deep ring and transversalis fascia is pushed bluntly off the fascial margin. The edges of the deep ring are then grasped with Kocher clamps and drawn medially ( Fig. 2.28).
Fig. 2.28).
The superior part of the abdominal muscles is retracted to allow suture of the entire circumference of the deep ring. Suturing is done medial to the spermatic cord, and the cranial parts of the transversalis fascia and possibly the transversus abdominis aponeurosis and the inferior fibers of the iliopubic tract, and, if necessary, the inguinal ligament can be included in the suture. In Zimmerman’s original method, the caudal part of the iliopubic tract and the inguinal ligament are included ( Fig. 2.29).
Fig. 2.29).
Stable medial transversalis fascia is essential for this repair method. If this is weak and tenuous, it should be doubled completely, as in the Shouldice procedure. When the fascia is stable and especially when there is merely a persistent processus vaginalis, repair of the deep inguinal ring alone is just as safe. The deep ring should be tightened to fingertip width as there is a risk of recurrence if the deep ring is too wide but excessive tightening risks strangulation of the spermatic cord with a consequent danger of ischemic orchitis. An 11.5 Hegar dilator can be used for standardization. A continuous single-layer or two-layer suture is an alternative to a single row of interrupted sutures ( Fig. 2.30,
Fig. 2.30,  Fig. 2.31).
Fig. 2.31).
After tightening the deep inguinal ring, the internal oblique and transversus abdominis muscles can be fixed to the inguinal ligament in a single row of interrupted sutures or a two-row continuous suture, starting medially behind the spermatic cord. This corresponds to the Bassini and Shouldice reconstruction of the muscle plane. In Zimmerman’s original method, any fixation of muscle to the inguinal ligament is omitted to preserve its mobility. The operation ends with suture of the external oblique aponeurosis ( Fig. 2.32) after repositioning the spermatic cord, approximating subcutaneous interrupted sutures, and wound closure.
Fig. 2.32) after repositioning the spermatic cord, approximating subcutaneous interrupted sutures, and wound closure.
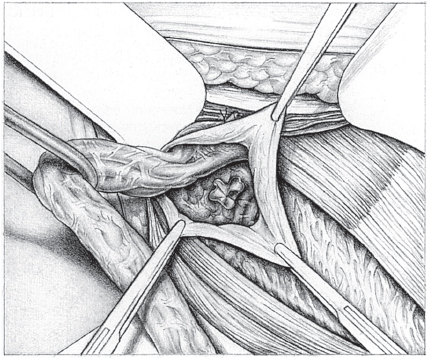
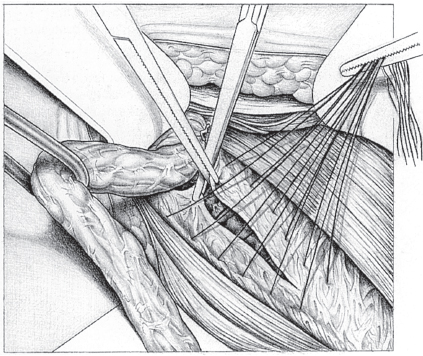
Fig. 2.29 Placing the sutures through the superior (transversus abdominis aponeurosis) and inferior (iliopubic tract) suture lines.
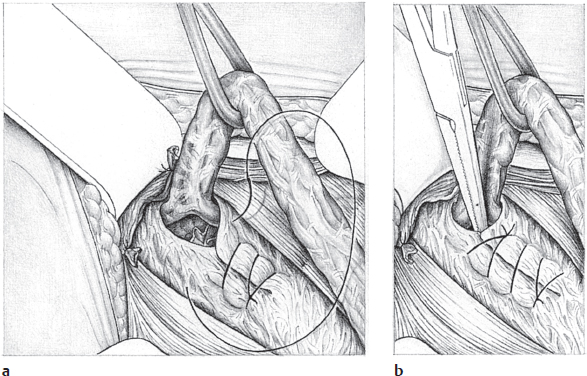
Fig. 2.30 Alternative reconstruction of the deep inguinal ring by a single-row continuous suture from medial to lateral (a). It is tightened until it just admits a closed clamp or forceps beside the spermatic cord (b).
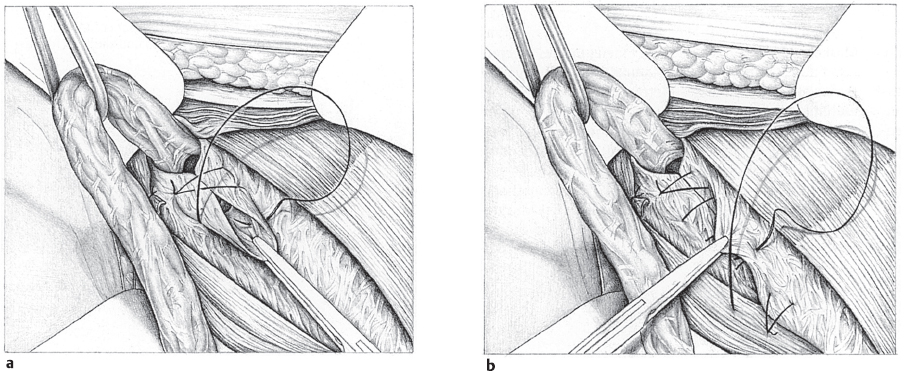
Fig. 2.31 a and b Alternative reconstruction of the deep inguinal ring by direct closure (a) and doubling of the superior layer of the transversalis fascia over the inferior layer (b). The suture starts laterally, turns around at the medial end, and continues back laterally.
Minimal Repair Technique
Indication
The minimal repair technique is an innovative operation technique that can be used for inguinal hernia repair and to treat sports hernia. Minimal repair is performed without insertion of mesh. The technique was developed by our working group in 2002 and we have now treated more than 3,500 patients with the minimal repair method.
The minimal repair technique is suitable for all patients in whom the consistency and structure of the transversalis fascia allows direct suture. Therefore, the final decision on this type of repair is often made only at operation after an assessment of the anatomy. We use the minimal repair technique mostly for groin pain due to sportsman’s groin (see section  3.2), where there is protrusion of the posterior wall of the inguinal canal with compression of the genital branch of the genitofemoral nerve (
3.2), where there is protrusion of the posterior wall of the inguinal canal with compression of the genital branch of the genitofemoral nerve ( Fig. 2.33). However, patients with a direct (M 1–2) or indirect (L 1–2) inguinal hernia are benefiting increasingly from the technique.
Fig. 2.33). However, patients with a direct (M 1–2) or indirect (L 1–2) inguinal hernia are benefiting increasingly from the technique.
In patients with sportsman’s groin, operative intervention is indicated, especially when targeted rest combined with anti-inflammatory medication is ineffective within 6 to 8 weeks. This recommendation is based on the highest available level of medical evidence. In a randomized study,27 professional footballers with the described symptom complex were divided into four groups: a control group without treatment, two treatment arms with different physical exercise programs, and a group treated surgically. Patients who had reinforcement of the inguinal canal (posterior wall) and neurolysis and neurectomy of the genital branch of the genitofemoral nerve had a significantly better outcome 6 months after the respective treatment.
