Numerous arthropods can produce infestations, stings, and bites (see box). In addition to infestations, like scabies, arthropods can produce pruritic bites and local envenomation reactions that can result in tissue necrosis and ulceration. Moreover, some arthropods, such as ticks, mosquitoes, and flies, can be vectors of viral, rickettsial, bacterial, and protozoan infections that can cause skin disease or even systemic disease.
Insects
- •
Ants (see Chapters 6 and 12 )
- •
Bees
- •
Bedbugs (see Chapter 6 )
- •
Fleas (see Online Chapter)
- •
Flies (see Chapter 13 and Online Chapter)
- •
Mosquitoes
- •
Sandflies (see Chapter 36 )
- •
Wasps
- •
Yellowjackets
Arachnids
- •
Mites (see Chapters 6 and 12 )
- •
Scorpions
- •
Spiders (also see Chapter 14 )
- •
Ticks
Important History Questions
Did you see what bit or stung you?
For arthropods that cause skin injury, rather than an infestation, the answer to this question, in an observant and reliable patient, establishes the diagnosis. However, one must not be misled because there is tendency for patients to assume an exogenous explanation, such as a spider bite, when another disease process is actually the cause. For example, in one study of 600 skin injuries attributed to “spider bites” by patients, 20% ultimately had some other disease process at play.
Did you capture, kill, or photograph the “bug” that bit or stung you?
Patients only rarely bring in the arthropod, but increasingly patients have used smartphones to document the offending arthropod.
Does anyone else that you know have a similar problem?
An affirmative response favors some infestation. A child with head lice may have siblings, playmates, or classmates with a similar problem. Head lice can also be transmitted by shared hats, combs, hairbrushes, and other fomites. Scabies is another infestation that often affects multiple persons in a household.
Are you sexually active?
This question is important in the assessment of pubic louse and scabies infestations. The answer may be useful in establishing the diagnosis, but the answer is even more important in identifying others who require treatment. It is also important to realize that pubic louse infestations are not always sexually acquired, and the condition may be passed from those simply in close contact with an infested individual.
Does the lesion itch, or is it painful?
Most arthropod reactions are pruritic, but if pain is reported, this raises the possibility of a spider bite, reduviid bug bite, sting reaction (e.g., bees, wasps, yellowjackets, scorpions), or infected arthropod bite.
How do you feel?
Systemic symptoms are important in some severe envenomation reactions, such as those of the black widow spider, or with multiple bee stings, or in any bite causing anaphylaxis.
Important Physical Findings
What is the distribution of the lesions?
Some arthropod reactions are more likely to involve specific body regions. For example, head lice involve the scalp and upper neck, whereas pubic lice involve the genital areas or, rarely, the eyelashes. Tick bites often involve the scalp, neck, or intertriginous skin folds.
What does the bite site look like?
Spider bites often demonstrate two closely apposed fang marks, whereas other arthropod reactions cause red papules, often without a visible punctum. Skin necrosis should prompt consideration of brown recluse spider bite, particularly if the tissue damage is relentlessly expanding.
Pediculosis Capitis
ICD10 code B85.0
ARTHROPOD INFESTATION
Pathogenesis
Pediculosis capitis is caused by infestation with the human head louse, Pediculus humanus var. capitis ( Fig. 26.1 ). Head louse infestations are seen mostly in children, with 6 to 12 million new cases in the United States each year. The condition is least common in African American children.

Clinical Features
- •
Pruritus is variable, ranging from negligible to severe.
- •
Primary skin lesions consist of macular erythema or erythematous papules on the scalp. The posterior auricular scalp is often most affected ( Fig. 26.2 ). Lymphadenopathy and a morbilliform eruption (pediculid) may be present.

Fig. 26.2
Patient with posterior scalp dermatitis due to head lice infestation. Nits were difficult to find.
(From the Fitzsimons Army Medical Center Collection, Aurora, CO.)
- •
Secondary skin findings include excoriations and crusts.
- •
Lice are difficult to locate because the organisms rapidly relocate when the hair is disturbed. However, nits (louse eggs) are affixed to hair shafts and are usually easy to locate ( Fig. 26.3 ).

