■ CT scanning of the chest is not routine for the workup of that early-stage breast cancer. However, if a CT scan of the chest or positron emission tomography (PET)-CT is performed for other indications, internal mammary node enlargement may be identified (FIG 2A,B). If the patient has palpable fullness in the parasternal region, a CT scan should be ordered to evaluate for internal mammary nodal metastases.

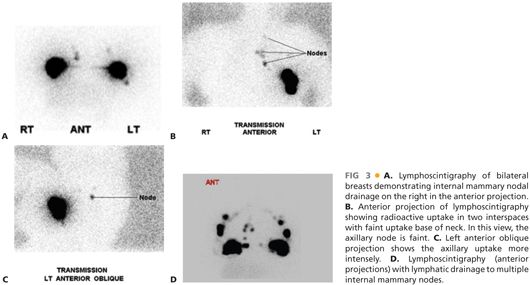
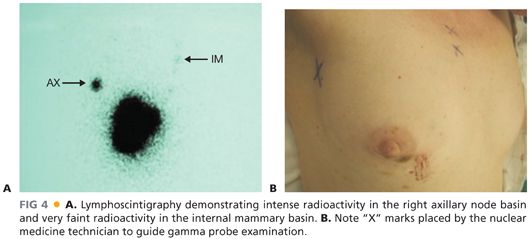
■ In order to identify the internal mammary nodal drainage in the sentinel node procedure, it is critical to inject a radiolabeled tracer for mapping of the pathways to the internal mammary nodes. To maximize the chance of identifying internal mammary lymphatic drainage, it is important to perform the injections of technetium sulfur colloid in the peritumoral region rather than performing a subareolar injection only. Lymphoscintigraphy can be performed to have a visual representation of the location of the internal mammary drainage (FIG 3A–D). The area of radioactivity in the parasternal region can be marked on the skin by the nuclear medicine technician at the time of scanning (FIG 4A,B). This increases the efficiency of identifying the appropriate interspace for exploration for the sentinel node. Most commonly, there will be one interspace that demonstrates a hot spot. However, more than one interspace may demonstrate a radioactive focus. The most common areas of drainage are the 2nd and 3rd interspaces.
SURGICAL MANAGEMENT
Preoperative Planning
■ The lymphoscintigraphy should be reviewed prior to going into the operating room. It is important to consent the patient specifically for the internal mammary exploration. Knowing from the lymphoscintigraphy that there is internal mammary lymphatic drainage, the surgeon can convey to the patient that this pathway can be pursued if the patient is agreeable. If it is the practice of the surgeon not to perform lymphoscintigraphy prior to surgery, then the interspaces can be examined intraoperatively with the gamma probe to identify foci of increased radioactivity in the parasternal interspaces. It remains important to consent the patient for the possibility of an internal mammary exploration with its potential complications.
Positioning
■ The patient is positioned supine with the arms abducted to 90 degrees on padded arm boards. The skin prep of the chest wall should cross to the contralateral breast so that the sternum and parasternal regions are draped into the field of operation.
TECHNIQUES
INCISION AND INITIAL IDENTIFICATION OF AREA OF INTERNAL MAMMARY SENTINEL NODE
■ Placement of the incision is governed by the procedure planned for resection of the breast tumor. For patients having breast-conserving surgery, the incision for the primary tumor is placed overlying the primary lesion. If the primary lesion is near to the area of internal mammary drainage, then it may be feasible to explore the interspaces via the partial mastectomy incision. However, if the primary lesion is distant from the parasternal region, then the incision for exploration of the interspace is placed overlying the area of focal radioactivity.
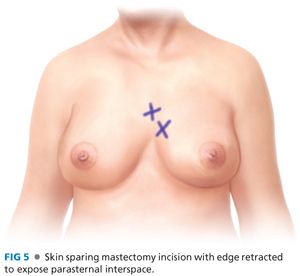
■ If the patient is undergoing a mastectomy, the standard mastectomy incision is used for accessing the parasternal interspaces (FIG 5). When reconstruction is planned, the mastectomy incision is generally more limited with the skin-sparing technique. However, the parasternal region can be generally accessed via these incisions with retraction of skin flaps, unless there is nipple preservation with the incision placed in the inframammary line. In this circumstance, the incision location would be determined in a similar fashion as patients having breast-conserving surgery.
■ It is much easier to identify the area of focal radioactivity in the interspaces after the breast is removed or after the partial mastectomy is completed. This reduces the amount of background radioactivity, which increases the ease of identifying radioactivity in an internal mammary node. In order to find an internal mammary sentinel node, it is imperative to have a strong signal that can be picked up by the gamma probe to direct the incision placement.
■ Lymphazurin blue, which is often injected for identification of the sentinel nodes in the axilla, should be injected prior to beginning any resective procedure in the operating room. Lymphazurin blue alone will not be successful in identifying the internal mammary sentinel nodes. However, once the area of radioactivity is identified and exploration is begun, blue lymphatics or staining of the sentinel nodes may be identified but not with the frequency that it is seen in the axillary nodes. As with the radioactive tracer, the blue dye is more likely to be identified in the internal mammary nodes if the injection is peritumoral.
■ After the blue dye is injected, the axillary sentinel node exploration is then begun. (Refer to Chapter 8 for more information on sentinel node dissection.) In most cases, there will be an axillary sentinel node identified in those patients who also have internal mammary drainage.
■ The mastectomy or partial mastectomy is then performed.
EXPLORATION OF THE PARASTERNAL INTERSPACES
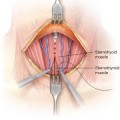
■ Using the gamma probe, the parasternal interspaces are examined in sequence from superior to inferior. In patients having a standard or skin-sparing mastectomy incision, the skin edges can be retracted with a Richardson retractor or with Lone Star hooks, which can obviate the need for an assistant to retract. With the pectoralis muscle exposed, the gamma probe is then placed directly on the muscle after palpating the interspace. When an area of focal radioactivity is identified, counts are taken for 10 seconds, two or three times with a background taken a centimeter away to confirm that it is a focal hot spot. Counts are taken at each interspace.
■
Related posts:
 Thyroidectomy for Substernal Goiters
Thyroidectomy for Substernal Goiters
 Inguinal Lymph Node Dissection (Inguinofemoral and Ilioinguinal) for Metastatic Melanoma
Inguinal Lymph Node Dissection (Inguinofemoral and Ilioinguinal) for Metastatic Melanoma
 Thyroid Lobectomy
Thyroid Lobectomy
 Pedicled Transverse Rectus Abdominis Myocutaneous Flap Breast Reconstruction
Pedicled Transverse Rectus Abdominis Myocutaneous Flap Breast Reconstruction
 Open Neck Exploration for Primary Hyperparathyroidism
Open Neck Exploration for Primary Hyperparathyroidism
 Subtotal Parathyroidectomy or Total with Autologous Graft
Subtotal Parathyroidectomy or Total with Autologous Graft
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