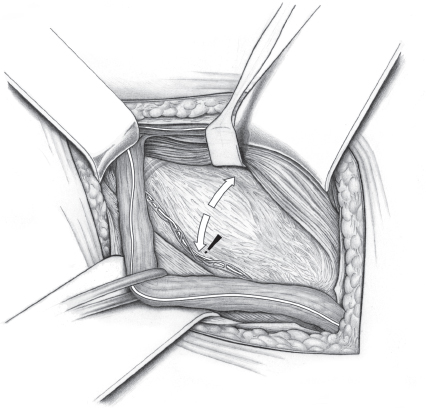
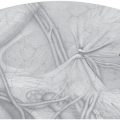
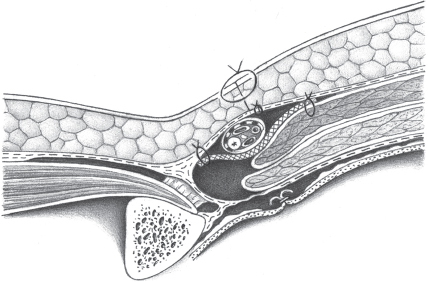
Fig. 2.33 Pathomechanism of “sportsman’s groin.” Weakness of the posterior wall of the inguinal canal can cause sudden or chronic recurrent irritation of the genital branch of the genitofemoral nerve.
The preoperative diagnostic tests are described in section  3.2.
3.2.
Special Risks and Informed Consent
When selecting treatment, conservative management should always be considered first, if this has not been attempted already. When the history and clinical symptoms are consistent, however, one should be aware that further delay of surgery may lead to chronification rather than improvement of the symptoms. Conservative therapy should therefore not continue longer than 6 to 8 weeks.
Patients must be given complete preoperative information about risks such as secondary bleeding, seroma, wound infection, spermatic cord injury, testicular atrophy, chronic groin pain, and persistent numbness, and about the possibility of recurrence.
Anesthesia
The operation is performed under local conduction anesthesia, which is injected at the anterior superior iliac spine and in the area of the planned skin incision. The ilioinguinal and iliohypogastric nerves and the genital branch of the genitofemoral nerve are exposed at operation and local anesthetic is injected directly into the perineurium.
The patient is fully monitored by an anesthesiologist. Concomitant analgosedation can be given if the patient wishes.
Position
As in inguinal hernia surgery, the operation is performed with the patient in the supine position.
To relieve the groin region, gel pads are place beneath the buttocks and knees.
To minimize wound infections, appropriate sterile preparation of the operation field including the genital region, must be ensured. An adhesive incision drape is applied to the skin.
Access
The incision is similar to the classic inguinal hernia incision in the groin but is only 4 cm long. The distal medial part of the incision should be slightly oblique to allow adequate dissection on the pubic bone.
Relevant Anatomy, Dangers, and Tricks
Sportsman’s groin is often due to irritation of the genital branch of the genitofemoral nerve ( Fig. 2.33). The circumscribed weakness of the transversalis fascia forces apart the matrix of muscle fasciae and tendons passing to the pubic bone, and symptoms are worsened by pinpoint stress on the bone insertion sites on the pubic bone. This was described by Morales-Conde73 as “syndrome of muscle imbalance of the groin.”
Fig. 2.33). The circumscribed weakness of the transversalis fascia forces apart the matrix of muscle fasciae and tendons passing to the pubic bone, and symptoms are worsened by pinpoint stress on the bone insertion sites on the pubic bone. This was described by Morales-Conde73 as “syndrome of muscle imbalance of the groin.”
The epigastric vessels posterior to the transversalis fascia, with their cremasteric branches, are at risk during dissection of the inferior fascial leaf that is needed for the first row of sutures. In most cases, it should be possible to push back the epigastric vessels by blunt dissection, resecting the small branches of the cremasteric vessels, and this will create a fascial border 0.5 cm wide for this row of sutures.
Complication Rate
The management of special complications is generally identical with that of regular hernia surgery.
A prospective study of recurrence after minimal repair of inguinal hernia is currently in progress. The initial results show that the outcome is similar to or better than the compared methods (Shouldice, Lichtenstein). As mesh implantation is omitted, the rate of postoperative seroma and hematoma is much lower compared with the Lichtenstein repair. The abdominal wall muscles still slide smoothly, which is essential, especially for athletes.
Postoperative Management
When the patient is discharged on the day of operation, postoperative care includes ultrasonography including Doppler ultrasound of the testis on the operated side. Adequate nonsteroidal anti-inflammatory analgesia is prescribed.
For patients with sportsman’s groin, we draw up an individual training program with the following guidelines: light running is permitted from the second postoperative day. Training units are increased from the third day, and full stress is permitted from the fifth day. Full stress without any restriction, including high-performance sport, should always be possible after 10 to 14 days.
Results of Minimal Repair of Sportsman’s Groin
According to an Australian study in footballers,112 the risk of symptom persistence after a year is 59% with conservative treatment only.
In our study of 132 consecutive patients who underwent minimal repair surgery, 78.9% were completely asymptomatic a median 14 days after the operation (range 7–28 days). 83.3% of the professional athletes in this group (87 of 129; 67%) reached their peak preoperative performance after a median 14 days (range 10–28 days).74
Operation Techniques
Following dissection of the subcutaneous tissue, the external oblique aponeurosis is exposed and is split from lateral to medial above the midline. It is important that the ilioinguinal nerve and more superior iliohypogastric nerve beneath the aponeurosis are not injured. The nerves should not be mobilized from their fascia. The cremaster muscle should always be preserved in full. The pampiniform plexus is snared together with the ilioinguinal nerve.
The posterior wall of the inguinal canal can then be palpated directly and the weak area of tissue can be exposed ( Fig. 2.33).
Fig. 2.33).
The defect is now opened ( Fig. 2.34).
Fig. 2.34).

Caution
To ensure that the defect is not extended, it is important to grasp the edges of the defect precisely with small sharp forceps and dissect it accurately.
The genital branch of the genitofemoral nerve must always be exposed and its surface assessed. If this is smooth and shining, resection can be omitted. If the nerve surface is dull and yellowish, and macroscopically fibrosed, resection is advisable. Resection is also recommended if the anatomical position of the nerve prevents adequate closure of the posterior wall defect at the deep inguinal ring.
When dissecting the leaf of fascia needed for the first row of sutures, it is important that these can be placed without tension. The inferior leaf is dissected from the iliopubic tract from superomedial to inferolateral, avoiding inclusion of the inguinal ligament in the first row of sutures. It is also important not to go beyond the fascial border of the defect ( Fig. 2.35). The first row of sutures starts at the medial edge of the defect, placing them from inferior to superior. As in the Shouldice repair, the white line is the superior boundary.
Fig. 2.35). The first row of sutures starts at the medial edge of the defect, placing them from inferior to superior. As in the Shouldice repair, the white line is the superior boundary.
The superior leaf of fascia created by the first suture is now grasped and fixed by a continuous suture to the lowest point of the inguinal ligament ( Fig. 2.36), using a 2/0 monofilament nonabsorbable suture (e.g., Prolene). The suture turns back at the deep inguinal ring, which it tightens; it should still admit an 11.5 mm Hegar dilator easily. The suture is now continued medially to the pubic bone to lateralize the rectus abdominis thereby reducing the vertical pull on the pubic bone (
Fig. 2.36), using a 2/0 monofilament nonabsorbable suture (e.g., Prolene). The suture turns back at the deep inguinal ring, which it tightens; it should still admit an 11.5 mm Hegar dilator easily. The suture is now continued medially to the pubic bone to lateralize the rectus abdominis thereby reducing the vertical pull on the pubic bone ( Fig. 2.37).
