Severe zinc deficiency states, such as acrodermatitis enteropathica, are associated with a variety of skin manifestations, such as perioral, acral, and perineal dermatitis. These syndromes can be reversed with systemic zinc repletion. In addition to skin pathologies that are clearly zinc-dependent, many dermatologic conditions (eg, dandruff, acne, and diaper rash) have been associated and treated with zinc. Success rates for treatment with zinc vary greatly depending on the disease, mode of administration, and precise zinc preparation used. With the exception of systemic zinc deficiency states, there is little evidence that convincingly demonstrates the efficacy of zinc as a reliable first-line treatment for most dermatologic conditions. However, zinc may be considered as an adjunctive treatment modality. Further research is needed to establish the indications for zinc treatment in dermatology, optimal mode of zinc delivery, and best type of zinc compound to be used.
In 1869, Raulin described zinc as an essential component for Aspergillus niger . Since this observation, zinc was shown to be a cofactor for more than 300 metalloenzymes and 2000 transcription factors. Zinc is a vital prosthetic group in zinc/copper superoxide dismutase, thereby affecting cellular reduction/oxidation status. This metal is also putatively involved in gene transcription with factors possessing zinc-finger motifs and participates in histone deacetylase reactions. Overall, zinc has been recognized as crucial for the normal development and physiology of a variety of organisms, including humans. Zinc is found in all types of tissue. The skin contains approximately 6% of total body zinc and is second only to muscle and bone in zinc content. Foods that are rich in zinc include beef, oysters, and liver. Zinc is absorbed in the distal duodenum and proximal jejunum. Absorption of zinc by the intestine is inhibited by phytate, among other molecules. Zinc is primarily excreted through the intestine and to a lesser extent in urine. For more than 3000 years, zinc salts, such as zinc oxide or calamine, have been applied topically to facilitate wound healing. In the past 50 years, progress has been made to associate zinc with numerous skin pathologies. The roles of zinc in dermatology will be discussed later. Refer to Table 1 for a summary of skin conditions associated with zinc deficiency and the proposed modes of treatment, respectively.
| Disease | Mode | Efficacy | References | Study Design |
|---|---|---|---|---|
| Acne vulgaris | ||||
| … | Systemic | ++ | Hillstrom et al | Double-blind RCT a |
| … | Systemic | ++ | Göransson et al | Double-blind RCT |
| … | Systemic | ++ | Verma et al | Double-blind RCT |
| … | Systemic | ++ | Liden et al | Double-blind RCT |
| … | Systemic | − | Orris et al | Double-blind RCT |
| … | Systemic | + | Weimar et al | Double-blind RCT |
| … | Systemic | ++ | Dreno et al | Double-blind RCT |
| … | Systemic | − | Dreno et al | Double-blind RCT |
| … | Topical | − | Sharquie et al Sharquie et al | Single-blind RCT |
| … | Systemic | = | Michaelsson et al Michaelsson et al Michaelsson et al | Double-blind RCT |
| … | Topical | = | Feucht et al | Double-blind RCT |
| … | Topical | + | Habbema et al | Double-blind RCT |
| … | Topical | + | Schachner et al Schachner et al | Double-blind Randomized cross-over trial |
| … | Topical | + | Schachner et al Schachner et al | Double-blind RCT |
| … | Topical | − | Langner et al | Investigator-Blind RCT |
| … | Topical | = | Cunliffe et al | Investigator-blind RCT |
| … | Topical | + | Strauss & Stranieri | Double-blind RCT |
| … | Topical | = | Bojar et al | Double-blind RCT |
| … | Topical | + | Pierard-Franchimont et al | Double-blind RCT |
| Aphthous ulcers/mucositis | ||||
| … | Systemic | + | Sharquie et al Sharquie et al | Double-blind RCT |
| Diaper dermatitis | ||||
| … | Topical | − | Arad et al | Observation |
| … | Topical | − | Wananukul et al | Investigator-blind RCT |
| Eczema | ||||
| … | Topical | + | Faghihi et al | Double-blind RCT |
| Seborrheic dermatitis and dandruff | ||||
| … | Topical | + | Marks et al | Parallel observation |
| … | Topical | − | Pierard-Franchimont et al | Randomized, parallel observation |
