Key Words
pediculosis, scabies, Lyme disease, creeping eruption, leishmaniasis, erythema migrans, cat-scratch, bacillary angiomatosis, allergic reaction, myiasis, swimmer’s itch, seabather’s eruption, black fever
Scabies
Human scabies is a highly contagious disease caused by the mite Sarcoptes scabiei var. hominis . The mite is an obligate parasite to humans. Scabies is not primarily a sexually transmitted disease, but sexual transmission does occur ( Table 15.1 ). High-risk persons include men who have sex with men. There is no evidence that mites can transmit infection with the human immunodeficiency virus (HIV).
| Coverage | Recommended Regimen | Alternative Regimen | Special Considerations |
|---|---|---|---|
| Trichomoniasis | Metronidazole 2 g orally in a single dose OR Tinidazole 2 g orally in a single dose Recommended regimen for women with HIV infection: Metronidazole 500 mg orally twice daily for 7 days | Metronidazole 500 mg orally twice a day for 7 days | IgE mediated–type allergy to a nitroimidazole can be managed by metronidazole desensitization |
| Pediculosis pubis | Permethrin 1% cream rinse applied to affected areas and washed off after 10 minutes OR Pyrethrins with piperonyl butoxide applied to the affected area and washed off after 10 minutes | Malathion 0.5% lotion applied to affected areas and washed off after 8–12 hours OR Ivermectin 250 mcg/kg orally, repeated in 2 weeks | Lindane can be considered as an alternative therapy only when other therapies cannot be tolerated or are not effective |
| Scabies | Permethrin 5% cream applied to all areas of the body from the neck down and washed off after 8–14 hours OR Ivermectin 200 mcg/kg orally, repeated in 2 weeks | Lindane (1%) 1 oz of lotion or 30 g of cream applied in a thin layer to all areas of the body from the neck down and thoroughly washed off after 8 hours | Infants and small children should be treated with permethrin Infants and young children aged <10 years should not be treated with lindane |
Scabies spreads in households and neighborhoods in which there is a high frequency of intimate personal contact or sharing of inanimate objects, and fomite transmission is a major factor in household and nosocomial passage of scabies. Dogs and cats may be infested by almost identical organisms (e.g., sarcoptic mange); rarely they may be a source for human infestation, but animal scabies species do not reproduce in humans. In the past, scabies was attributed to poor hygiene. Most contemporary cases, however, appear in individuals with adequate hygiene who are in close contact with numbers of individuals, such as schoolchildren. Scabies is endemic in many developing countries and is usually associated with overcrowding, low socioeconomic standards, and poor hygiene.
Anatomic Features, Life Cycle, and Immunology of the Mite
Anatomic Features.
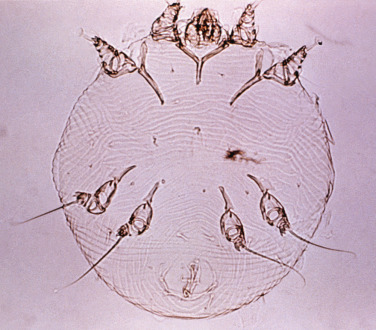
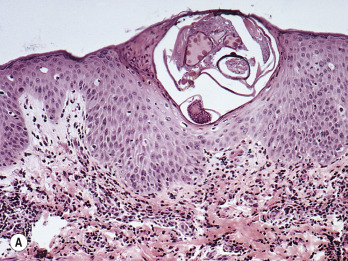
The adult mite is ![]() -mm long and has a flattened, oval body with wrinkle-like, transverse corrugations and eight legs ( Fig. 15.1 ). The front two pairs of legs have claw-shaped suckers and the two rear pairs end in long, trailing bristles. The digestive tract fills a major portion of the body and is readily observed when the mite is seen in cross-section of histologic specimens ( Fig. 15.2A ).
-mm long and has a flattened, oval body with wrinkle-like, transverse corrugations and eight legs ( Fig. 15.1 ). The front two pairs of legs have claw-shaped suckers and the two rear pairs end in long, trailing bristles. The digestive tract fills a major portion of the body and is readily observed when the mite is seen in cross-section of histologic specimens ( Fig. 15.2A ).

Infestation and Life Cycle.
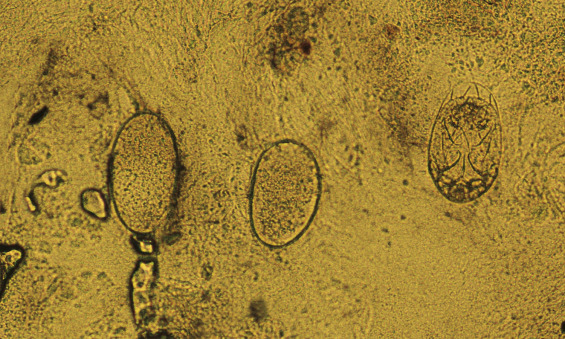
Infestation begins when a fertilized female mite arrives on the skin surface. Within an hour, the female excavates a burrow in the stratum corneum (dead, horny layer) ( Fig. 15.2B ). During the mite’s 30-day life cycle, the burrow extends from several millimeters to a few centimeters in length. The burrow does not enter the underlying epidermis except in the case of hyperkeratotic Norwegian scabies, a condition in which scaly, thick skin develops in intellectually disabled, immunosuppressed, or elderly patients in the presence of thousands of mites. Eggs laid at the rate of two or three a day ( Fig. 15.3 ) and fecal pellets (scybala) are deposited in the burrow behind the advancing female. Scybala are dark, oval masses that are seen easily with the eggs when burrow scrapings are examined under a microscope. Scybala may act as an irritant and may be responsible for some of the itching. The larvae hatch, leaving the egg casings in the burrow, and reach maturity in 14 to 17 days. The adult mites copulate and repeat the cycle. Therefore, 3 to 5 weeks after infestation, there are only a few mites present. This life cycle explains why patients experience few, if any, symptoms during the first month after contact with an infested individual. After a number of mites (usually less than 20) have reached maturity and have spread by migration or the patient’s scratching, the initial, minor, localized itch evolves into intense, generalized pruritus.
Immunology.
A hypersensitivity reaction rather than a foreign-body response may be responsible for the lesions, which may delay recognition of symptoms of scabies. Elevated immunoglobulin E (IgE) titers develop in some patients infested with scabies, along with eosinophilia and an immediate-type hypersensitivity reaction to an extract prepared from female mites. IgE levels fall within a year after infestation. Eosinophilia returns to normal shortly after treatment. The fact that symptoms develop much more rapidly when reinfestation occurs supports the claim that the symptoms and lesions of scabies are the result of a hypersensitivity reaction.
Clinical Manifestations
Transmission of scabies occurs during direct skin contact with an infected person.
A mite can possibly survive for days in normal home surroundings after leaving human skin. Mites survive up to 7 days in mineral oil microscopic slide mounts.
The disease begins insidiously. Symptoms are minor at first and are attributed to a bite or dry skin. Scratching destroys burrows and removes mites, providing initial relief. The patient remains comfortable during the day but itches at night. Nocturnal pruritus is highly characteristic of scabies. Scratching spreads mites to other areas and after 6 to 8 weeks the once localized area of minor irritation has become a widespread, intensely pruritic eruption.
The most characteristic features of the lesions are pleomorphism and a tendency to remain discrete and small. Primary lesions are soon destroyed by scratching.
Primary Lesions
Mites are found in burrows and at the edge of vesicles but rarely in papules.
Burrow.
The linear, curved, or S-shaped burrows are approximately as wide as no. 2 suture material and are 2 to 15 mm long ( Fig. 15.4 ). They are pink-white and slightly elevated. A vesicle or the mite, which may look like a black dot at one end of the burrow, often may be seen. Scratching destroys burrows; therefore they do not appear in some patients. Burrows are most likely to be found in the finger webs, wrists, sides of the hands and feet, penis, buttocks, scrotum, and the palms and soles of infants.