Fig. 2.37).
Finally ( Fig. 2.38), the pampiniform plexus with the preserved ilioinguinal nerve is protected from mechanical irritation by forming a small lateral lip of the internal oblique muscle. The external oblique aponeurosis is then doubled by a two-row continuous suture using monofilament absorbable material (e.g., Monocryl, 3/0) with the spermatic cord replaced in subfascial position. After careful hemostasis, the wound can now be closed in layers with a continuous subcutaneous suture. A vacuum drain is not placed. The skin is closed with a continuous absorbable intracutaneous suture, e.g., Monocryl 4/0.
Fig. 2.38), the pampiniform plexus with the preserved ilioinguinal nerve is protected from mechanical irritation by forming a small lateral lip of the internal oblique muscle. The external oblique aponeurosis is then doubled by a two-row continuous suture using monofilament absorbable material (e.g., Monocryl, 3/0) with the spermatic cord replaced in subfascial position. After careful hemostasis, the wound can now be closed in layers with a continuous subcutaneous suture. A vacuum drain is not placed. The skin is closed with a continuous absorbable intracutaneous suture, e.g., Monocryl 4/0.
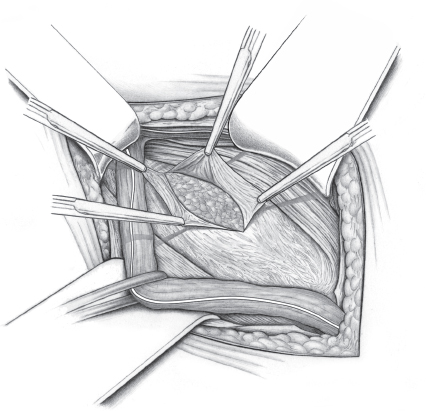
Fig. 2.34 After dissecting the subcutaneous tissue and splitting the external oblique aponeurosis, the posterior wall of the inguinal canal is exposed and the weak area of tissue is opened, without enlarging the defect. The genital branch of the genitofemoral nerve is assessed macroscopically and resected if necessary.
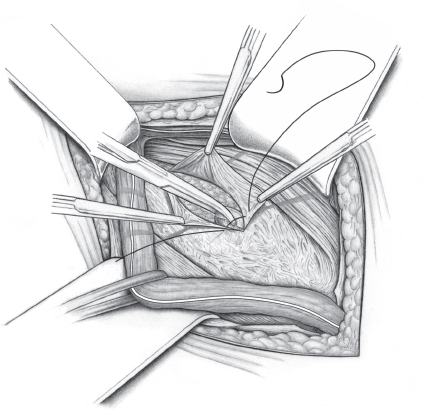
Fig. 2.35 After splitting the transversalis fascia and creating the inferior leaf of fascia from the iliopubic tract, the inferior leaf is fixed to the posterior wall of the superior leaf with a continuous suture, starting medially. The superior boundary is the white line. The suture is tied medially and positioned below the second row of sutures.
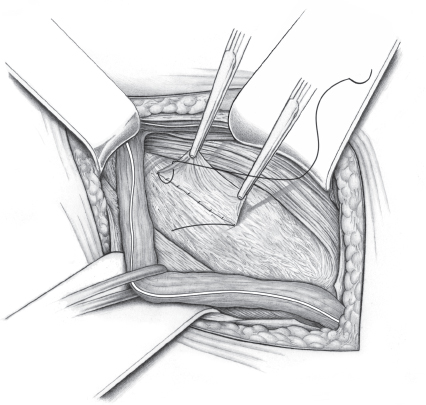
Fig. 2.36 The resulting layer of fascia is doubled from superior to distal with a continuous suture. The suture picks up the inguinal ligament deeply, thus reinforcing the anterior abdominal wall.
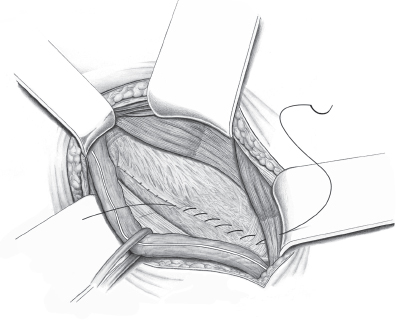
Fig. 2.37 With this suture, the rectus abdominis is lateralized, thereby reducing the vertical pull on the pubic bone.
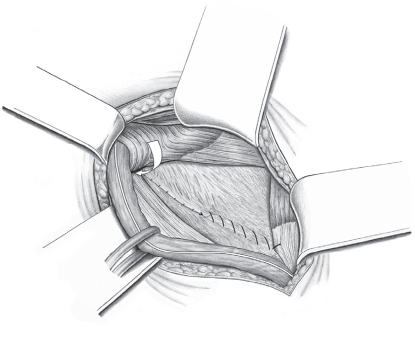
Fig. 2.38 Creation of a lateral sleeve of muscle with the lower border of the internal oblique around the spermatic cord to reinforce the deep inguinal ring and protect the pampiniform plexus against mechanical irritation.
Shouldice Repair
Indication
This is the standard open anterior hernia repair nowadays.
After exposing the deep inguinal ring, the index finger (of the left hand on the right side and right hand on the left side) is inserted in the deep ring to test the resistance of the transversalis fascia to pressure from behind. This test is unnecessary with medial hernias as fascial defects requiring repair are present in any case, and fascial doubling is indicated.
With lateral hernias, extensive weakness is found in nearly 90% of the cases, indicating additional fascial doubling. Occasionally, for instance with small hernias, only the lateral part of the fascia is thinned. In this situation, partial splitting and repair will suffice. The transition with the Zimmerman procedure of only tightening the deep inguinal ring is fluid.
Operation Techniques
Repair Principle
See  Fig. 2.39.
Fig. 2.39.
Digital Examination of Fascial Stability
See  Fig. 2.40.
Fig. 2.40.
Splitting of the Transversalis Fascia
The first step is to split the transversalis fascia obliquely from the deep inguinal ring toward the pubic tubercle ( Fig. 2.41). The length of the incision is guided by the extent of the fascial weakness or hernial orifice but usually extends fully to the pubic bone. Partial splitting followed by doubling occasionally suffices with small indirect hernias and stable transversalis fascia. With large direct hernias, it is often difficult to identify the fascial edges. These should be dissected gradually off the hernial sac and marked with the Kocher clamps. After managing the sac, fascial doubling can take place.
Fig. 2.41). The length of the incision is guided by the extent of the fascial weakness or hernial orifice but usually extends fully to the pubic bone. Partial splitting followed by doubling occasionally suffices with small indirect hernias and stable transversalis fascia. With large direct hernias, it is often difficult to identify the fascial edges. These should be dissected gradually off the hernial sac and marked with the Kocher clamps. After managing the sac, fascial doubling can take place.
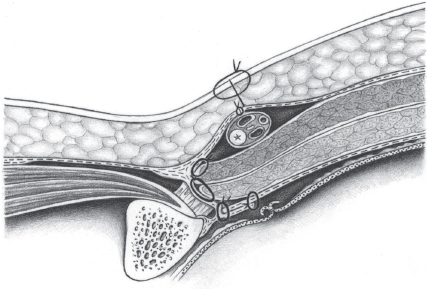
Fig. 2.39 The principle of the Shouldice inguinal hernia repair consists of doubling of the defective transversalis fascia by two continuous rows of fascial suture and attachment of the transverse and internal oblique muscles to the inguinal ligament by a continuous suture. The spermatic cord is positioned in front of the muscle and behind the external oblique aponeurosis.
