This article focuses on the management of discoid lupus erythematosus, subacute cutaneous lupus erythematosus, and systemic lupus erythematosus when the usual therapeutic arsenal such as oral antimalarial drugs and topical/oral steroids fail or provide insufficient treatment efficacy. Many of the treatments listed are the same or similar to each other because of similarities in the pathogenesis of various subtypes of cutaneous lupus. The clinical challenge is to determine the indications for topical versus systemic therapy, and to also identify the scenarios when combined therapy is necessary.
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease that may affect any tissue or organ system, but most often involves the skin and joints. SLE affects women much more commonly than men (9:1), with a lifetime prevalence of 25 to 64 cases per 100,000 people, mainly among people of Afro-Caribbean origin. Its clinical course is episodic, and can range from an indolent cutaneous disease with occasional flares to a fulminant systemic course with significant mortality. Furthermore, primary dermatologic lupus may herald the progression of the indolent cutaneous manifestation to systemic internal disease. Many important topical and systemic therapies have been developed recently to better manage this life-threatening disease.
No specific genetic cause for SLE has heretofore been identified; however, multiple large demographic studies have highlighted genetic, racial, hormonal, and environmental factors associated with this disorder. Given multiorgan involvement, the diagnosis of SLE rests on the recognition of the relationship of disparate features. There are 11 criteria from the American College of Rheumatology (ACR) for the diagnosis of SLE and 3 of these are cutaneous lesions: malar rash, photosensitivity, and discoid rash ( Table 1 ).
| Malar rash | Fixed erythema, flat or raised, over the malar eminences, tending to spare the nasolabial folds |
| Discoid rash | Erythematous raised patches with adherent keratotic scaling and follicular plugging; atrophic scarring may occur in older lesions |
| Photosensitivity | Skin rash as a result of unusual reaction to sunlight by patient history or physician observation |
| Oral ulcers | Oral or nasopharyngeal ulceration, usually painless, observed by physician |
| Arthritis | Nonerosive arthritis involving 2 or more peripheral joints, characterized by tenderness, swelling or effusion |
| Serositis |
|
| Renal disorder |
|
| Neurologic disorder |
|
| Hematologic disorder |
|
| Immunologic disorder |
|
| Antinuclear antibody | An abnormal titer of antinuclear antibody by immunofluorescence (or an equivalent assay) at any point in time and in the absence of drugs known to be associated with “drug-induced lupus” syndrome |
a The proposed classification is based on 11 criteria. For the purpose of identifying study patients for clinical studies of systemic lupus erythematosus if any 4 or more of the 11 criteria are present, serially or simultaneously, during any interval of observation.
Cutaneous involvement occurs in 90% of patients with SLE. A new system that standardizes disease scoring in cutaneous lupus has been spearheaded by Dr Victoria Werth. This system is similar to the Psoriasis Area Severity Index (PASI) and is called the Cutaneous Lupus Erythematosus Disease Area and Severity Index (CLASI). This system scores skin damage and disease activity separately, thereby enabling investigators to standardize assessment of therapeutic response ( Table 2 ).
| CLASI (Cutaneous Lupus Erythematosus Disease Area and Severity Index) | |
|---|---|
| Activity | Damage |
| -Erythema | -Dyspigmentation |
| -Scale/Hypertrophy | -Scarring |
| -Nonscarring alopecia | -Scarring alopecia |
The cutaneous presentation of lupus can be divided into 3 distinct groups:
- 1.
Lupus erythematosus (LE) specific skin lesions
- •
acute cutaneous LE (ACLE) or “Butterfly rash”
- •
subacute cutaneous LE (SCLE)
- •
chronic cutaneous LE (CCLE) or discoid LE (DLE)
- •
LE panniculitis and LE tumidus
- •
- 2.
LE nonspecific skin disease: vasculitis, urticaria, and livedo reticularis
- 3.
Cutaneous complications of drug therapy for LE.
This article focuses on the management of DLE, SCLE, and SLE when the usual therapeutic arsenal such as oral antimalarial drugs and topical/oral steroids fail or provide insufficient treatment efficacy ( Table 3 ). Many of the treatments listed are the same or similar to each other because of similarities in the pathogenesis of various subtypes of cutaneous lupus. The clinical challenge is to determine the indications for topical versus systemic therapy, and to also identify the scenarios when combined therapy is necessary.