Vesicles and Papules.
Vesicles are isolated, pinpoint and filled with serous rather than purulent fluid. The fact that the vesicles remain discrete is a key point in differentiating scabies from other vesicular diseases such as poison ivy. The finger webs are the most likely areas to find intact vesicles ( Fig. 15.5 ). Infants may have vesicles or pustules on the palms and soles. Small, discrete papules may represent a hypersensitivity reaction and rarely contain mites.

Secondary Lesions
Secondary lesions result from infection or are caused by scratching. They often dominate the clinical picture. Pinpoint erosions are the most common secondary lesions ( Fig. 15.6 ). Pustules are a sign of secondary infection. Scaling, erythema, and all stages of eczematous inflammation occur as a response to excoriation or to irritation caused by overzealous attempts at self-medication. Nodules occur in covered areas such as the buttocks, groin, scrotum, penis, and axillae ( Fig. 15.7 ). The 2 to 10 mm indolent, red papules and nodules sometimes have slightly eroded surfaces, especially on the glans penis ( Fig. 15.8 ![]() ). Nodules may persist for weeks or months after the mites have been eradicated. They may result from persisting antigens of mite parts.
). Nodules may persist for weeks or months after the mites have been eradicated. They may result from persisting antigens of mite parts.





Distribution
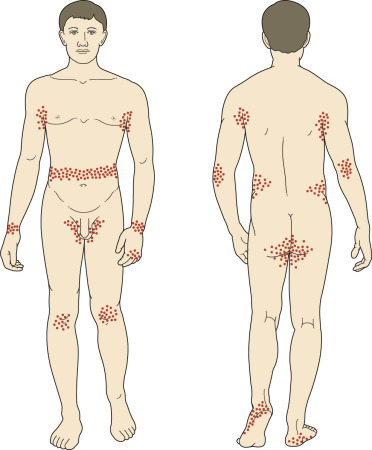
Lesions of scabies are typically found in the finger webs, wrists, extensor surfaces of the elbows and knees, sides of the hands and feet, axillary areas, buttocks, waist area, and ankle area ( Figs. 15.9 ![]() to 15.12 ). In men, the penis and scrotum are usually involved; in women, the breast, including the areola and nipple, may be infested. Lesions, often vesicular or pustular, may be most numerous on the palms and soles of infants. The scalp and face, rarely involved in adults, occasionally are infested in infants.
to 15.12 ). In men, the penis and scrotum are usually involved; in women, the breast, including the areola and nipple, may be infested. Lesions, often vesicular or pustular, may be most numerous on the palms and soles of infants. The scalp and face, rarely involved in adults, occasionally are infested in infants.



The number and type of lesions and the extent of involvement vary greatly among patients. Some patients have a few itchy vesicles in the finger webs early in the course of their disease. Many patients in these early stages attempt self-treatment and are encouraged by the relief obtained from over-the-counter antipruritic lotions. Topical steroids offer greater relief but mask the progressive disease by suppressing inflammation. Delay of proper treatment allows the eruption to extend into all of the characteristic areas, as well as onto the trunk, arms, legs, and occasionally the face. Extensive involvement is often accompanied by erythema, scaling, and infection. Infants and children have diffuse scabies more often than do adults. Symptoms vary from periods of nocturnal pruritus to constant, frantic itching. Untreated scabies can last for months or years.
Infants
Infants, more frequently than adults, have widespread involvement. This may occur because the diagnosis is not suspected and proper treatment is delayed while medication is given for other suspected causes of itching, such as dry skin, eczema, and infection. Infants occasionally are infested on the face and scalp, something rarely seen in adults. Vesicles are common on the palms and soles; this is a highly characteristic sign of scabies in infants (see Fig. 15.6 ). Secondary eczematization and impetiginization are common, but burrows are difficult to find. Nodules may be seen in the axillae and diaper area.
The Elderly
Elderly patients may have few cutaneous lesions but itch severely. The decreased immunity associated with advanced age may allow the mites to multiply and survive in great numbers. These patients have few cutaneous lesions other than excoriations, dry skin, and scaling, but they experience intense itching. Eventually papules and nodules appear and may become numerous ( Figs. 15.13 to 15.15 ). Entire nursing home populations may be infested (see Treatment and Management section , below). A skin scraping from any scaling area may show numerous mites at all stages of development.



Crusted (Norwegian) Scabies
The term Norwegian scabies was first used in 1848 to describe an overwhelming scabies infestation of patients with Hansen disease. In patients with crusted scabies, lesions tend to involve hands and feet with asymptomatic crusting rather than the typical inflammatory papules and vesicles ( Fig. 15.16 ). There is thick, subungual, keratotic material and nail dystrophy. Digits and sites of trauma may show wart-like formations. Gray scales and thick crusts may be present over the trunk and extremities. Desquamation of the facial skin may occur. The hair may shed profusely. Crusted scabies occurs in people with neurologic or mental disorders (especially Down syndrome), senile dementia, nutritional disorders, infectious diseases, leukemia, and immunosuppressive disorders (such as patients with acquired immunodeficiency syndrome [AIDS]). Itching may be absent or severe. A lack of immunity and indifference to pruritus have been suggested as reasons for the development of this distinct clinical picture. A mineral oil or potassium hydroxide examination of crusts shows numerous mites at all stages of development.

Diagnosis
The diagnosis is suspected when burrows are found or when a patient has typical symptoms with characteristic lesions and distribution ( Box 15.1 ). In a report from a sub-Saharan region, the presence of diffuse itching and visible lesions associated either with at least two typical locations of scabies or with a household member with itching had 100% sensitivity and 97% specificity for the diagnosis.
- •
Nodules on the penis and scrotum
- •
Sudden worsening of a rash present for 4 to 8 weeks
- •
Pustules on the palms and soles of infants
- •
Nocturnal itching
- •
Generalized, severe itching
- •
Pinpoint erosions and crusts on the buttocks
- •
Vesicles in the finger webs
- •
Diffuse eruption sparing the face
- •
Patient improves and then worsens after treatment with topical steroids
- •
Rash present in several members of the same family
- •
Patient (especially an infant) develops more extensive rash despite treatment with antibiotics and topical medications
A definite diagnosis is made when any of the following products are obtained from burrows or vesicles and identified microscopically: mites, eggs, egg casings (hatched eggs), or feces (scybala). About 5 to 15 female mites live on a person infected with classic scabies. Failure to find a mite is common and does not rule out the diagnosis of scabies. Hundreds or thousands of mites can occur in cases of crusted scabies. Mites are easily demonstrated in such patients.
Burrow Identification
Initially, the areas most apt to contain burrows are observed. To enhance burrows for better viewing, the surface should be touched with a drop of mineral or immersion oil or a blue or black fountain or felt-tip pen (the ink method dyes the burrow; surface ink may be removed with an alcohol swab). The burrow absorbs the ink and is highlighted as a dark line ( Fig. 15.17 ). The accentuated lesions are smoothly scraped away with a curved no. 15 scalpel blade and transferred to a glass microscope slide for examination.