When incising the transversalis fascia, the epigastric vessels beneath it must be carefully preserved. They are located in the loose preperitoneal fat and usually comprise two veins and one artery. Collateral vessels to the spermatic cord (the external cremasteric vessels) are regularly found and must be ligated between clamps and divided. Without this precaution, persistent and troublesome bleeding can occur. If the epigastric vessels are injured, they must be double ligated and divided.
Dissection of the Superior Fascial Layer
After splitting the transversalis fascia, the superior part is grasped with sharp forceps and dissected bluntly from the preperitoneal fat ( Fig. 2.42). The femoral canal can be demonstrated inferiorly. Any femoral hernia is first closed.
Fig. 2.42). The femoral canal can be demonstrated inferiorly. Any femoral hernia is first closed.
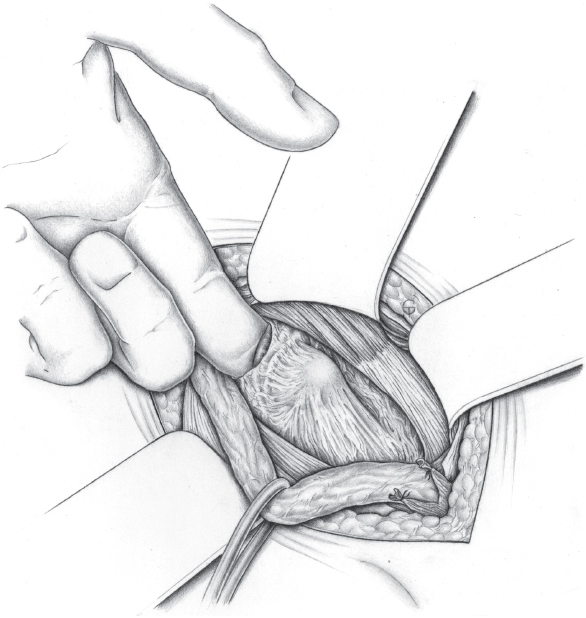
Fig. 2.40 Digital examination of the strength of the transversalis fascia by palpation through the deep inguinal ring. If the wall is weak, the transversalis fascia may bulge forward. Fascial doubling using the Shouldice method is indicated for small fascial defects or weak areas; Lichtenstein mesh repair is indicated for bigger defects (see section  2.3.1).
2.3.1).
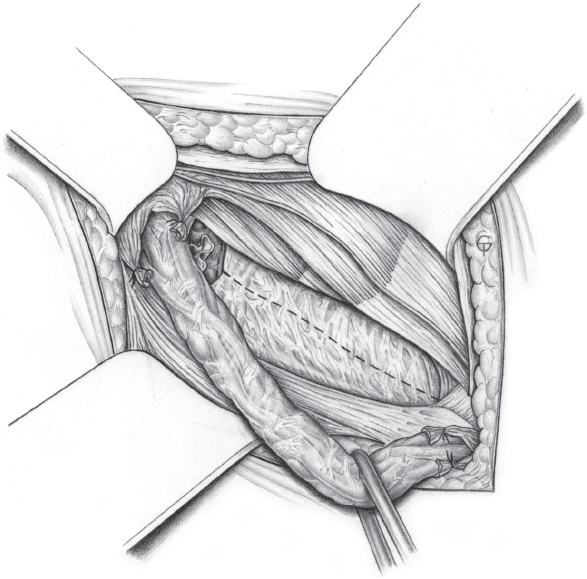
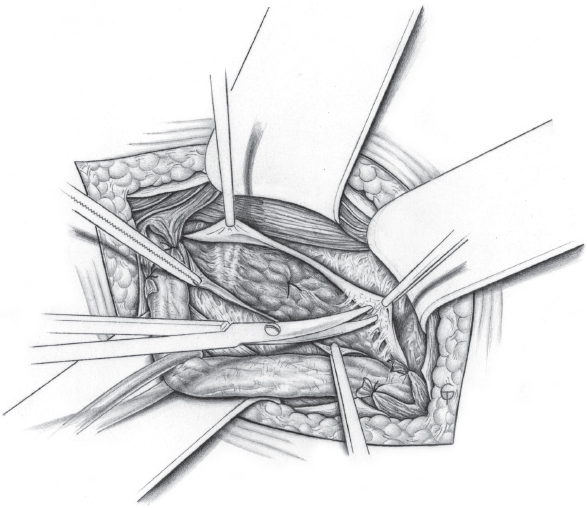
Fig. 2.42 Dissection of the superior fascial layer from the underlying preperitoneal fat until the lateral border of the rectus sheath and arch of the transversus abdominis aponeurosis (the white line) are exposed. This is followed by sparing dissection of the inferior leaf.
Excision of Defective Fascia and Creation of Stable Borders
The inferior leaf of the transversalis fascia should be mobilized only until the femoral hernial orifice is visualized. It too is grasped with sharp forceps. If the central part is thin and fragile, it is resected to provide strong edges that can be sutured ( Fig. 2.43). The superomedial leaf of the transversalis fascia is usually narrower than the inferolateral one, which should be approximately 1.5 to 2.0 cm wide, if possible.
Fig. 2.43). The superomedial leaf of the transversalis fascia is usually narrower than the inferolateral one, which should be approximately 1.5 to 2.0 cm wide, if possible.
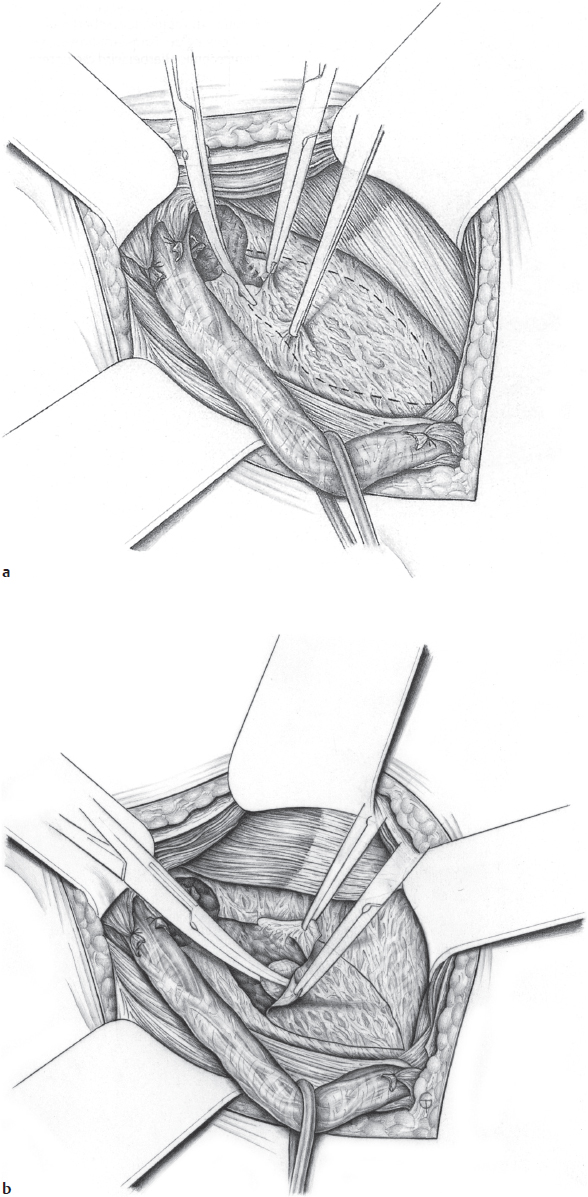
Fig. 2.43 When there is a fascial defect with a large medial hernia, the weak part of the fascia is resected. It is incised (a) and dissected off (b) to leave the edges that can be sutured.