| … | Topical | + | Shin et al | Randomized |
| Androgenic alopecia | ||||
| … | Topical | + | Berger et al | Investigator-blind RCT |
| Recalcitrant viral warts | ||||
| … | Topical | + | Khattar et al | Double-blind RCT |
| Leprosy | ||||
| … | Topical | − | Reinar et al | RCT |
| Psoriasis | ||||
| … | Topical | = | Housman et al | Double-blind RCT |
| Rosacea | ||||
| … | Systemic | + | Sharquie et al Sharquie et al | Double-blind RCT |
| Chronic cutaneous ulcers | ||||
| … | Topical | + | Brandrup et al | Randomized trial |
| … | Topical | + | Stromberg et al | Double-blind |
| … | Topical | = | Agren et al | Single-blind RCT |
| … | Topical | + | Apelqvist et al | Open RCT |
Methods
In 2005, the authors conducted a PubMed search using zinc and the dermatosis in question as search words. Literature beyond the scope of the authors’ initial search was added for background purposes and to compliment their results. The results of this review were previously published. In September 2009, the authors repeated this method searching articles written since 2005, in addition to the previous search.
Results
Dermatologic Diseases Attributed to Systemic Zinc Abnormalities
Three separate major entities involving systemic zinc deficiency have been described to date.
Moderate systemic zinc deficiency
In 1961, Prasad and colleagues described several series of subjects from the Mediterranean suffering from growth retardation, male hypogonadism appearing in adolescence, cell-mediated immune dysfunctions, abnormal neurosensory changes, rough and dry skin, and delayed wound healing. This syndrome was attributed to inadequate dietary zinc intake or disruption of its absorption by other molecules in the intestine (eg, phytate), resulting in moderate zinc deficiency. When treated with dietary zinc supplementation, these subjects greatly improved.
Acrodermatitis enteropathica
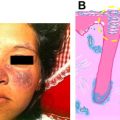
Acrodermatitis enteropathica, also known as Danbolt-Closs syndrome, is an autosomal recessive condition initially reported by Danbolt and Closs in 1942. Acrodermatitis enteropathica is characterized by gastrointestinal disturbances, eye infections, growth failure, vesiculobullous, and psoriasiform dermatitis. These skin lesions are distributed in the perioral, acral and perineal areas in a symmetric pattern ( Fig. 1 ). In 1973, Barnes and Moynahan noted the association between the acrodermatitis enteropathica phenotype and severe zinc deficiency. Consequently, acrodermatitis enteropathica was successfully treated by supplementation of dietary zinc. Recently, mutations in the SLC39A4 gene, encoding a zinc transporter protein (hZIP4) were identified to be responsible for the acrodermatitis enteropathica phenotype by impeding zinc absorption in the intestinal tract. In addition to congenital acrodermatitis enteropathica, an acquired class of syndromes with a similar phenotype was described.
Acute zinc deficiency
With the advances in intensive care made in the latter half of the 20th century, an acute form of zinc deficiency was identified. This condition is associated with parenteral alimentation. The hallmarks of acute zinc deficiency are diarrhea; mental apathy; depression; alopecia; and acute dermatitis (more pronounced in the perioral region). This syndrome is usually reversible with appropriate zinc supplementation. Severe to moderate zinc deficiency is increasingly rare, especially in developed countries; however, one should be alert to the possibility of zinc deficiency as a differential diagnosis, especially in intensive care-associated dermatoses.
The states mentioned earlier are closely linked to systemic zinc depletion. Beyond these conditions, many dermatologic diseases are associated and treated with topical or systemic zinc preparations with varying degrees of success. As a general note, with the exception of systemic zinc deficiency states, this trace element is not currently used as a first-line dermatologic treatment. The following discussion will explore skin conditions for which zinc was postulated to carry a therapeutic effect and the efforts made to investigate the role of zinc in those dermatoses.