Sampling Techniques and Slide Mount Preparation
Various techniques are available for obtaining diagnostic material. In most cases the suspected lesion can be sampled easily if it is shaved or scraped with a no. 15 surgical blade and the material is transferred to a microscope slide for direct examination.
Mineral Oil Mounts.
A drop of mineral oil may be placed over the suspected lesion before removal. Skin scrapings adhere, feces are preserved, and the mite remains alive and motile in clear oil. Squamous cells do not separate when heated in a clear oil mount, and mites under a clump of squamous cells may be missed. Mites migrate on a glass slide greased with oil, even when it is covered with a coverslip. To prevent mites from leaving the area under the coverslip or from becoming entangled at the edge of it, where they are difficult to see, the coverslip has to be sealed with nail polish and the slide must be kept in a refrigerator, if not examined immediately.
Potassium Hydroxide Wet Mounts.
The scrapings are transferred directly to a glass slide, a drop of potassium hydroxide is added, and a coverslip is applied. If diagnostic material is not found, the preparation is gently heated and the coverslip is pressed to separate squamous cells. Feces remain intact for short periods but may be dissolved quickly when the mount is heated. Skin biopsy is rarely necessary to make the diagnosis.
Adhesive Tape.
This method is simple and useful for the diagnosis of scabies infestation in long-term care nursing units or in facilities where scraping lesions is not practical. Transparent adhesive tape (Tartan tape) is cut into strips the size of a microscope slide (25 × 50 mm), firmly applied to a lesion, and then pulled off rapidly. The tape is transferred to a slide and the slide is stored at 10° C to 14° C until it is read. Slides are scanned at ×40 magnification. If a mite is suspected, the magnification is increased to ×100.
Dermoscopy
Dermoscopy is performed using a handheld dermatoscope with ×10 magnification. The “delta wing sign” indicates the presence of a mite. Under ×10 magnification, the mite appears as a triangular shape resembling a circumflex accent (e.g., in French, the letter ô). The circumflex accent corresponds to the head and front legs of the mite as seen at higher magnification. The shape of the body mite is sometimes seen at low magnification.
Treatment and Management
Permethrin
Permethrin (Elimite cream) is a synthetic pyrethrin that demonstrates extremely low mammalian toxicity. It is the drug of choice for the treatment of scabies in children and adults of all ages including pregnant and lactating women. Studies show that cure rates are similar to or better than those for lindane. A diminished sensitivity to permethrin has been documented. One application is said to be effective but a second treatment 1 week after the first application is standard practice. The over-the-counter permethrin preparation Nix is lower in strength (1%) and ineffective against scabies. Unlike lindane, permethrin undergoes insignificant absorption (2%), after which it is rapidly degraded ( Table 15.2 ).
| Treatment | Dosage | Treatment Regimen | Contraindication | Advantages | Disadvantages | Comments |
|---|---|---|---|---|---|---|
| Permethrin | 5% cream | Rinsed off after 8–12 hours | Effective, well tolerated, safe | Itching and stinging on application | Second application often routinely prescribed 1 week after the first application | |
| Lindane | 1% lotion or cream | Rinsed off after 6 hours | Pregnant women, infants, seizure disorders | Effective, inexpensive | Cramps, dizziness, seizures in children | Withdrawn in the European Union because of neurotoxicity concerns |
| Benzyl benzoate | 25% ointment | Rinsed off after 24 hours (once or several times) | Pregnant women and infants (limit duration of use to 12 hours) | Effective, inexpensive | Can cause severe skin irritation | Not currently available in Canada, approved in Europe |
| Crotamiton | 10% ointment | Rinsed off after 24 hours and then reapplied for an additional 24 hours | Well tolerated, safe for infants | Questionable efficacy | Not available in Canada, often used on scabies nodules in children | |
| Precipitated sulfur | 2%–10% precipitate in petroleum base | Rinsed off after 24 hours and then reapplied every 24 hours for the next 2 days (with a bath taken between each application) | Safe for infants, and pregnant and breast-feeding women | Questionable efficacy, skin irritation | ||
| Ivermectin | Pills | 200 mcg/kg repeated on day 14 | Children <15 kg; pregnant or breast-feeding women | Good patient compliance | Expensive | Not approved in many countries |
Lindane
Lindane is the generic name for the chemical γ-hexachlorocyclohexane, a compound chemically similar to an agricultural pesticide also referred to as lindane . It is a central nervous system (CNS) stimulant that produces seizures and death in the scabies mite. Kwell is one brand name for lindane. Generic lindane is available. Lindane is available as a cream, shampoo, and lotion. Lotion dispensed from bulk containers may not be agitated; therefore the concentration of lindane may be inadequate. Reports of lindane resistance have appeared. A second treatment 1 week after the first application is standard practice. A follow-up examination at 2 to 4 weeks is recommended. Approximately 10% of lindane is absorbed through intact skin. Lindane accumulates in fat and binds to brain tissue. Pruritus may persist for weeks. Additional, unprescribed applications, without documented evidence of persistent infestation, may be dangerous. Lindane should be avoided in children younger than 2 years of age, pregnant or nursing women, and patients with HIV or AIDS. Children with severe, underlying, cutaneous disease may be at greater risk for toxicity. This is also true for premature, emaciated, or malnourished children and those with a history of seizure disorders. Lindane is no longer available in the United Kingdom or Australia.
Application Technique for Permethrin and Lindane.
The cream or lotion is applied to all skin surfaces below the neck and the face in children. Patients with relapsing scabies and the elderly should be treated from head (including the scalp) to toe. One ounce is usually adequate for adults. Reapply medicine to the hands if hands are washed. The nails should be cut short and medication applied under them vigorously with a toothbrush. A hot, soapy bath is not necessary before application. Moisture increases the permeability of the epidermis and increases the chance for systemic absorption. If a patient has bathed before lindane administration, the skin must be allowed to completely dry to prevent excessive absorption. Adults should wash 12 hours after application, and infants should be washed 8 to 12 hours after application. One application of either medicine is considered adequate. Many clinicians prefer two applications 1 week apart. Patients should be told that it is normal to continue to itch for days or weeks after treatment and that further application of medication is usually not necessary and worsens itching by causing irritation. Bland lubricants may be applied to relieve itching.
Benzyl Benzoate
The 25% lotion is the most common preparation. A standard program in developing countries consists of a bath with monosulfiram soap followed by application of benzyl benzoate lotion to the entire body below the neck, repeated daily for 3 to 5 consecutive days. Reported cure rates vary from 50% to more than 80%. It may cause irritant dermatitis, especially in the genital area and on the face. There is no evidence for adverse effects on pregnancy outcome. It is not available in the United States.
Crotamiton (Eurax Lotion)
The toxicity of crotamiton is unknown. Reported cure rates for once-a-day application for 2 to 5 days range from 50% to 100%. Crotamiton may have antipruritic properties, but this has been questioned.
Sulfur
Sulfur has been used to treat scabies for more than 150 years. The pharmacist mixes 8% (5% to 10% range) precipitated sulfur in petrolatum or a cold cream base. The compound is applied to the entire body below the neck once each day for 3 days. The patient is instructed to bathe 24 hours after each application. Sulfur applied in this manner is highly effective, but these preparations are messy, have an unpleasant odor, stain, and cause dryness.
Ivermectin (Stromectol)
Ivermectin is used for patients who fail topical therapy, the elderly, patients with generalized eczema, or those who cannot tolerate or comply with topical therapy. Cure rates increase when ivermectin is used in combination with topical scabicides. A single dose of ivermectin (200 mcg/kg) is reported to be 59% to 80% effective for the treatment of scabies. The cure rate increases to 93% if a second ivermectin dose is taken 2 weeks later. The standard single dose is two Stromectol 6-mg tablets for a 70-kg person. It is important to dose by weight and increase the dose for heavier patients (see Table 15.2 ).
Scabies in Long-Term Care Facilities
Scabies in a nursing home can be highly disruptive. The staff, families, and patients become anxious about issues of treatment, origin of infestation, hygiene, and communicability. Everyone has a sense of urgency. Diagnosis is often a problem.
Diagnosis.
It is important to confirm the diagnosis microscopically before committing large financial resources to treatment. The diagnosis of scabies should be considered in any nursing home resident with an unexplained generalized rash. The clinical presentation may vary in older, immunocompromised, or cognitively impaired persons. Erythematous, papulosquamous lesions are predominantly truncal. Pruritus is often absent.
Eradication Program for Nursing Homes.
Scabies is a problem in nursing homes. The severity is greater than that in an ambulatory population. The face and scalp can be involved, and multiple treatments may be necessary. The first problem is proper diagnosis. The elderly have an atypical presentation with few lesions other than excoriations, dry skin, and scaling, but they experience intense itching. Lesions are located on the back and buttocks rather than on the web spaces, axilla, and groin. A plan for eradication of scabies in nursing homes is outlined in Box 15.2 ![]() .
.
| I. P lanning and O rganization | |
| Formation and regular meetings of a management team with clear assignment of responsibilities |
|
| Development of a time schedule |
|
| Preparation of person lists |
|
| Information of all involved persons |
|
| Reservation of suitable rooms for examination and treatment |
|
| Clarification of reimbursement of costs |
|
| Other |
|
| II. S ynchronous I nitial E xamination | |
| Preparation and assistance |
|
| Nursing activities |
|
| Physician’s examination and documentation |
|
| Calculation and ordering of the required amount of antiscabietic |
|
| III. S imultaneous T herapy of A ll A ffected and C ontact P ersons | |
| Preparation and assistance |
|
| Topical therapy with 5% permethrin in a cream base |
|
| Systemic therapy with ivermectin in weight-adapted dosage |
|
| IV. D econtamination and Q uarantine M easures | |
| Cleaning of clothing, bed linens, towels, etc. |
|
| Cleaning of surfaces, furniture, and objects |
|
| Minimization of transmission pathways |
|
| Isolation of those affected |
|
| V. F ollow-up E xaminations and T reatments | |
| Schedule 2 weeks after the last treatment (day 28) |
|
| Treatment of all still or newly affected persons |
|
| Repeated follow-up examination of all definitely and possibly affected persons at intervals of 14 days |
|
Management of Complications
Eczematous Inflammation and Pyoderma.
Patients with signs of infection should be prescribed systemic antibiotics that treat Staphylococcus aureus and Streptococcus pyogenes . A group V topical steroid may be applied three times a day to all red, scaling lesions for 1 or 2 days before the application of lindane.
Postscabietic Pruritus.
Pruritus may persist for weeks after treatment and may be attributed to a hypersensitivity response to remaining dead mites and mite products.
Itching usually decreases substantially 24 hours after treatment and then gradually decreases during the following 1 or 2 weeks. Patients with persistent itching may be treated with oral antihistamines, and, if inflammation is present, they may be treated with topical steroids. Intractable itching responds to a short course of systemic corticosteroids.
Nodular Scabies.
Nodular scabies is an infrequent manifestation of scabies that presents with pruritic, red-brown nodules, especially in the genital, gluteal, and axillary regions, persisting for weeks or months after successful scabies treatment. Persistent nodular lesions are treated with intralesional steroids (e.g., triamcinolone acetonide 10 mg/mL). Nodules sometimes contain mites and will require retreatment for eradication.
Environmental Management.
Intimate contacts and all family members in the same household should be treated. The spread of scabies via inanimate objects occurs. Live mites have been recovered from dust samples, chairs, and bed linens in the homes of patients with scabies up to 96 hours after being isolated from the host. Clothing that has touched infected skin should be washed. Wash all clothing, towels, and bed linens (in a normal washing machine cycle) that have touched the skin. It is not necessary to rewash clean clothing that has not yet been worn. Bed linens, floors, and chairs should be vacuumed and cleaned. It is especially important to thoroughly clean the rooms of patients who are confined in single rooms in long-term care facilities.
Pediculosis
Infestation with lice is called pediculosis . Lice are transmitted by close personal contact and contact with objects such as combs, hats, clothing, and bed linen. Infestation is usually symptomless and is not associated with serious disease. Lice cannot jump or fly. Pets are not vectors. Diagnosis is made by visualizing the lice or their eggs. Treatment with lindane, permethrin, pyrethrins, and malathion is used, but resistance to all medications has been documented in various countries.
Biology and Life Cycle
Lice are obligate human parasites that cannot survive off their host for more than 10 days (adults) to 3 weeks (fertile eggs). Actual survival rates may be shorter than this. Lice are called ectoparasites because they live on, rather than in, the body. They are classified as insects because they have six legs. Three kinds of lice infest humans: Pediculus humanus var. capitis (head louse), Pediculus humanus var. corporis (body louse), and Phthirus pubis (pubic or crab louse). All three have similar anatomic characteristics. Each is a small (less than 2 mm), flat, wingless insect with three pairs of legs located on the anterior part of the body directly behind the head. The legs terminate in sharp claws that are adapted for feeding and permit the louse to grasp and hold firmly onto hair or clothing. The body louse is the largest and is similar in shape to the head louse ( Fig. 15.18 ). The crab louse is the smallest, with a short, oval body and prominent claws resembling sea crabs ( Fig. 15.19 ).