First Suture “Lower Below Upper” from Medial to Lateral
Repair of the transversalis fascia starts with suture of the inferior leaf behind the superior leaf. The first suture is placed in the medial corner of the fascia at the pubic tubercle and fixes the caudal border of the divided transversalis fascia to the underside of the cranial part ( Fig. 2.44). In the medial part, the sutures are placed in the posterior surface of the rectus sheath, which gleams through the transversalis fascia (the “white line”). In the lateral segment, the sutures are placed in the tendinous part of the transversus abdominis aponeurosis. The suture is continuous, placed at intervals of 0.6 cm, and each stitch is inserted 0.6 to 1.0 cm from the edge of the tissue.
Fig. 2.44). In the medial part, the sutures are placed in the posterior surface of the rectus sheath, which gleams through the transversalis fascia (the “white line”). In the lateral segment, the sutures are placed in the tendinous part of the transversus abdominis aponeurosis. The suture is continuous, placed at intervals of 0.6 cm, and each stitch is inserted 0.6 to 1.0 cm from the edge of the tissue.
The suture (monofilament, polypropylene 0 to 2/0 or PDS 0 to 2/0) should be under even tension and not too tight so that a continuous approximation is obtained. After inserting the first stitch at the pubic tubercle, the suture is tied, leaving a long end. The suture is continued as far as the deep inguinal ring, where the superior part of the cremaster muscle can be included. Additional securing (“plugging”) of the deep hernial orifice can be achieved in this way. The deep ring should be tightened so that it admits the index finger tip or a 11.5 Hegar dilator alongside the spermatic cord, which has been dissected free of the cremaster.
Second Suture “Upper Over Lower” from Lateral to Medial
Starting from the deep inguinal ring, the suture direction is reversed and continues by suturing the cranial to the caudal leaf from above. The sutures are placed in the iliopubic tract ( Fig. 2.45) and the insertion of the inguinal ligament.
Fig. 2.45) and the insertion of the inguinal ligament.
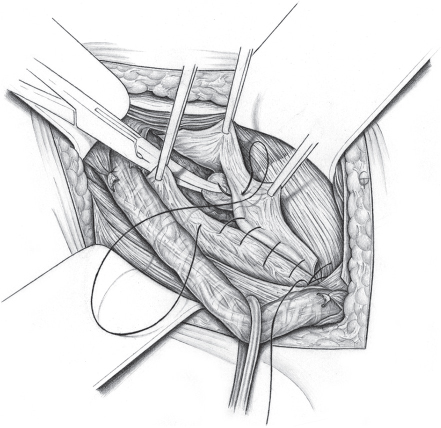
Fig. 2.44 Start of fascial doubling medially on the pubic periosteum with a continuous suture. The caudal leaf of the transversalis fascia is sutured below the cranial leaf, pushing the preperitoneal fat back with a swab.
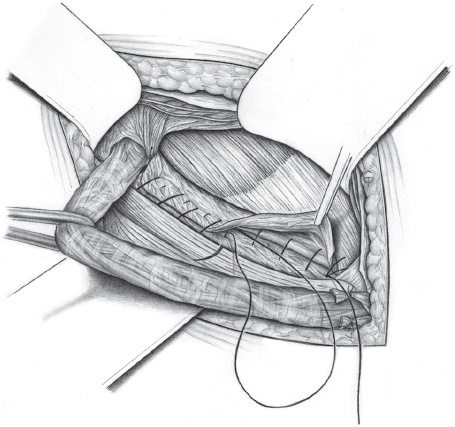
Fig. 2.45 Second fascial suture from lateral to medial attaching the cranial leaf to the caudal one. The sutures are placed in the iliopubic tract at the base of the inguinal ligament. The suture is continuous.
Medial Oversewing of the First Knot and Tying
After the pubic tubercle is reached, the continuous suture is continued two more stitches medially ( Fig. 2.46a) to prevent suprapubic recurrence. After turning around and locking it at the pubic tubercle, the suture is tied with the long end left at the start (
Fig. 2.46a) to prevent suprapubic recurrence. After turning around and locking it at the pubic tubercle, the suture is tied with the long end left at the start ( Fig. 2.46b).
Fig. 2.46b).
Third Suture as First Muscle Suture
When the double row of fascial sutures is complete, the transversus abdominis muscle is fixed to the inguinal ligament with a continuous suture, starting from the deep inguinal ring. This suture is fixed at the base of the inguinal ligament to avoid any dead space ( Fig. 2.47).
Fig. 2.47).
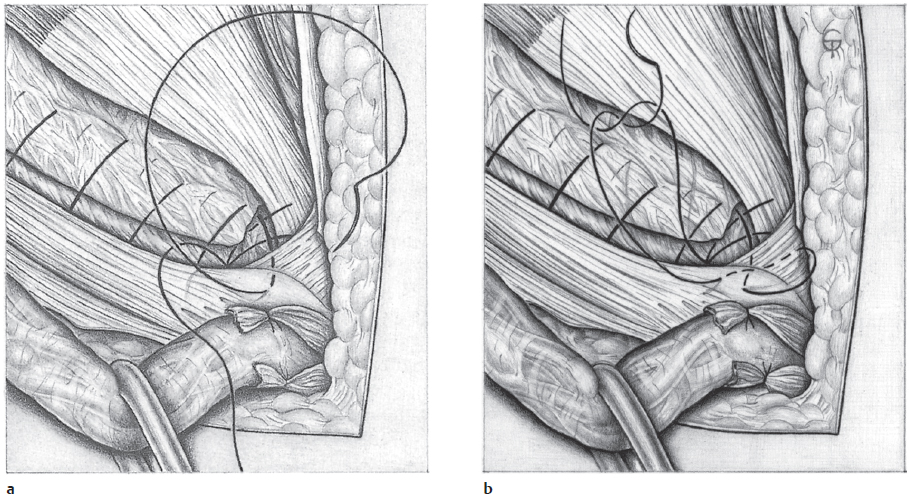
Fig. 2.46 At the medial end, the suture is continued over the reflected ligament (a) and then returns to the starting point (b). Here it is tied with the initial long end.
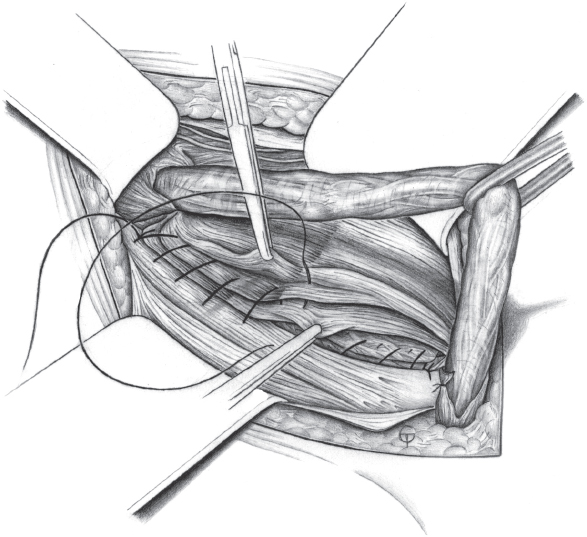
Fig. 2.47 Attachment of the muscle to the inguinal ligament by a two-row continuous suture, starting laterally. The first row picks up the transversus muscle and the lower edge of the internal oblique.