| Discoid Lupus Erythematosus | Subacute Cutaneous Lupus Erythematosus | Systemic Lupus Erythematosus | |
|---|---|---|---|
| Topical: | Pimecrolimus, tacrolimus, R-salbutamol | Sunscreens—anti UVA and UVB, pimecrolimus, tacrolimus | Pimecrolimus, tacrolimus |
| Systemic: | Hydroxychloroquine, chloroquine, quinacrine, lenalidomide, abatacept, efalizumab, a | Hydroxychloroquine, thalidomide, leflunomide, mycophenolate mofetil, intravenous immunoglobulin, efalizumab, a rituximab calcipotriene | Vitamin D supplementation Cyclophosphamide + azathioprine, intravenous immunoglobulin, mycophenolate mofetil, rituximab, belimumab, abatacept, epratuzumab |
| Other: | Pulse dye laser | Intralesional triamcinolone |
For more information on current clinical trials and innovative ideas we refer you to the following Web site sponsored by the National Institutes of Health: http://ClinicalTrials.gov . ClinicalTrials.gov is a registry of federally and privately supported clinical trials conducted in the United States and around the world. http://ClinicalTrials.gov gives information about a trial’s purpose, who may participate, locations, and contact numbers.
DLE
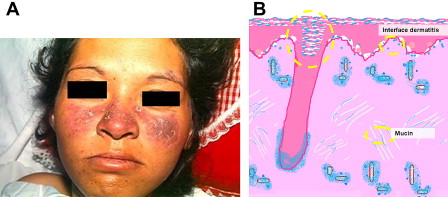
DLE is the most common manifestation of chronic cutaneous LE, and is characterized by single or multiple persistent, well-defined plaques with hyperkeratosis, scaling, telangiectasia, atrophy, scarring, follicular plugging, and peripheral hyperpigmentation with central hypopigmentation ( Fig. 1 A). Fig. 1 B shows illustration of histopathology demonstrating follicular plugging. Female/male ratio is 3:1. Localized involvement of the head and scalp accounts for 70% of DLE, whereas the disseminated form involves the chest, upper back, and extensor surfaces of the arms. High-titer antinuclear antibodies (ANAs) occur in 5% of patients, but generally no anti-double-stranded DNA (anti-dsDNA) antibodies are present. It is associated with photosensitivity in 50% of cases, and a small minority of patients (<5%) eventually develop SLE. Largely because of its chronicity and cosmetic sequelae, DLE severely affects quality of life.
Current treatment options include topical and systemic glucocorticoids, sunscreens, antimalarials, retinoids, dapsone, thalidomide, methotrexate, azathioprine, immunoglobulins, and cyclophosphamide. In a Cochrane database review, treatment of DLE with topical 0.05% fluocinonide was more effective than the use of 1% hydrocortisone. Likewise, a comparison between the use of acitretin and hydroxychloroquine showed no significant differences in treatment efficacy. Nevertheless, treatment-related adverse effects were more frequent and severe with acitretin. The review concluded that there was not enough reliable evidence to support the use of other drugs that are commonly used to treat DLE such as azathioprine, chloroquine, clofazamine, dapsone, gold, interferon alpha-2a, methotrexate, phenytoin, retinoids, sulphasalazine, thalidomide, topical calcineurin blockers, and biologic agents. Despite the paucity of high-quality evidence, some of these interventions have become commonplace and will be reviewed herein.
New therapies for DLE
Topical Calcineurin Inhibitors
Licensed for the treatment of moderate and severe atopic dermatitis in children and adults, topical calcineurin inhibitors are effective and have fewer severe side effects than topical steroids. The most frequent adverse events are irritation, burning, and erythema.
Pimecrolimus
This topical calcineurin inhibitor is an immunomodulator closely related to tacrolimus. Both inhibit T-cell proliferation and the production and release of proinflammatory cytokines such as interleukin-2 (IL-2), IL-4, and tumor necrosis factor-alpha (TNF-alpha). In contrast to tacrolimus, pimecrolimus has no effect on dendritic cells. Pimecrolimus does not induce skin atrophy or telangectasias because it does not affect endothelial cells and fibroblasts. It has comparable efficacy to betamethasone valerate. The use of pimecrolimus has correlated well with an improved quality of life in a number of studies.
Pimecrolimus is not approved by the Food and Drug Administration (FDA) for DLE.
Tacrolimus
Tacrolimus is a calcineurin inhibitor that may be used topically to block cutaneous T-cell activation. Skin infiltrating T lymphocytes play a major role in CCLE (DLE). Many small studies and case reports have established both the efficacy and safety of tacrolimus in the treatment of DLE. It has an advantage in safety over clobetasol concerning the development of skin telangiectasias. Additionally, one small study showed that tacrolimus compounded in clobetasol ointment was more effective than tacrolimus ointment or clobetasol ointment alone for the treatment of cutaneous lupus erythematosus.
Tacrolimus is not FDA approved for DLE.
R-salbutamol
R-salbutamol sulfate, a topical anti-inflammatory preparation, was tested successfully on patients with treatment-resistant DLE. An R-enantiomer of salbutamol, formulated as a cream for topical treatment of cutaneous lupus, it holds promising therapeutic potential in cutaneous lupus treatment (DLE). A double-blinded, randomized controlled trial of 37 patients with DLE showed significant improvement on scaling/hypertrophy, induration, pain, and itching. It was found to be safe and well tolerated.