Lice feed approximately five times each day by piercing the skin with their claws, injecting irritating saliva, and sucking blood. They do not become engorged like ticks, but after feeding they become rust colored from the ingestion of blood; their color is an identifying characteristic. Lice feces can be seen on the skin as small, rust-colored flecks. Saliva and, possibly, fecal material can induce a hypersensitivity reaction and inflammation. Lice are active and can travel quickly, which explains why they can be transmitted so easily. The life cycle from egg to egg is approximately 1 month.
Nits
The female lays approximately six eggs, or nits, each day for up to 1 month, and then dies. The louse incubates, hatches in 8 to 10 days, and reaches maturity in approximately 18 days. Nits are 0.8 mm long and are firmly cemented to the bases of hair shafts close to the skin to acquire adequate heat for incubation ( Fig. 15.20 ). Nits are very difficult to remove from the hair shaft.

Clinical Manifestations
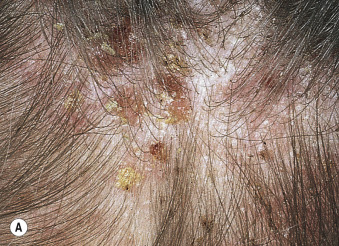
Pediculosis Capitis
The head louse effectively infests only the human head and is distinct from body and pubic lice. Lice infestation of the scalp is most common in children. More girls than boys are afflicted and American black people rarely have head lice. Head lice can be found anywhere on the scalp, but are most commonly seen on the back of the head ( Fig. 15.21 ) and neck and behind the ears. The average patient carries less than 20 adult lice. Less than 5% of patients will have more than 100 lice in the scalp. Scratching causes inflammation and secondary bacterial infection, with pustules, crusting, and cervical adenopathy. Sensitization to the lice toxin, feces, or body parts takes 3 to 8 months and is a cause of pruritus. Posterior cervical adenopathy without obvious disease is characteristic of lice. The eyelashes may be involved, causing redness and swelling. Examination of the posterior scalp shows few adult organisms but many nits. Nits are cemented to the hair, whereas dandruff scale is easily moved along the hair shaft ( Fig. 15.21B ). Head lice can survive away from the human host for about 3 days, and nits can survive for up to 10 days. The primary source of transmission is direct contact with an infested person but fomite transmission (hats, brushes, combs, earphones, bedding, furniture) is common. Head lice do not carry or transmit any human disease.

Pediculosis Corporis
Infestation by body lice is uncommon. Typhus, relapsing fever, and trench fever are spread by body lice during wartime and in underdeveloped countries. Pediculosis corporis is a disease of the unclean. Body lice live and lay their nits in the seams of clothing and return to the skin surface only to feed. They run and hide when disturbed and are rarely seen. Body lice induce pruritus that leads to scratching and secondary infection.
Eyelash Infestation.
Infestation of the eyelashes is seen almost exclusively in children. The lice are acquired from other children or from an infested adult with pubic lice. Eyelash infestation may induce blepharitis with lid pruritus, scaling, crusting, and/or purulent discharge. Eyelash infestation may be a sign of childhood sexual abuse ( Fig. 15.22 ).

Pediculosis Pubis
Pubic lice are the most contagious sexually transmitted problem known ( Table 15.1 ). Up to 30% of patients infested with pubic lice have at least one other sexually transmitted disease. The chance of acquiring pubic lice from one sexual exposure with an infested partner is more than 90%, whereas the chance of acquiring syphilis or gonorrhea from one sexual exposure with an infected partner is approximately 30%. Black people are affected with the same frequency as white people. The pubic hair is the most common site of infestation ( Fig. 15.23 ), but lice frequently spread to the hair around the anus. On hairy persons, lice may spread to the upper thighs, abdominal area, axillae, chest, and beard. Infested adults may spread pubic lice to the eyelashes of children.