Fourth Suture as Second Muscle Suture
After the deep muscle suture has reached the pubic bone, it turns back to fix the internal oblique to the inguinal ligament in a fourth row ( Fig. 2.48).
Fig. 2.48).
When the deep inguinal ring is reached, the continuous suture is tied with the long end of the first muscle suture. According to Berliner,9 the double attachment of the muscle can achieve a similarly good result with a single row of sutures that combine both muscle components. We prefer two rows of suture because of the better attachment of the muscles.
Closure of the External Oblique Aponeurosis
The external oblique aponeurosis is closed over the spermatic cord with a single-row continuous suture using 2/0 PDS (Maxon;  Fig. 2.49). The operation concludes with an optional subcutaneous vacuum drain (not used routinely) and skin suture.
Fig. 2.49). The operation concludes with an optional subcutaneous vacuum drain (not used routinely) and skin suture.
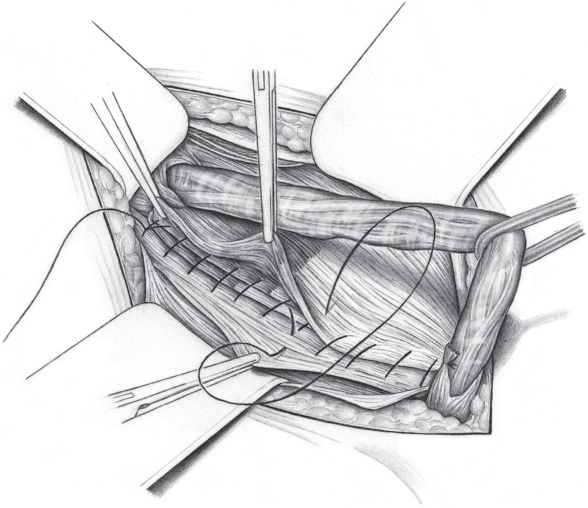
Fig. 2.48 Second row of the muscle suture, attaching the anterior parts of the internal oblique to the inguinal ligament using a continuous suture from medial to lateral.
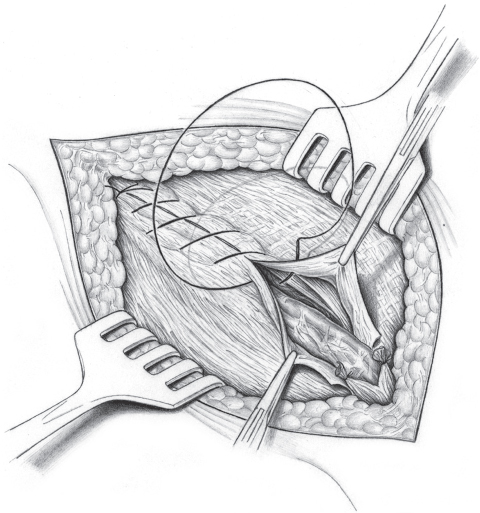
Fig. 2.49 Closure of the external oblique aponeurosis by a continuous suture.
Lotheissen/McVay Repair
Indication
The Lotheissen/McVay anterior sutured repair is rarely used nowadays; it is technically complex, painful, and often unsafe, as the elastic muscles may tear out of the Cooper ligament, which is attached to bone, in the long term. TEP is a better alternative today.
Operation Preparation
The preoperative diagnosis is made by clinical examination, ultrasonography of the groin, and Doppler ultrasound of the testicular vessels in the case of surgery for recurrence.
Special Risks
None apart from the usual complications of inguinal hernia repair:
• Spermatic cord injury (1%).
• Wound infection (2%).
• Chronic groin pain (< 5%).
• Recurrence (1–10%).
Anesthesia
Local anesthesia in cooperative patients, otherwise spinal or epidural anesthesia or general anesthesia.
Position
Supine.
Access
Transverse or slightly oblique incision above the inguinal crease.
Relevant Anatomy, Dangers, and Tricks
Adequate exposure of the often deep structures, especially in obese patients, is crucial for success.
Management of Special Complications
Ligature of the corona mortis and suture of the femoral vein if injured.
Postoperative Management
![]() Medical care. Male patients should wear close fitting underpants in the first few days and the patient should be provided with an information leaflet on gradual resumption of physical effort and sports activities.
Medical care. Male patients should wear close fitting underpants in the first few days and the patient should be provided with an information leaflet on gradual resumption of physical effort and sports activities.
![]() Diet. Immediately.
Diet. Immediately.
![]() Bowels. Enema if necessary.
Bowels. Enema if necessary.
![]() Mobilization. Immediately.
Mobilization. Immediately.
![]() Physical therapy. None required.
Physical therapy. None required.
Operation Techniques
The transversalis fascia is split along its entire length where it is still present ( Fig. 2.50).
Fig. 2.50).
After splitting the transversalis fascia, the preperitoneal space is opened and the peritoneal sac can be dissected bluntly off the pectineal (Cooper) ligament with a swab. The horizontal ramus of the pubic bone and the pectineal ligament overlying it are exposed laterally from the lacunar (Gimbernat) ligament in the medial corner of the wound ( Fig. 2.51).
Fig. 2.51).
The anastomosis between the inferior epigastric artery and the obturator artery, the corona mortis, varies in caliber and must be protected. The pectineal ligament is located considerably deeply, especially in obese patients, and can be exposed only by generous use of retractors. In the lateral part of the wound, the vascular sheath is seen with the femoral vein medially, and this is retracted laterally. The hernia is repaired by attaching the triple layer consisting of transversalis fascia, transversus abdominis, and internal oblique to the pectineal ligament. It is technically simpler to place five to six nonabsorbable sutures (2/0) in the inferior column first. The most medial suture picks up the lacunar (Gimbernat) ligament as well as the periosteum of the pubic tubercle. The average distance to be bridged is 4 cm ( Fig. 2.52).
Fig. 2.52).
Elevation of the internal oblique muscle exposes the cranial suture line consisting of transversalis fascia, the aponeurosis of the transversus abdominis, and the internal oblique muscle. The sutures pass through the three layers from posterior to cranial. Once all the sutures have been placed, they are tied from medial to lateral so that the knots lie increasingly deep. The sutures are placed as laterally as possible, sparing the femoral vein ( Fig. 2.53).
Fig. 2.53).
McVay recommends concluding the sutures laterally with a “transition stitch,” which includes the pectineal ligament and femoral vascular sheath as well as the triple-layered abdominal muscle. This is intended to prevent a perivascular hernia. The transversalis fascia can be reconstructed by the Zimmerman method if it is still gaping at the deep inguinal ring to prevent later indirect recurrence ( Fig. 2.54).
Fig. 2.54).
A relieving incision of the rectus sheath is obligatory; this greatly reduces suture tension ( Fig. 2.55). Closure of the external oblique aponeurosis after replacement of the spermatic cord and wound closure as usual conclude the operation.