Fig. 26.3
Patient with extensive infestation by numerous nits. Nits are red-brown before hatching and light tan or white after hatching.
(From the Fitzsimons Army Medical Center Collection, Aurora, CO.)
Diagnosis
- •
Any dermatitis on the scalp of a young child prompts concern for head louse infestation.
- •
Posterior auricular or cervical lymphadenopathy should raise the index of suspicion further.
- •
The diagnosis is established by the visualization of nits on scalp hair (see Fig. 26.3 ) or by combing the hair with a fine-toothed comb (so-called nit comb) to extract the eggs or lice ( Fig. 26.4 ).
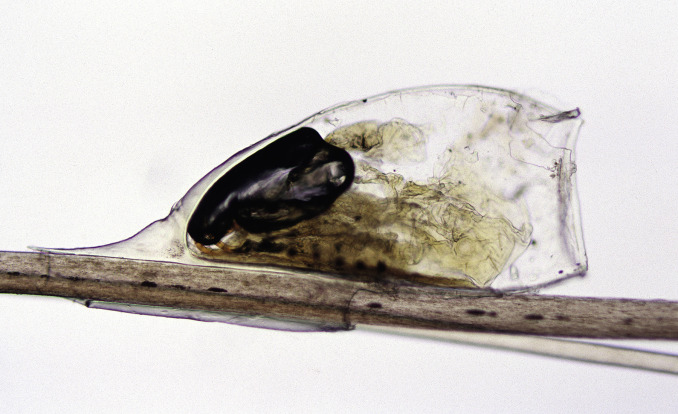
Fig. 26.4
Microscopic appearance of an empty egg casing. Suspected nits should be examined microscopically to differentiate from white hair casts that surround hair shafts.
Treatment
- •
Permethrin, 1% shampoo, has been a long-standing treatment, and it is available over the counter (OTC). However, as of 2015, resistance to permethrin was reported in 25 states. Also, permethrin is not ovicidal, so nits must be removed manually, and a second treatment with permethrin must be applied, 7 to 10 days after first use.
- •
Malathion, 0.5% lotion (Ovide), kills lice and eggs rapidly, although resistance has been reported. It can be used in children 6 years of age and older. Malathion lotion is flammable and expensive.
- •
Pyrethrins with piperonyl butoxide are available OTC and can be used in children 2 years of age and older. Some resistance has been reported in the United States. A second treatment is needed 7 to 10 days later.
- •
Ivermectin may be used as a 0.5% lotion or as a single-dose oral treatment (200 µg/kg). It is not ovicidal. A second treatment is recommended, 7 to 10 days after the first, to kill late-hatching organisms.
- •
Benzyl alcohol, 5% lotion, kills lice but is not ovicidal, and a second treatment is needed 7 days after the first treatment to kill late-hatching lice organisms. It can be irritating to the skin.
- •
Lindane 1% (Kwell), formerly a first-line agent, is now a second-line agent because of toxicity; use is advocated only when other treatments have failed.
- •
Lice require hair to complete their life cycle, and shaving of the scalp is an alternative therapy. Nit removal with combs (wet combing) is a useful adjunctive measure. Diluted vinegar, 8% formic acid, and a specially formulated enzymatic cream rinse may be helping in removing nits.
Clinical Course
The American Academy of Pediatrics (AAP) and the National Association of School Nurses (NASN) are opposed to so-called no-nit policies, and the presence of nits should not bar a child from returning to school.
Pediculosis Pubis
ICD10 code B85.3
ARTHROPOD INFESTATION
Pathogenesis
Pediculosis pubis is due to infestation with the pubic louse, Pthirus pubis , also known as the “crab” louse ( Fig. 26.5 ). Pubic louse infestations are seen primarily in sexually active young adults.

Clinical Features
- •
The infestation usually affects pubic hair. Less often, it affects the eyelashes or scalp of black children.
- •
Pruritus is variable, ranging from negligible to severe.
- •
Primary skin lesions, if present, consist of macular erythema or erythematous papules in the genital region.
- •
Secondary skin findings include excoriations and crusts.
- •
Nits (eggs) vary from a few to many in number ( Fig. 26.6 ). The nits appear red-brown before hatching and light tan or white after hatching.