The majority of patients complain of pruritus. Many patients are aware that something is crawling on the groin, but are not familiar with the disease and have never seen lice. Approximately 50% of patients have little inflammation, but those who delay seeking help may develop widespread inflammation and infection of the groin with regional adenopathy. Occasionally, gray-blue macules (maculae ceruleae) varying in size from 1 to 2 cm are seen in the groin and at sites distant from the infestation. Their cause is not known, but they may represent altered blood pigment.
Diagnosis
Lice are suspected when a patient complains of itching in a localized area without an apparent rash. Scalp and pubic lice will be apparent to those who carefully examine individual hairs; they are not apparent with only a cursory examination. Finding nits does not indicate active infestation. Nits may persist for months after successful treatment. Live eggs reside within a quarter inch of the scalp.
Combing
Combing the hair with a fine-toothed “nit,” or detection, comb is effective for detecting and removing live lice. The comb is inserted near the crown until it touches the scalp, and then drawn firmly down. The teeth of the comb should be 0.2 to 0.3 mm apart to trap lice. The entire head of hair should be combed at least twice; the comb should be examined for lice after each stroke. It usually takes 1 minute to find the first louse.
Lice and nits can be seen easily under a microscope. Live nits fluoresce and can be detected easily by Wood’s light examination, a technique that is especially useful for rapid examination of a large group of children. Nits that contain an unborn louse fluoresce white. Nits that are empty fluoresce gray.
Treatment
Treatment options for head lice are presented in Table 15.3 .
| Treatment | Ovicidal | Directions | Cost | Comments |
|---|---|---|---|---|
| Benzyl alcohol 5% lotion (Ulesfia) | No | Apply to dry hair, leave on for 10 min, then rinse; repeat in 7 days. | $63 (227-g bottle) | Can be costly for long hair (dosed by hair length) Must be used in conjunction with nit combing Approved for children 6 months and older; can be used in pregnant and lactating women |
| Ivermectin (Stromectol; not FDA- approved for treatment of pediculosis) | No | Administer 200–400 mcg/kg, given on day 1 and day 8 (total of two doses). | $5 to $10 per 3-mg tablet (total cost dependent on weight) | Should not be used in children weighing less than 33 lb (15 kg) or in pregnant or breast-feeding women Common adverse effects include dizziness and pruritus |
| Ivermectin (Sklice lotion 0.5%) | Yes | Apply lotion to hair and wash out in 10 min. Combing out nits is unnecessary. | $283 | For patients 6 months of age and older. |
| Malathion 0.5% lotion (Ovide) | Partial | Apply to dry hair enough to sufficiently wet the hair and scalp; allow hair to dry naturally. Shampoo 8–12 hours later, rinse, and use lice comb. Repeat after 7 to 9 days if live lice still are present. | $185 (59-mL bottle) | Flammable; do not use hair dryer, cigarettes, or open flame while hair is wet |
| Permethrin 1% lotion (Nix) | No | Apply to damp hair and leave on for 10 min, then rinse; repeat in 7 days. | $20 for two 59-mL bottles | First-choice treatment per CDC guidelines |
| Pyrethrins 0.3%/piperonyl butoxide 4% shampoo or mousse (Rid) | No | Apply to dry hair and leave on for 10 min, then rinse. | $20 for 236 mL | Piperonyl butoxide is thought to prolong activity of pyrethrins; avoid in patients with chrysanthemum allergy |
| Spinosad 0.9% topical suspension (Natroba) | Yes | Apply to dry hair, leave on for 10 min, then rinse; repeat in 7 days only if live lice are seen. | $263 (4-oz bottle) | Safe for use in children 4 years and older; may be used without nit combing, although best results occur with nit combing Do not use in infants younger than 6 months because of benzyl alcohol content |
Head, Body, and Pubic Lice
Permethrin 1% or malathion is first-line treatment. Resistance to all topical medications has been documented. Some head lice in the United States have become resistant to 1% lindane, Nix, and pyrethrins. Malathion is the only pediculicide in the United States that has not become less effective. Insecticides kill both lice and eggs. A fine-toothed comb should be used 1 or 2 days after the final application of insecticide to confirm that the treatment has been successful. The presence of live (moving) lice of all sizes suggests resistance to treatment, whereas finding only one adult-sized louse suggests reinfestation. Regular weekly detection combing is recommended for several weeks after cure. Household members and those in close contact with the patient should be screened and treated as necessary. Environmental cleaning is probably unwarranted, although combs and brushes should be washed in hot water.
Permethrin.
Permethrin is the most effective over-the-counter treatment. It paralyzes the nerves that allow the lice to breathe. Lice can close their respiratory airways for 30 minutes when immersed in water. Therefore, all insecticides are applied to dry hair. The cream rinse (Nix) is applied to the scalp after the hair is shampooed and dried. The medication is rinsed out with water after 10 minutes. Permethrin is not 100% ovicidal, and higher cure rates may be obtained by a second application 1 week after the first treatment. Developing eggs have no CNS during the first 4 days of life. Insecticides that act on the metabolism of neural tissue must have residual activity to be ovicidal. Permethrin has a clinical efficacy of 95%. Lindane and pyrethrin have cure rates less than 90%. Permethrin, unlike pyrethrin and all other topical insecticides, remains active for 2 weeks and is detectable on the hair for 14 days. Cream rinses and conditioning shampoos coat the hairs and protect the lice from the insecticide. Do not use these products for 2 weeks after permethrin treatment. Patients who fail to respond may respond to the prescription strength cream (5% permethrin). The medication is left on overnight under a shower cap.
Pyrethrin.
Pyrethrin is available as a liquid, gel, and shampoo. The shampoos are applied, lathered, and washed off in 5 minutes. Lotions are used for treating body and pubic hair infestation. They are applied over the entire affected area and washed off in 10 minutes. Treatment should be repeated in 7 to 10 days. It does not kill all nits and has no residual activity. It is used a second time 1 week after the initial application.
Malathion.
Malathion is rapidly pediculicidal and ovicidal and is useful for lice resistant to pyrethrins and permethrin. It binds to hair and has residual activity. One treatment is usually sufficient. The lotion is applied to dry hair until the hair and scalp are wet. It does not need to be applied to the ends of long hair below the level of the shirt collar. It is left on for 8 to 12 hours and then removed. Nits are removed with a comb. The treatment is repeated in 7 to 9 days if lice are still present. The alcoholic preparation Ovide is flammable until dry. Malathion is available by prescription in the United States but is over-the-counter in the United Kingdom. A 1% shampoo is available outside of the United States. It is applied to the scalp and rinsed off 10 minutes later, and then the procedure is repeated 1 week later. It is not recommended for infants and neonates.
Lindane.
Lindane 1% shampoo is indicated for patients who have failed to respond to the previously listed medications or who are intolerant to other lice therapies. Resistance of the louse to lindane is reported.
Ivermectin.
Ivermectin causes paralysis and death of lice. The drug has selective activity against parasites, without systemic effects in mammals. A single oral dose of ivermectin 200 mcg/kg repeated in 10 days is effective. A single dose of 12 mg (two 6-mg pills) is generally used for an average-sized adult. The efficacy is 73% after a single dose. Results were more favorable when ivermectin was used in combination with the LiceMeister comb ( www.licemeister.org ).
Ivermection Lotion.
Ivermectin lotion is a treatment option when permethrin or pyrethrins have failed or when there is a desire to reduce the need for nit combing and increase the probability of success with a single application. More than 90% of ivermectin-treated patients are louse-free 1 day after application.
Spinosad.
Spinosad 0.9% topical suspension has pediculicidal and ovicidal activity. It was introduced in 2011 and is approved in children 4 years of age and older for the treatment of head lice infestations. It is effective against head lice with permethrin resistance. The distinguishing factor between spinosad and other topical therapies for lice, such as permethrin, is the ability to kill nits. Head lice and nits are cleared from more than 90% of patients following a single application. Spinosad is applied to dry hair and scalp for 10 minutes and then rinsed with warm water. Nit picking is not necessary. If live lice are seen a week later, a second treatment is applied. It is very expensive.
Trimethoprim/Sulfamethoxazole.
A rare patient with severe hair matting and dense infestation may not respond to conventional treatment. The two remaining options are shaving the head or treating the patient with trimethoprim/sulfamethoxazole (TMP/SMX). A study of 20 females with pediculosis capitis showed that 1 tablet of Bactrim or Septra (80 mg of TMP plus 400 mg of SMX) twice daily for 3 days resulted in a cure. Within 12 to 48 hours after treatment, the lice migrated to the bed linen and died. Trimethoprim/sulfamethoxazole probably works by killing essential bacteria in the louse’s gut. Cotrimoxazole has no effect on nits; therefore a second course must be given 7 to 10 days later.
A combination of 1% permethrin creme rinse (two weekly applications) and TMP/SMX (10-day course) was effective in one study for treating children 2 to 13 years old. Dual therapy can be reserved for cases of multiple treatment failures or for suspected cases of lice-related resistance to therapy.
Nit Removal
All preparations kill lice, but some nits may survive. Even dead nits remain attached to the hair until removed. Nits are difficult to remove. Over-the-counter “nit looseners” or “nit removers” are probably not very effective. Applying hair conditioner, gripping the hair with the index finger and thumb, and sliding the nits off is an effective treatment solution.
A special comb, the LiceMeister ( www.licemeister.org ), has ![]() -inch-long metal teeth that penetrate more hair with each pass, collecting both lice and nits. It is available online and at pharmacies. As many nits as possible should be removed to prevent reinfestation. A close haircut may be considered for patients with hundreds of nits.
-inch-long metal teeth that penetrate more hair with each pass, collecting both lice and nits. It is available online and at pharmacies. As many nits as possible should be removed to prevent reinfestation. A close haircut may be considered for patients with hundreds of nits.
Wet Combing (Bug Busting).
Special busting kits are sold with a comb in which the spacing between the teeth is narrow enough to trap the smallest lice but wide enough to pass easily through the hair. Mechanical removal of lice with a wet comb is an alternative to insecticides. The combing procedure is the same as that followed for diagnosis but is performed on wet hair with added lubricant (hair conditioner or olive oil) and continued until no lice are found (15 to 30 minutes per session or longer for long, thick hair). Combing is repeated once every 3 to 4 days for several weeks and should continue for 2 weeks after any session in which an adult louse is found. Reported cure rates vary from 38% to 57%.
Pomades.
Petrolatum, mayonnaise, and pomades immobilize lice and kill them in about 10 minutes. Copious amounts must be used to ensure inundation of the adult lice in the scalp hair. These noninsecticidal therapies do not kill the eggs (nits), which take 8 to 10 days to hatch. These therapies must be repeated weekly for 4 weeks unless it is possible to remove all the nits by combing.
Hot Air.
One 30-minute application of hot air has the potential to eradicate head lice infestations. A custom-built machine called the LouseBuster was effective in killing lice and their eggs when operated at a comfortable temperature, slightly cooler than a standard blow-dryer.
Fomite Control.
Fomite control is important to prevent reinfestations. Clean bed linens, pillows, towels, clothing, and hats. Rugs, furniture, mattresses, and car seats should be thoroughly vacuumed.
“No Nit” Policies
Exclusion from school for head lice is a common practice. Three-quarters of children with nits alone are not infested, and no-nit policies are therefore excessive. Exclusion from school based on the presence of lice or nits is not recommended. A child can return to school immediately after completion of the first application of a normally effective insecticide or the first wet combing session, regardless of the presence of nits. It would be useful to provide a letter of explanation to the school nurse.
Eye Infestation
Several methods are used for treating eye infestation. The most practical and effective method is to place petrolatum (Vaseline) on the fingertips, close the eyes, and rub the petrolatum slowly into the lids and brows three times each day for 5 days. A simple alternative is to close the eyes and apply baby shampoo to the lashes and brows with a cotton swab three times each day for 5 days. Some patients are so mortified by the presence of lice close to their eyes that they demand immediate removal. To do so, the reclining patient closes the eyes and the lice are plucked from the eyelashes with forceps. Older children tolerate this simple procedure. Fluorescein drops (10% to 20%) applied to the lids and lashes produce an immediate toxic effect on the lice. Oral ivermectin should be considered for resistant cases.
Spiders
Spiders are carnivorous arthropods that have fangs and venom, which they use to catch and immobilize or kill their prey. Most spiders are small and their fangs are too short to penetrate human skin. Spiders are not aggressive and bite only in self-defense. Spider bites may not be felt at the instant they occur. Localized pain, swelling, itching, erythema, blisters, and necrosis may occur. Most spider venoms are composed of the harmless, enzyme-spreading factor hyaluronidase and a toxin that is distributed by the spreading factor. Most toxins simply cause pain, swelling, and inflammation; however, brown recluse spider toxin causes necrosis, and black widow spider toxin causes neuromuscular abnormalities.
Spider bites are common, but of the 50 species of spiders in the United States that have been known to bite humans, only the black widow and the brown recluse spiders are capable of producing severe reactions ( Table 15.4 ). The diagnosis of a spider bite cannot be made with certainty unless the act is witnessed or the spider is recovered.
| Bite Characteristics | Widow Spider ( Latrodectus ) Bites | Recluse Spider ( Loxosceles ) Bites |
|---|---|---|
| Initial bite symptoms | Moderately to severely painful; little or no surrounding inflammation | Painless or minimally painful; localized inflammation that subsequently spreads |
| Presumed mechanism of envenomation | Massive presynaptic discharge of all autonomic neurotransmitters | Local cytotoxicity with subsequent ulcerating dermonecrosis |
| Predominant toxin | α-Latrotoxin | Sphingomyelinase D |
| Potential for systemic toxicity | Present; usually atypical and rarely full-blown (latrodectism) | Present but rare (loxoscelism) |
| Incubation period from bite to systemic toxicity | Rapid (i.e., 30 min to 2 hours) | Delayed (i.e., 3 to 7 days) |
| Most common signs of systemic toxicity | Muscular spasm and rigidity beginning at bite site and spreading proximally to abdomen and face; rebound tenderness mimicking acute appendicitis is possible | Arthralgias, fever, chills, maculopapular rash, nausea, vomiting |
| Potential associated signs of systemic toxicity | Arthralgias, bronchorrhea, regional or generalized diaphoresis, fever, hypertension, hyperreflexia, regional lymphadenopathy, nausea, vomiting, paresthesias, priapism, ptosis, restlessness, salivation | Febrile seizures, hemoglobinuria, myoglobinuria, acute renal failure |
| Outcomes of most bites | Resolution of all manifestations over 2 or 3 days; death rarely occurs | Most necrotizing ulcers will heal over 1 to 8 weeks with a 10% to 15% incidence of major scarring. One study found no deaths in 111 patients with entomologist-confirmed Loxosceles reclusa bites |
Most spider bites cause pain at the instant they occur. A hive-like swelling appears at the bite site and expands radially, usually for just a few centimeters ( Figs. 15.24 and 15.25 ![]() ); however, the swelling can sometimes reach gigantic proportions. Occasionally, two puncta or fang marks can be found on the skin surface. The warmth and deep erythema of a bite may resemble bacterial cellulitis, but the hive-like swelling and small, satellite hives are not characteristic of bacterial infection. A biopsy, although usually not necessary for diagnosis, may show mouth parts and intense inflammation. The lesion resolves spontaneously, but itching and swelling can be controlled with cool compresses and antihistamines.
); however, the swelling can sometimes reach gigantic proportions. Occasionally, two puncta or fang marks can be found on the skin surface. The warmth and deep erythema of a bite may resemble bacterial cellulitis, but the hive-like swelling and small, satellite hives are not characteristic of bacterial infection. A biopsy, although usually not necessary for diagnosis, may show mouth parts and intense inflammation. The lesion resolves spontaneously, but itching and swelling can be controlled with cool compresses and antihistamines.