Fig. 2.55). Closure of the external oblique aponeurosis after replacement of the spermatic cord and wound closure as usual conclude the operation.
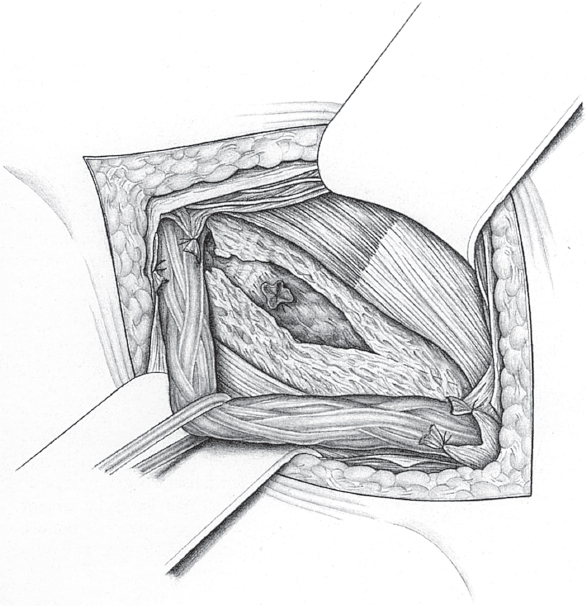
Fig. 2.50 Direction and extent of the splitting of the transversalis fascia on the posterior wall of the inguinal canal, shown here with a repaired direct hernial sac.
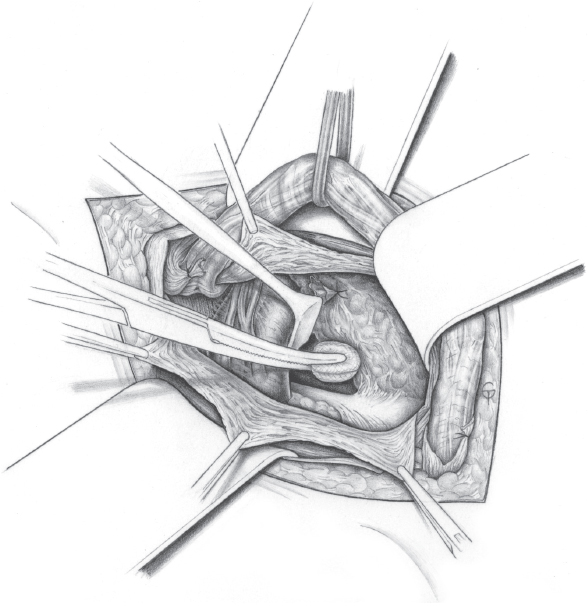
Fig. 2.51 After splitting the transversalis fascia, the preperitoneal fat is pushed bluntly in posterosuperior direction and the pectineal (Cooper) ligament is exposed.
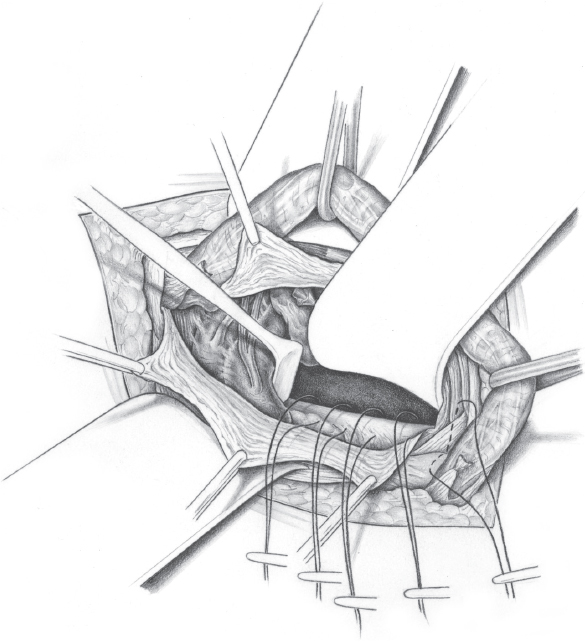
Fig. 2.52 Placement of the sutures at the medial end of the wound and in the pectineal (Cooper) ligament.
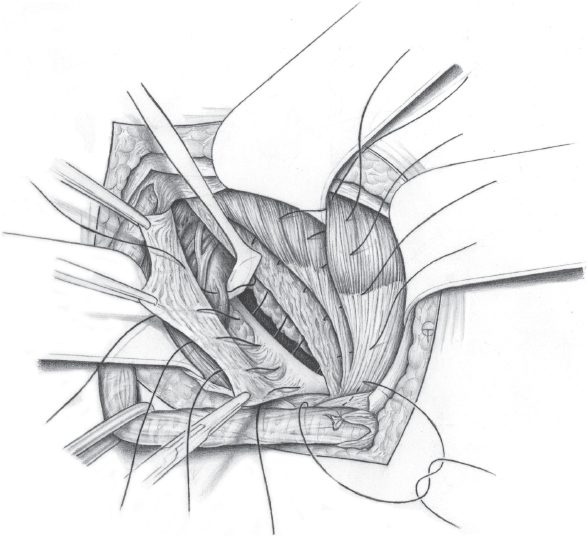
Fig. 2.53 The cranial ends of the sutures are passed through the three cranial layers of the suture line. The femoral vascular sheath is included in the suture laterally, sparing the femoral vein (transition stitch).
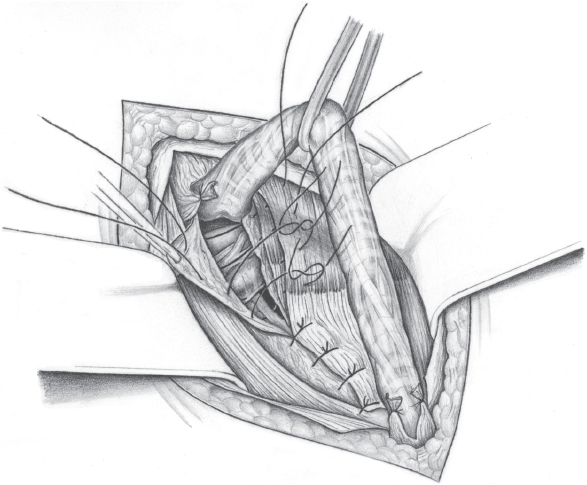
Fig. 2.54 Closure of the posterior wall of the inguinal canal after tying the medial sutures and tightening the deep inguinal ring laterally with interrupted sutures as in the Zimmerman procedure.
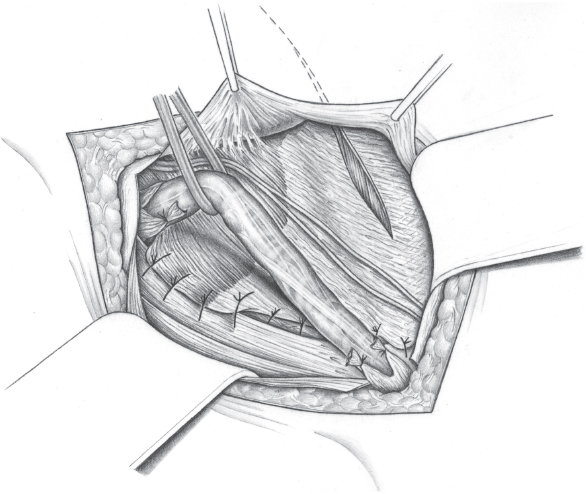
Fig. 2.55 Full reconstruction of the posterior wall of the inguinal canal and relieving incisions in the rectus sheath.
