CHAPTER 12 Internal Brow Lift: Browplasty and Browpexy
An internal brow lift offers the patient a method of raising the eyebrow without any additional incisions or scars; however, it is useful only for mild brow ptosis that is confined to the central and temporal aspect of the eyebrow. The technique does not lift the nasal brow, reduce excessive tissue above the nose, or treat overaction of the corrugator or procerus muscle. Nonetheless, I have been using this technique for several decades and find it invaluable in many cases.
There are some patients who have a unilateral brow ptosis that leads to asymmetric upper eyelid creases and folds (Fig. 12-1). In these patients, the internal brow lift not only makes the brows more symmetrical but also helps symmetry of the upper eyelid creases and folds.

The internal brow lift (browpexy) and excision of excessive brow fat (browplasty) are important adjunctive procedures in selected blepharoplasty patients.1–3
Anatomic considerations
The eyebrow and its surrounding soft tissues represent a specialized anatomic region of the face and the superficial sliding muscle plane of the forehead. Cadaveric studies by Lemke and Stasior4 have helped to define the brow-eyelid anatomic unit and its importance in repair of brow ptosis and dermatochalasis.
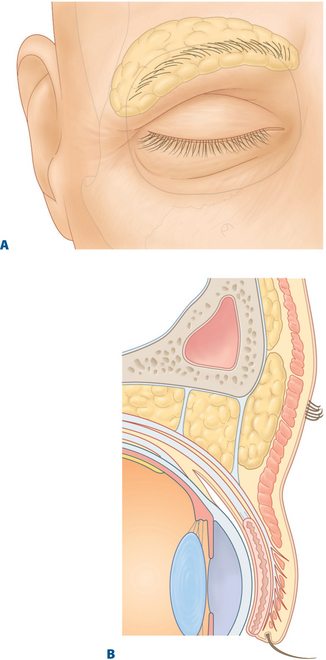
A fat pad exists beneath the eyebrow, from which dense attachments secure the brow to the supraorbital ridge. This fat pad enhances eyebrow motility, especially laterally, where it is most pronounced (Fig. 12-2A). The brow fat pad often extends inferiorly into the suborbicularis fascia-preseptal plane in the upper eyelid and can be mistaken for orbital fat by the novice blepharoplasty surgeon (Fig. 12-2B).
Indications
Although the coronal and endoscopic forehead lift procedures provide the most pronounced correction of forehead and glabella laxity, these techniques may be more extensive than the patient or surgeon desires. It should be emphasized that the internal browpexy procedure does not replace conventional brow lifts and should not be done in patients with severe brow ptosis (see Chapter 6).
I have also found the internal brow approach to be useful in lowering an abnormally high eyebrow that occurs from fixation of the brow to periosteum from trauma.5 In these cases the brow is sutured to the level of the superior orbital rim.
Surgical technique
Related posts:
 Upper Blepharoplasty Combined with Levator Aponeurosis Repair
Upper Blepharoplasty Combined with Levator Aponeurosis Repair
 Evaluation of the Cosmetic Oculoplastic Surgery Patient
Evaluation of the Cosmetic Oculoplastic Surgery Patient
 Brow Lift Techniques
Brow Lift Techniques
 Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
 Eyelid and Facial Laser Skin Resurfacing
Eyelid and Facial Laser Skin Resurfacing
 Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