Black Widow Spider
The syndrome latrodectism is characterized by painful muscle rigidity and autonomic disturbances such as tachycardia, hypertension, and diaphoresis. Symptoms typically last 1 to 3 days. Opioid analgesics combined with muscle relaxants, such as benzodiazepines, are only effective at symptomatic and temporary control. Antivenom is the most effective therapy.
The black widow spider, Latrodectus mactans (“shoe-button spider”), is so named because the female attacks and then consumes her mate shortly after copulation. The black widow is found in every state except Alaska and is especially numerous in the rural South. Several species are found in Europe.
Black widow spiders have a shiny, fat abdomen that looks like a big black grape or shoe button, with the longest legs extending out in front. There is a red hourglass marking on the underside of the abdomen. This marking may appear as triangles, spots, or an irregular blotch. Adult females have a total length of 4 cm ( Fig. 15.26 ) and are the only spiders capable of envenomation. The venom contains a neurotoxin, α-latrotoxin. It binds to specific receptors at the neuromuscular motor end plate of both sympathetic and parasympathetic nerves, resulting in increased synaptic concentrations of catecholamines. This results in clinically migratory muscle cramps and spasm, with nausea, vomiting, hypertension, weakness, malaise, and tremors, usually lasting from days to a week. Normally shy, black widow spiders are found in woodpiles, barns, and garages, but they migrate indoors, into closets and cupboards, during cold weather. They usually do not bite when away from the web because they are clumsy and need the web for support. The web has an unmistakable crinkling, crackling sound when it is disrupted.