Utility of Zinc in General Dermatology
Acneiform dermatoses
Acne vulgaris
The initial link between zinc deficiency and acne was made as early as the 1970s by Michaelsson and Fitzherbert who reported the improvement of acne upon supplementation of zinc in zinc-deficient patients. Michaelsson first noted the favorable effects of zinc on acne in a patient suffering from acrodermatitis enteropathica. Subsequently, serum levels of zinc surveyed in patients suffering from severe inflammatory acne vulgaris were found to be significantly lower than normal. Following these observations, several double-blinded, randomized controlled trials (RCT) reported oral zinc sulfate to be effective in the treatment of severe acne and less efficient for the treatment of mild to moderate acne. Nausea, vomiting, and diarrhea were noted as side effects with this mode of treatment and may have lead to low compliance. Orally administered zinc gluconate was also found to be effective in treating inflammatory acne with no additional benefit for an initial loading dose. When compared with systemic tetracycline treatment in a multicenter, double-blinded randomized trial, zinc salts appear to be equal to or less effective than this class of antibiotics and are not considered first-line treatment for this condition.
Sharquie and colleagues evaluated the effectiveness of 2% tea lotion in comparison with topical 5% zinc sulfate solution in the treatment of acne vulgaris. In a single-blind, randomized study of 47 subjects with mild acne, the 5% zinc sulfate solution was shown to be beneficial, but did not reach statistically significance, whereas the tea lotion did. Topically applied preparations containing zinc salts (ie, zinc acetate, zinc octoate) with or without erythromycin were either equal to or superior to a single antibiotic (ie, erythromycin, tetracycline, or clindamycin) in reducing the severity of acne and the number of lesions in some studies. However, a study by Langner and colleagues found that the onset of action of clindamycin phosphate plus benzoyl peroxide once daily was quicker than twice daily erythromycin plus zinc acetate and there was no overall difference in efficacy or adverse events. Conversely, topical zinc sulfate was found to be ineffective in the treatment of acne and caused considerable local irritation. The differences between the two salts may be caused by different absorption rates and solubility. A recent study of 24 subjects with mild to moderate acne demonstrated that the systemic absorption of clindamycin in subjects using a combined topical zinc/clindamycin 1% gel was 30% to 50% less than in subjects using a clindamycin lotion alone. No differences in efficacy were noted leading the investigators to believe that this inhibitory effect of systemic absorption may lead to improved compliance. To further improve compliance, it was observed that subjects using zinc in combination with clindamycin once daily or twice daily compared with clindamycin lotion alone led to equivalent efficacy and safety.
From a mechanistic point of view, the role of zinc in the treatment of acne vulgaris is not well understood. Several studies noted a reduction in local skin microbial parameters such as the Propionibacterium acnes count and free fatty acids levels. Zinc appears to target P acnes specifically and does not affect Staphylococcus sp. Whether zinc is effective against Micrococcaceae has yet to be determined because existing data are controversial. A possible mechanism for this antimicrobial effect is inhibition of P acnes lipase by zinc. Treatment with zinc gluconate improved polymorphonuclear chemotaxis in subjects suffering from acne. This finding suggests a role for zinc as an inflammation modulating agent in skin. An additional proposed mechanism for the benefit of zinc in the treatment of acne is suppression of sebum delivery, perhaps by anti-androgenic activity. Zinc appears to enhance the topical absorption of erythromycin. This observation alludes to a possible benefit in combining erythromycin with zinc salts. In summary, zinc is thought to be linked to acne through direct effects on the microbial-inflammatory equilibrium, and possible facilitation of topical antibiotic absorption in combined zinc preparations. Regardless, these studies provide evidence that zinc may be regarded as a second-line treatment that could be considered especially in patient groups in which first-line treatments for acne may be contraindicated, such as pregnant women, or poorly tolerated, minimizing the concern of side effects.