2.3 Open Mesh Techniques
2.3.1 Lichtenstein Repair
Repair Principle
The principle of the Lichtenstein repair is to reinforce the posterior wall of the inguinal canal by a mesh measuring approximately 6 × 14 cm, which, in the transinguinal method, is placed behind the spermatic cord from the base of the inguinal ligament as far as the internal oblique muscle ( Fig. 2.56). The procedure was developed in the 1970s by I.L. Lichtenstein (Los Angeles, CA, United States of America) and has spread worldwide in the past 20 years as, it is a relatively simple procedure technically that can be performed under local anesthesia.
Fig. 2.56). The procedure was developed in the 1970s by I.L. Lichtenstein (Los Angeles, CA, United States of America) and has spread worldwide in the past 20 years as, it is a relatively simple procedure technically that can be performed under local anesthesia.
Indication
The Lichtenstein repair is suitable for all direct and indirect hernias that require mesh repair and for repair of femoral hernias through an inguinal approach.
Operation Techniques
The operation can be performed under local anesthesia, epidural or spinal anesthesia, or general anesthesia (laryngeal mask or intubation).
It starts with the usual technique of transinguinal dissection until the inguinal canal is exposed.

Background
In the original description3 resection of the cremaster muscle was omitted, the spermatic cord was snared together with the ilioinguinal nerve and the external cremasteric vessels including the genital branch of the genitofemoral nerve, the hernial sac was reduced without opening it after appropriate dissection, and the hernial orifice was merely covered with the mesh without further treatment. The sac should be buried over an absorbable suture only in the case of large direct hernias. All the nerves located in the operation field (genital branch, ilioinguinal and iliohypogastric nerves) should be left intact. The mesh size was reported to be 8 × 16 cm.
Since then, a series of studies have shown that the treatment of the nerves must be revised. Consistently leaving sensory nerves in the operation field in direct contact with the mesh is associated with a high rate of postoperative chronic pain and foreign body sensation.87 When in doubt, the current recommendation is for optional neurectomy at the primary operation.
In the past 15 years, several modifications of the Lichtenstein technique have been described. These have addressed mesh size and material and the form of fixation. In the great majority, the aim of these modifications was to reduce the risk of postoperative pain.41
The Lichtenstein repair technique as currently employed by most surgeons is described below.
For indirect hernias, after opening the inguinal canal, the cremaster muscle is split over the deep inguinal ring, the preperitoneal lipoma is resected, and the sac is reduced.
In the case of direct hernias, the spermatic cord together with the cremaster sleeve is snared initially and the sac is reduced.

Tip
To secure sac reduction, a continuous suture is recommended between the superior and inferior margins of the transversalis fascia from medial to latera l, e.g., with 2/0 polypropylene or PDS.
In our experience, the external cremasteric vessels should not be snared with the genital branch that runs in the floor of the inguinal canal but should be ligated and divided together with the nerve laterally where they join the deep epigastric vessels. This allows optimal medial mesh coverage at the deep inguinal ring and prevents painful irritation of the nerve by the mesh.
The ilioinguinal nerve can be left in place on the cremaster muscle unless it has to be dissected and moved from its enclosing fascia to avoid direct mesh-nerve contact. Otherwise, infiltration with local anesthetic followed by neurectomy lateral to the deep inguinal ring is recommended.47
A large-pore, lightweight mesh is recommended for the repair. It should measure 6 × 14 cm and be cut as per the size ( Fig. 2.57). Mesh fixation starts over the pubic bone with a U-shaped suture (e.g., Prolene 2/0), without picking up the periosteum. The mesh should overlap by 1 cm medially.
Fig. 2.57). Mesh fixation starts over the pubic bone with a U-shaped suture (e.g., Prolene 2/0), without picking up the periosteum. The mesh should overlap by 1 cm medially.
The suture is continuous, attaching the inferior border of the mesh to the base of the inguinal ligament as far as immediately lateral to the deep inguinal ring ( Fig. 2.58).
Fig. 2.58).
From the lateral side, the mesh is incised 2 cm above the lower edge of mesh as far as the medial boundary of the deep inguinal ring. The cranial tongue is wrapped around the spermatic cord, and the medial part of the mesh is placed on the internal oblique muscle beneath the spermatic cord.

Caution
The iliohypogastric nerve, which emerges from the internal oblique and penetrates the external oblique aponeurosis, must be noted. Direct mesh-nerve contact must be avoided.
It is then fixed to the internal oblique fascia with 2–3 interrupted sutures (e.g., 2/0 Prolene), which should preferably not be tight so as not to irritate the iliohypogastric nerve running within the muscle ( Fig. 2.59).
Fig. 2.59).
The inferior edge of the cranial tongue of mesh, lateral to the deep inguinal ring is sutured to the base of the inguinal ring together with the caudal tongue beneath it and the projecting parts of the mesh are pushed laterally under the external oblique aponeurosis ( Fig. 2.60).
Fig. 2.60).
To treat a femoral hernia, caudal mesh fixation, medial to the femoral vessels is not to the inguinal ligament but more deeply to the Cooper ligament. When repairing inguinal hernias, mesh fixation with fibrin glue is a possible alternative that has been well investigated.78 To date, there have been no studies in this regard for the rarer femoral hernia and mesh fixation with a continuous suture is recommended.
The operation concludes with closure of the external oblique aponeurosis in front of the spermatic cord and suture of the Scarpa fascia and skin. A vacuum drain is usually not required.
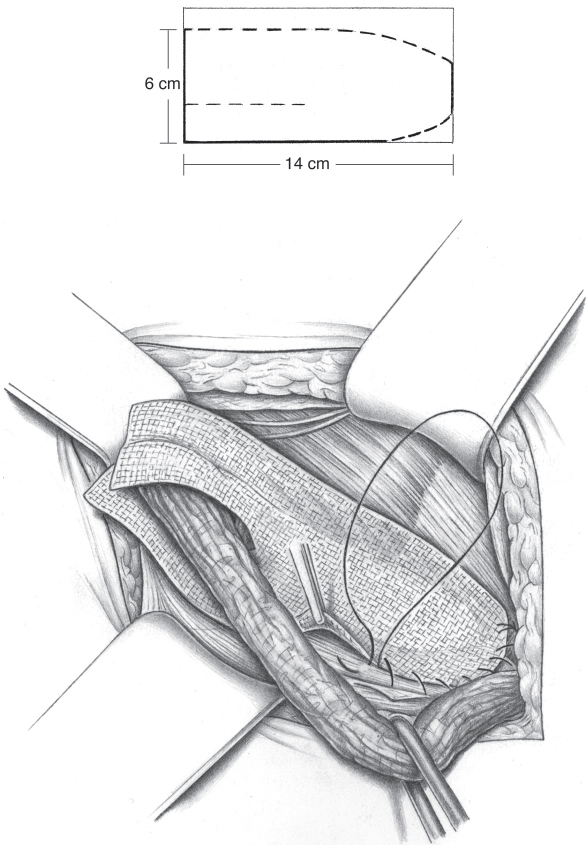
Fig. 2.57 Top: Mesh cutting pattern. Bottom: after trimming the mesh, it is fixed to the inguinal ligament with a continuous suture.