Clinical Manifestations
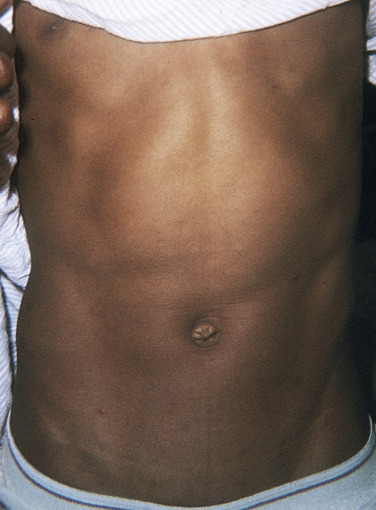
The bite may produce an immediate, sharp pain or may be painless. The subsequent reaction is minimal, with slight swelling and the appearance of a set of small, red fang marks. The symptoms that follow are caused by lymphatic absorption and vascular dissemination of the neurotoxin and are collectively known as latrodectism. The most common presenting complaints are generalized abdominal, back, and leg pain. Fifteen minutes to 2 hours after the bite, a dull muscle cramping or severe pain with numbness gradually spreads from the inoculation site to involve the entire torso but is usually more severe in the abdomen and legs. Any or all of the skeletal muscles may be involved. Severe abdominal pain and spasm simulating a surgical abdomen are the most prominent and distressing features of latrodectism ( Fig. 15.27 ![]() ). The abdominal muscles assume a board-like rigidity, but tenderness and distention usually do not occur. There is a generalized increase in the deep tendon reflexes. Other symptoms include dizziness, headache, sweating, nausea, and vomiting. The symptoms increase in severity for several hours (up to 24 hours), slowly subsiding and gradually decreasing in severity in 2 or 3 days. Residual symptoms such as weakness, tingling, nervousness, and transient muscle spasm may persist for weeks or months after recovery from the acute stage. Recovery from one serious attack usually offers complete systemic immunity to subsequent bites. Convulsions, paralysis, shock, and death occur in approximately 5% of cases, usually in the young or the debilitated elderly. There are reports of priapism from widow spider bites that implicate direct venom action on blood vessels, leading to venous engorgement of the penis.
). The abdominal muscles assume a board-like rigidity, but tenderness and distention usually do not occur. There is a generalized increase in the deep tendon reflexes. Other symptoms include dizziness, headache, sweating, nausea, and vomiting. The symptoms increase in severity for several hours (up to 24 hours), slowly subsiding and gradually decreasing in severity in 2 or 3 days. Residual symptoms such as weakness, tingling, nervousness, and transient muscle spasm may persist for weeks or months after recovery from the acute stage. Recovery from one serious attack usually offers complete systemic immunity to subsequent bites. Convulsions, paralysis, shock, and death occur in approximately 5% of cases, usually in the young or the debilitated elderly. There are reports of priapism from widow spider bites that implicate direct venom action on blood vessels, leading to venous engorgement of the penis.
Treatment
Immediate First Aid.
If the patient is seen within a few minutes of being bitten, ice may be applied to the bite site to help restrict the spread of venom. Pain relief is achieved either with black widow spider–specific antivenin alone or with a combination of intravenous (IV) opioids and muscle relaxants. Healthy patients between ages 16 and 60 years usually respond to muscle relaxants and recover spontaneously. In emergencies, the local or state poison center or the Department of Public Health may be called for information about the closest source of antivenin.
Antivenin.
The only therapies with proven effectiveness are opioid analgesics and black widow spider antivenin. Antivenin Latrodectus mactans is an equine-derived antivenom based on immunoglobulin G (IgG). The proposed pharmacologic mechanism is binding of venom toxic constituents by the antivenin antibodies. A single vial (2.5 mL) generally provides adequate relief in human (adult or pediatric) poisoning cases. Patients treated with antivenin experience a much shorter duration of symptoms and are less likely to be admitted to the hospital than those who do not receive antivenin. Relief of symptoms occurs within an average of 31 minutes of antivenin infusion. Administration of antivenin even late in the course of envenomation is effective. One ampule is sufficient. The administration of antivenin to patients with prolonged or refractory symptoms of latrodectism, even after 90 hours after a bite, may alleviate discomfort and weakness.
Acute hypersensitivity reactions are the most feared complication. Although these reactions do occur, relatively few minor reactions have been reported. The package insert for antivenin Latrodectus mactans calls for infusion of diluted antivenin during a period of 15 to 30 minutes. At these slower infusion rates, immediate hypersensitivity is rare. Patients may be pretreated with diphenhydramine and/or steroids in an attempt to blunt a hypersensitivity response. Multiple allergies, asthma, or past reactions to equine-based products should be considered contraindications.
Muscle Relaxants.
Although calcium gluconate was once the first-line treatment of severe envenomations, it was found in one large series to be ineffective for pain relief compared with a combination of IV opioids and benzodiazepines. Intravenous diazepam may be used and later replaced with diazepam pills. Alternatively, diazepam or 1 or 2 g of methocarbamol (100 mg/mL in 10-mL vials) may be administered undiluted over 5 to 10 minutes. Oral doses may be used thereafter, and they usually sustain the relief initiated by the injection.
Analgesics.
Aspirin or, if pain is severe, IV morphine may be given. Morphine should be used with caution, since the venom is a neurotoxin and may cause respiratory paralysis.
Brown Recluse Spider
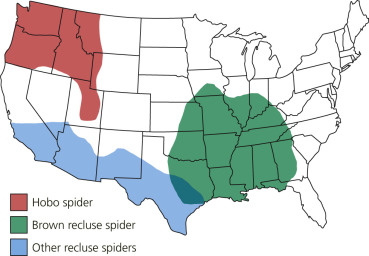
The brown recluse spider, Loxosceles reclusa (“fiddle-back spider”), is small, approximately 1.5 cm in overall length. Its color ranges from yellowish tan to dark brown. A characteristic dark, violin- or fiddle-shaped marking is located on the spider’s back. The broad base of the violin is near the head and the violin stem points toward the abdomen ( Fig. 15.28 ). The spider is a timid recluse, avoiding light and disturbances and living in dark areas (under woodpiles and rocks and inside human habitations, often in closets, behind picture frames, under porches, and in barns and basements). Its web is small, haphazard, and woven in cracks, crevices, or corners. It bites only when forced into contact with the skin, such as when a person puts on clothing in which the spider is residing or rummages through stored material harboring the spider. The brown recluse is usually found in the southern half of the United States, but some have been found as far north as Connecticut. The hobo spider, Tegenaria agrestis, has been implicated in necrotic lesions in the Pacific Northwest of the United States ( Fig. 15.29 ![]() ).
).