Hydroxychloroquine, Chloroquine, and Quinacrine
Quinacrine (Qn), chloroquine (CQ), and hydroxychloroquine (HCQ) are antimalarial drugs routinely used to treat autoimmune diseases such as SLE and rheumatoid arthritis (RA). Their therapeutic impact on lupus treatment derives from their immunomodulating and photoprotective properties. A recent study on CQ showed a reduction of skin lesions via inhibition of angiogenesis. Qn leads to inhibition of neovascularization in mice during experimentally provoked inflammation, thereby impairing pathologic angiogenesis. The association of HCQ (dosage up to 5 mg/kg/d) and Qn (100 mg/d) appears to be safe and effective in DLE lesions when HCQ (200 mg twice a day or dosage up to 6.5 mg/kg/d) alone fails.
Lenalidomide
A thalidomide analog developed in the mid-1990s and FDA approved for multiple myeloma and myelodysplastic syndrome, lenalidomide is 2000-fold more potent than thalidomide in blocking the formation of TNF-alpha. Lenalidomide has fewer side effects (sedation, constipation, neuropathy, and teratogenicity) than its precursor thalidomide. Its most important side effects are myelosuppresion (neutropenia and thrombocytopenia) and an increased risk of deep venous thrombosis. In a recent report, 2 African American female patients were treated with low-dosage lenalidomide (5 mg/d), with 1 responding to treatment in the first month. This oral drug may be a good alternative for severe recalcitrant generalized DLE.
Abatacept
Abatacept is a fully human recombinant fusion protein that selectively modulates T-cell activation by blocking costimulation via the B7:CD28 pathway. This results in decreased T-cell activation, proliferation, cytokine secretion, and subsequent autoantibody production without depletion of T or B cells. It has effectively prevented SLE onset in several murine models. It has been used to treat lupus flares, mainly discoid lesions, pericarditis, and pluritis/pleurisy. Treatment consists of 4 monthly intravenous boluses of 10 mg/kg.
Efalizumab
Efalizumab is an anti-CD-11 monoclonal antibody, which is no longer available because of an association with the development of progressive multifocal leukoencephalopathy (PML) in 3 patients who took this drug over 3 years. It had been used to treat a small group of patients with DLE with good results. Usmani and Goodfield reported treatment success at 5.5 weeks among 12 of 13 patients treated with a weekly subcutaneous dosage of 1 mg/kg efalizumab. An additional report claimed almost complete remission in one 50-year-old male with DLE treated with subcutaneous efalizumab. Unfortunately, because of the possible etiologic association with progressive multifocal encephalopathy, this agent has been withdrawn from the American, Canadian, and European Union marketplaces.
Pulsed Dye Laser
Pulsed dye laser (PDL) is used for the treatment of benign skin lesions such as vascular lesions (eg, port wine stains, telangiectasias). PDL is considered to be the laser of choice for vascular lesions, because at wavelengths of 585 to 595 nm, the laser is known to produce excellent clinical results at minimal risk to patients. PDL is designed to deliver an intense but gentle burst of laser light to the skin. The light is absorbed by the erythrocytes, while leaving the surrounding tissue undamaged.
Treatment of DLE lesions with PDL was first described in 1999 by Raulin and colleagues. In a new study, 12 patients with active DLE demonstrated overall improvement when treated with the 585 nm PDL (fluence 5.5 J/cm 2 ) with a pulse duration of 0.45 milliseconds over a spot size diameter of 7 mm, and a treatment interval of 6 weeks. PDL may be effective and safe in cases of refractory DLE, and may be considered for the treatment of stable, solitary, active chronic DLE lesions when topical or systemic therapies have failed.
Related posts:
 Innovative Management of Recurrent Furunculosis
Innovative Management of Recurrent Furunculosis
 Innovative Therapy of Cutaneous T-Cell Lymphoma: Beyond Psoralen and Ultraviolet Light and Nitrogen Mustard
Biologic Drugs for the Treatment of Hidradenitis Suppurativa: An Evidence-Based Review
Innovative Uses of Tumor Necrosis Factor α Inhibitors
Innovative Uses of Thalidomide
Innovative Uses for Zinc in Dermatology
Innovative Therapy of Cutaneous T-Cell Lymphoma: Beyond Psoralen and Ultraviolet Light and Nitrogen Mustard
Biologic Drugs for the Treatment of Hidradenitis Suppurativa: An Evidence-Based Review
Innovative Uses of Tumor Necrosis Factor α Inhibitors
Innovative Uses of Thalidomide
Innovative Uses for Zinc in Dermatology
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