Rosacea
Rosacea is typically treated with topical and systemic therapies, such as antibiotics, metronidazole, retinoids, topical antifungals, azelaic acid, tacrolimus, and others. In a double-blind, placebo-controlled crossover trial, 25 subjects were treated with 100 mg of zinc sulfate three times daily. A statistically significant improvement was demonstrated after 1 month of therapy. Thus, zinc sulfate is thought to have therapeutic and prophylactic effects in rosacea. The mechanisms of action in rosacea are unknown and are postulated to be mediated through effects on oxidative status, antiinflammatory properties, and targeting various organisms implicated in rosacea. Alternatively, zinc may be beneficial in rosacea acting as a modulator of inflammation.
Hidradenitis suppurativa
No standard of therapy exists for hidradenitis suppurativa. Many therapies including local antiseptics, antibiotics, long-term antibiotic therapy, isotretinoin, oral contraceptives, anti-androgens, corticosteroids, and surgery have been used. In an investigation of 22 subjects with grade I or II in Hurley’s classification, 90 mg of zinc gluconate was administered for 4 months. All subjects were noted to have a clinical response with eight complete remissions and 14 partial remissions. Also, recurrences disappeared when the dose of zinc salts was increased. Thus, this treatment appears to be suppressive rather than curative.
Folliculitis decalvans
Folliculitis decalvans is a chronic inflammatory condition of the scalp, commonly leading to scarring alopecia. Care is focused on antibiotic usage in patients with folliculitis decalvans and in severe cases steroids have been effective. Abeck reported three subjects responding to a combination therapy consisting of oral and topical fusidic acid 1000 mg daily for 3 weeks and 1.5% cream for 2 weeks respectively and a 6 month course of oral zinc sulfate 400 mg daily. After 1 year, two subjects had no evidence of folliculitis decalvans, whereas another subject had a recurrence after a 2-month disease-free period when zinc therapy was stopped. Abeck attributes the antiinflammatory effect to zinc sulfate.
Vasculitic conditions
Behcet’s disease
Behcet’s disease (BD) is a vasculitic syndrome presenting as oral aphthous ulcers; genital ulcers; ocular lesions; skin lesions, such as pustules and erythema nodosum; and a positive pathergy test. Conventionally, immunosuppressants and antiinflammatory drugs are used to control the symptoms of BD. Najim and colleagues studied 76 subjects with BD who showed increased levels of serum malondialdehyde and copper while glutathione and zinc levels were decreased ( P <.05). Furthermore, zinc levels were found to be inversely correlated with the clinical manifestation index and pathergy test positivity grades ( P <.01). In a randomized, controlled, double-blind cross-over trial of 30 subjects treated with 100 mg zinc sulfate or identical placebo tablet three times daily, a statistically significant difference was observed in the clinical manifestation index. In addition, mean serum zinc level in patients with BD was significantly lower than mean serum zinc levels in the control group. The investigators attribute the antioxidant and immunomodulatory effects of zinc sulfate to effectively treating patients with BD.
Conditions affecting hair
Androgenic alopecia
Treatment of androgenic alopecia with topical zinc pyrithione resulted in a modest, though sustained increase in hair growth. In a 6-month, randomized, investigator-blinded, parallel-group clinical study, the efficacy of a 1% pyrithione zinc shampoo was compared with that of a 5% minoxidil topical solution, a placebo shampoo, and a combination of 1% pyrithione zinc shampoo and 5% minoxidil topical solution. The 1% pyrithione zinc shampoo group showed a relative increase in hair count that was less than half that for the topical minoxidil. There was no advantage seen in using combined solution, perhaps indicating a joint pathway of action.