Clinical Manifestations
Patients infrequently present with a spider for positive identification. Overdiagnosis of brown recluse spider bites has led to harmful sequelae and misdiagnosis. Many patients currently present with a “spider bite,” but on investigation they have community-acquired methicillin-resistant Staphylococcus aureus (MRSA). There is no laboratory test for diagnosis. A summary of bite severity and treatment is found in Table 15.5 . Brown recluse spider bites frequently induce necrotic, slowly healing lesions. Maximum lesion severity is a predictor of time to complete healing. Most bites are on an extremity. The bite produces a minor stinging or burning sensation or an instantaneous sharp pain resembling a bee sting. Most bite reactions are mild and cause only minimal swelling and erythema. Site location seems to be a factor in the severity of the local bite reaction; fatty areas such as the proximal thigh and buttocks show more cutaneous reaction. Severe bites may become necrotic within 4 hours.
| Severity | Clinical Appearance/Signs | Symptoms | Treatment |
|---|---|---|---|
| Mild | Erythema, punctum, no necrosis | Pruritus | RICE, antihistamine, aspirin, tetanus vaccine |
| Moderate | Erythema, mild edema, vesicle, necrosis <1 cm 2 | Pain, other | Add analgesic, antibiotic; consider dapsone |
| Severe | Erythema, edema, (hemorrhagic) bullae, ulcer, necrosis >1 cm 2 | Pain, other | Add dapsone 50 mg PO daily, then 50 mg bid; order G6PD |
| Systemic * | Rash, fever, hemolysis, thrombocytopenia, DIC | Myalgia, headache, malaise, nausea | Support; serial CBC and U/A, vigorous hydration, systemic steroids, transfusion |
* Systemic symptoms are possible with bites of all cutaneous severity.
The first and most characteristic cutaneous change in necrotic arachnidism, or loxoscelism, is the development and rapid expansion of a blue-gray, macular halo around the puncture site; this halo represents local hemolysis. Violaceous skin discoloration is an indication of incipient necrosis and can be used as a guide to early initiation of therapy, when it is most effective. A cyanotic pustule or vesicle/bulla may also appear at the bite site. The lesion may have an oblong, irregular configuration area at the bite site and a sudden increase in tenderness. At this stage, the superficial skin may be rapidly infarcting and the pain is severe. The necrotizing, blue macule widens and the center sinks below the normal skin surface (“sinking infarct”) ( Fig. 15.30 ). The extent of the infarct is variable. Most patients experience localized reactions, but the depth of the necrotic tissue may extend to the muscle and over broad areas of skin, sometimes involving most of an extremity. The dead tissue sloughs, leaving a deep, indolent ulcer with ragged edges. Ulcers take weeks or months to heal; scarring is significant.

A severe, progressive reaction that begins with moderate to severe pain at the bite site develops in a few people. Within 4 hours, the pain is unbearable and the initial erythema gives way to pallor. Within 12 to 14 hours after the bite, the victims often experience fever, chills, nausea, vomiting, weakness, joint and muscle pains, and hives or measle-like rashes. The toxin may produce severe systemic reactions such as thrombocytopenia or hemolytic anemia with generalized hemolysis, disseminated intravascular coagulation, renal failure, and sometimes death. Severe systemic reactions are rare and occur most frequently in children. Serial complete blood cell counts should be analyzed for hemolysis, thrombocytopenia, and leukocytosis. Serial urinalyses evaluate the possibility of hemoglobinuria.
A bite during pregnancy does not appear to lead to unusual risks to mother or fetus.
Management
Experience has shown that most bites are mild and should be treated conservatively with the following measures:
- 1.
Bite sites are treated with RICE (Rest, Ice, Compresses [15 minutes each hour], Elevation).
- 2.
An aspirin a day helps counteract platelet aggregation and thrombosis.
- 3.
Tetanus toxoid is given if necessary.
Moderate to Severe Skin Necrosis.
Serious bites are usually obvious within the first 24 to 48 hours and need medical, but not surgically aggressive, treatment.
- •
Antibiotics (e.g., cephalosporins) should be used as infection prophylaxis in ulcerating lesions. Secondary infection increases localized skin temperature that raises enzymatic activity and leads to further tissue damage; therefore routine use of antibiotics is suggested.
- •
Analgesics are usually required.
Dapsone.
Immediate surgical excision of brown recluse bite sites induced more complications than did the use of dapsone with or without delayed excision and/or repair. Dapsone 50 to 200 mg/day may be helpful in severe cutaneous reactions to prevent extensive necrosis, even if it is administered 48 hours after the bite. Dapsone may help prevent the venom-induced perivasculitis with polymorphonuclear leukocyte infiltration that occurs with extensive cutaneous necrosis. Order a glucose-6-phosphate dehydrogenase level and complete blood cell count.
Steroids.
There is little evidence that oral and intralesional steroids decrease the severity of the progressive reaction. Patients with necrosis greater than 1 cm should be tested to see if progressive hemolytic anemia, manifested by an increasing level of free serum hemoglobin or thrombocytopenia, has developed. Severe systemic loxoscelism may be treated with prednisone (1 mg/kg) given as early as possible in the development of systemic symptoms to treat hematologic abnormalities.
Surgery.
Early excision of necrotic areas was once thought to help prevent the spread of the toxin and further necrosis. This practice is probably ineffective and should be discouraged. If a brown recluse spider bite does not become clinically necrotic within 72 hours, a serious wound healing problem rarely develops.
Sharp debridement or excision of spider bite lesions should be vigorously discouraged. Gentle eschar removal may be performed after the wound has stabilized and inflammation has subsided (approximately 6 to 10 weeks). Surgery is reserved for debridement of necrotic lesions.
Antivenin.
No commercial antivenin is available in the United States. A horse-derived antivenin is available in some countries. Inquire about availability in United States.
Ticks
Ticks are blood-sucking ectoparasites that act as vectors for rickettsial, spirochetal, bacterial, and parasitic infections. Adult ticks of some species can reach 1 cm in length; they have eight legs, and the front two are curved forward, as in crabs. The large oval or teardrop-shaped body is flat and sac-like and has a leathery outer surface. There are two families of ticks: hard-bodied ticks (Ixodidae) and soft-bodied ticks (Argasidae). They are distinguished by the consistency of their bodies. Hard (ixodid) ticks are of greatest concern because they are vectors for most of the serious tickborne diseases. They can inflict local reactions such as pain, erythema, and nodules, and they are more difficult to remove than the soft (argasid) ticks. Ticks should be removed from the host as soon as possible after they are discovered to reduce the chance of infection. Proper removal of the tick, however, is just as important in reducing the chance of infection as timely removal.
Ticks perch on grass tips and bushes and wait for a warm-blooded host to pass by. They insert their recurved teeth into the skin, produce a glue-like secretion that tightens their grip, suck blood ( Fig. 15.31 ), and become engorged, sometimes tripling in size. Hard ticks may remain attached to the host for up to 10 days, whereas soft ticks release in a few hours. The bite itself is painless, but within hours an urticarial wheal appears at the puncture site and may cause itching. Ticks may go unnoticed, particularly in children, for several hours after attachment to an inconspicuous area such as the scalp.

Ticks and their associated diseases are listed in Table 15.6 .
| Disease | Clinical Presentation | General Laboratory Findings and Diagnosis | Treatment |
|---|---|---|---|
| Anaplasmosis |
| General findings:
Diagnosis:
|
|
| Babesiosis |
| General findings:
Diagnosis:
|
|
| Borrelia miyamotoi disease |
| General findings:
Diagnosis:
|
|
| Colorado tick fever (CTF) |
| General findings:
Diagnosis:
|
|
| Ehrlichiosis |
| General findings:
Diagnosis:
|
|
| Heartland virus disease |
| General findings:
Diagnosis:
|
|
| Lyme disease |
| General findings:
Diagnosis:
|
|
| Powassan virus disease |
| General findings:
Diagnosis:
|
|
| Rocky Mountain spotted fever (RMSF) |
| General findings:
Diagnosis:
|
|
| Rickettsia parkeri rickettsiosis |
| General findings:
Diagnosis:
|
|
| Tick-borne relapsing fever (TBRF) |
| General findings:
Diagnosis:
|
|
| Tularemia |
| General findings:
Diagnosis:
|
|
| African tick-bite fever (ATBF) |
| General findings:
Diagnosis:
|
|
| Tick-borne encephalitis (TBE) |
| General findings:
Diagnosis:
|
|
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