Telogen effluvium
Zinc serum concentrations and the efficacy of zinc supplementation were tested in women with chronic telogen effluvium, which was traditionally linked with zinc deficiency. Low levels of zinc were detected in only 7% of the women in this study. Moreover, treatment of subjects who were supposedly zinc deficient with the essential amino acid L-lysine resulted in the achievement of normal serum zinc levels with the exception of one subject. Thus, zinc deficiency is most likely not associated with telogen effluvium.
Seborrheic dermatitis and dandruff
Seborrheic dermatitis (SD) and dandruff are traditionally treated with topical zinc pyrithione-containing preparations (eg, shampoo). Pyrithione is a zinc ionophore putatively facilitating local absorption of zinc. The stratum corneum of scalp samples taken from subjects with dandruff showed remarkable improvement after treatment with zinc pyrithione. Zinc pyrithione has been proposed to exert its effects through inhibition of keratinocyte proliferation ; however, in vivo studies fail to substantiate this claim. It is currently thought that in the case of dandruff and SD, the beneficial effects of zinc pyrithione are caused by direct inhibition of the growth of Malassezia sp. Clinically, several randomized controlled trials reported significant efficacy for zinc pyrithione in the treatment of dandruff and SD. However, in an open, randomized trial, 331 subjects were assigned to using a ketoconazole 2% or a zinc pyrithione 1% shampoo for 4 weeks twice weekly. Ketoconazole treatment resulted in a significantly greater improvement in the total dandruff severity score than zinc pyrithione ( P <.02). In addition, the recurrence rate of dandruff was significantly lower in the ketoconazole group when compared with zinc pyrithione. Another randomized trial by Shin and colleagues showed subjects using conventional treatment of zinc pyrithione improved continuously even after cessation of treatment, in contrast with betamethasone or tacrolimus therapy, and suggest zinc pyrithione be used in a combination with a topical steroid to improve results.
Dermatitis
Eczema
Hand Eczema is usually managed with emollients, barrier creams, corticosteroids, calcineurin inhibitors, immunosuppressants, and antimicrobial agents. The addition of 2.5% zinc sulfate to 0.05% clobetasol cream twice a daily for two weeks was more effective than Clobetasol 0.05% cream alone ( P <.05) in a study of 47 patients with chronic hand eczema. In addition, the recurrence rate of eczema was significantly lower in the group treated with this combination treatment ( P <.05). Multiple mechanisms of action of zinc were proposed, including anti-inflammatory effects, promotion of wound repair, etc.
Diaper dermatitis
Diaper rash is traditionally treated with topical zinc preparations. A recent report shows clinical efficacy for zinc oxide in the reduction of the inflammatory parameters of diaper dermatitis. Arad and colleagues investigated 54 infants with diaper dermatitis and randomly assigned each subject to one of three treatment groups including zinc oxide paste, clobetasone butyrate 0.05%, and aqueous solution of eosin 2%. After 5 days of treatment, the rate of complete healing in the eosin group was significantly higher than that in the zinc oxide paste and corticosteroid groups ( P = .048). In addition, partial healing was higher in the eosin group than in the other groups ( P = .021). A similar study in Thailand evaluating irritant diaper dermatitis from diarrhea demonstrated transepidermal water loss to be less on the side treated with 5% dexpanthenol and zinc oxide ointment (vs ointment base), but no statistical significance in the severity of the rash.
Infectious disease
Recalcitrant viral warts
Al-Gurairi and colleagues reported a cure rate of more than 80% of recalcitrant viral warts with oral zinc sulfate. However, this is a preliminary study, which merits additional research. In a randomized, placebo-controlled, double-blind study, Sadighha treated 13 subjects with oral zinc sulfate (10 mg/kg to a maximum dose of 600 mg/day) for 1 to 2 months, with a 54% response rate within the first month of treatment. Serum zinc levels were also studied in those subjects. The mean value of zinc in the subjects’ sera was 53.3 ± 9.7 μg/dl before the study and 181.5 ± 22.1 μg/dl in those who responded, whereas the mean level of serum zinc after 1 month of treatment in those who did not respond to treatment reached 69 ± 10.11 μg/dl. Some of the remaining subjects who had originally not responded within the first month eventually responded and were found to have mean serum zinc levels of 201.3 ± 22.0 μg/dl, whereas in the rest of the non-responders, the mean serum zinc levels were 69.8 ± 10.3 μg/dl. After a course of 2 months’ treatment with zinc sulfate, the success rate rose to 76.9% (10 subjects). This study demonstrates a dose-dependent response in subjects with recalcitrant warts treated with zinc. Yaghoobi conducted a similar study in 32 subjects with an oral dosage of 10 mg/kg zinc sulfate and found that elevated serum zinc levels corresponded with successful treatment of verrucae.
In a small subject population (n = 10), Sharquie looked into the use of 10% topical zinc sulfate solution three times daily for 4 weeks and found a full response in 80% for plane warts in a pilot trial and 86% in a double-blind trial without recurrence 2 to 6 months afterwards. Common warts responded in only 11%. A similar randomized, double-blind controlled trial of 44 subjects with treatment of topical zinc oxide 20% ointment or salicylic acid 15% + lactic acid 15% ointment twice daily was conducted for 3 months or until cure occurred. In the zinc oxide-treated group, 50% of the subjects showed complete cure and 19% failed to respond, compared with 42% and 26%, respectively, in the salicylic acid-lactic acid-treated group. Zinc is thought to have worked through an unspecified upregulation of immunologic events.
Old-world cutaneous leishmaniasis
Several groups assessed the efficacy of zinc sulfate for the treatment of acute old-world cutaneous leishmaniasis by systemic preparations and intralesional injections. Iraji’s double-blinded, case-controlled clinical study included 35 subjects receiving intralesional meglumine antimoniate (MA) and 31 subjects receiving intralesional zinc sulfate. A greater cure rate was reported for zinc sulfate (84%) than for MA (60%). After 2 and 4 weeks, treatment efficacy with zinc sulfate was higher than that with MA ( P <.01), but after 6 weeks, there was no significant difference between the two groups ( P >.05). Oral zinc sulfate given at 10 mg/kg divided into three daily doses appeared to be effective in eradicating cutaneous leishmaniasis. This effect was associated with increments in serum zinc levels. Studies where different doses of zinc sulfate are given show that subjects receiving 10 mg/kg versus 2.5 or 5 have higher response rates, although the difference was not statistically significant. The efficacy of intralesional zinc sulfate in cutaneous leishmaniasis is reportedly high, though its advantage over meglumine antimoniate remains controversial.
Miscellaneous conditions
Necrolytic acral erythema
Necrolytic acral erythema (NAE) is a cutaneous marker of hepatitis C virus (HCV) infection classified within a group of diseases known as necrolytic erythemas. Necrolytic erythema is linked to nutrient deficiencies and includes necrolytic migratory erythema, acrodermatitis enteropathica, pellagra, and essential fatty acid deficiencies. However, in most reported cases of NAE there is an absence of nutrient deficiency. Nofal observed five subjects with NAE, two of whom had low serum zinc and albumin levels. All subjects responded to oral zinc sulfate, whereas mild or no improvement was seen with oral amino acid supplementation. In addition, DeCarvalho described a case of NAE with a zinc deficiency in Brazil, which responded to oral zinc sulfate 210 mg twice daily with complete resolution over 7 weeks.
Case reports by Khanna and Abdallah both describe subjects with HCV and NAE with normal serum zinc treated successfully with oral zinc at 220 mg daily. Khanna, however, also treated the subject with interferon alpha-2b injections in addition to zinc. Many explanations exist for zinc’s role in cases where serum zinc levels are normal. Geria suggests that because albumin is the main carrier of zinc and essential fatty acids in plasma, decreased serum albumin levels may cause transitory deficiency in one or more of these nutrients, which could play a role in the development of NAE. Furthermore, decreased serum zinc levels may be a late indicator of zinc deficiency. Thus, skin manifestations of zinc deficiency may occur despite having serum zinc levels within reference range.
Psoriasis
Zinc was linked to psoriasis by a chain of case reports on the beneficial effects of locally applied zinc pyrithione-containing preparations on psoriatic plaques. However, in a well-planned controlled study of 24 subjects, topical zinc pyrithione was ineffective when compared with topical clobetasol propionate in the treatment of psoriasis. Furthermore, no additive effects were noted when combining zinc-pyrithione with clobetasol propionate. Systemic zinc sulfate supplementation was also ineffective as compared with placebo in the treatment of psoriasis. The authors conclude that, based on currently available data, zinc has no apparent role in the treatment of psoriasis.
Chronic cutaneous ulcers
Patients suffering from chronic skin ulcers have low skin and serum levels of zinc. In addition, zinc deficiency may be caused by excessive wound drainage. Ackerman and colleagues noted an altered zinc distribution in the skin of subjects with varicose ulcers. Topical preparations containing zinc oxide were effective in the treatment of arterial and venous leg ulcers, pressure ulcers, and necrotic diabetic foot ulcers. The therapeutic effects of zinc oxide or zinc sulfate on leg ulcers were most pronounced in subjects who were zinc-deficient. Zinc oxide was superior to zinc sulfate because the latter was not as effective and caused local irritation at high concentrations (see the earlier discussion of acne vulgaris). The use of oral zinc (zinc sulfate) for chronic leg ulcers remains controversial and may be of benefit in patients who are zinc deficient. Few studies have demonstrated a response to oral supplements including zinc; however, the exact cause of improvement is difficult to ascertain because many supplements are used at once. The therapeutic effects of zinc in chronic cutaneous ulcers are thought to be derived from its ability to enhance reepithelialization, decrease inflammation, and inhibit bacterial growth.
Local zinc deficiency
A poorly understood concept is local zinc deficiency (ie, low levels of tissue zinc with normal serum levels). Michaelsson and colleagues reported a lack of correlation between skin and serum zinc levels among healthy subjects. When zinc levels were surveyed in subjects with dermatitis herpetiformis, acne, psoriasis, and Darier disease, they were lower than normal. However, there was no association between serum and skin zinc levels, because many subjects had normal serum zinc. This finding may indicate tissue zinc depletion as contributing to disease etiology. Another plausible explanation is that serum zinc levels do not reflect total zinc capacity. Amer and colleagues reported a significantly lower serum zinc level in subjects with severe acne. Perhaps a more extensive examination of skin and serum levels corrected to the severity of the condition in question will yield a more significant correlation in the future.
Melasma
This pigmentation deposition usually occurs in association with elevated levels of hormones during pregnancy or from oral contraceptives, and is treated with topical bleaching agents, chemical peels, lasers, and sun avoidance. Bolanca and colleagues suggested sunscreens containing physical blockers, such as titanium dioxide and zinc oxide, are preferred over chemical blockers because of their broader protection. In addition to sunscreen containing zinc, Sharquie treated 28 subjects with 10% zinc sulfate solution twice daily for 2 months and found a statistically significant difference with its use. Sharquie postulated that zinc aids in melasma by its peeling, antioxidant, and sun-screening effects.
Related posts:
 Innovative Management of Recurrent Furunculosis
Innovative Management of Recurrent Furunculosis
 Innovative Management of Lupus Erythematosus
Innovative Management of Lupus Erythematosus
 Innovative Therapy of Cutaneous T-Cell Lymphoma: Beyond Psoralen and Ultraviolet Light and Nitrogen Mustard
Innovative Uses of Rituximab in Dermatology
Innovative Uses of Tumor Necrosis Factor α Inhibitors
Innovative Uses of Thalidomide
Innovative Therapy of Cutaneous T-Cell Lymphoma: Beyond Psoralen and Ultraviolet Light and Nitrogen Mustard
Innovative Uses of Rituximab in Dermatology
Innovative Uses of Tumor Necrosis Factor α Inhibitors
Innovative Uses of Thalidomide
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


