Indications and Techniques for Subcutaneous Lateral Brow Lifting
Richard J. Warren
DEFINITION
Lateral brow ptosis describes an abnormally low position of the lateral third to one-half of the eyebrow complex.
Brow position and shape convey an impression of emotion. When the lateral portion of the brow turns down, the patient appears sad or melancholy. It is also associated with aging.1
Ptosis of the lateral eyebrow encroaches on the upper lid sulcus, changing the dynamics of the upper lid/brow junction. Thus, lateral brow ptosis will affect the assessment of patients who present for blepharoplasty, periorbital fat grafting, or senile eyelid ptosis repair.
ANATOMY
Please refer to the anatomy section of the coronal brow lift chapter.
The position of the lateral brow depends on two main issues: muscle anatomy and the firmness of soft tissue attachment.
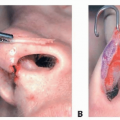
The level of the lateral eyebrow is the result of a balancing act between the muscular forces that elevate the brow and the muscular forces that depress the brow, along with the universal depressor, gravity (FIG 1).
The frontalis is the only elevator of the eyebrow. It originates from the galea aponeurotica superiorly and interdigitates inferiorly with the upper orbicularis. Contraction raises this muscle mass and the overlying eyebrow, which is a cutaneous structure. The muscle is deficient laterally and nonexistent lateral to the temporal crest line, so its primary lifting effect is exerted on the medial and central portions of the eyebrow.
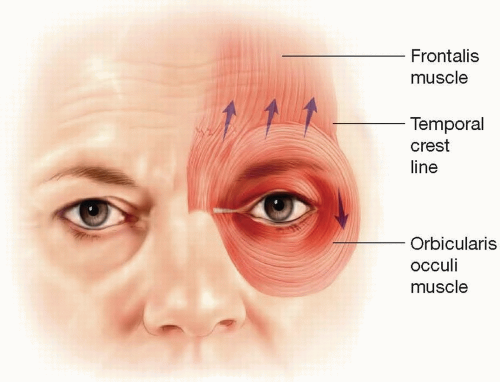
FIG 1 • The frontalis is the only muscle which lifts the eyebrow complex. On contraction, most of the movement occurs in the lower third of the muscle, and this action is strongest in the medial and central eyebrow. Laterally, frontalis action is weaker and is completely absent lateral to the temporal crest line. The orbicularis oculi acts like a sphincter surrounding the orbit. Laterally, it pulls the tail of the brow inferiorly.
The primary muscular depressor of the lateral eyebrow is the orbicularis that encircles the orbit acting like a sphincter. Its action on the lateral brow can be temporarily reversed with botulinum toxin.
Sensory Nerves
Innervation to the lateral brow and forehead is supplied by the supraorbital nerve that divides into two segments after it exits the orbit: the superficial and the deep branches.
The superficial branches of the supraorbital nerve run on the superficial surface of the frontalis muscle and are visible when a subcutaneous flap is raised. These nerves innervate the forehead and the first 2 cm of the hair-bearing scalp. The rest of the scalp, back to the vertex, is innervated by the deep branch that courses laterally and is deep to the frontalis muscle.
Motor Nerves
The temporal branch of the facial nerve crosses the middle third of the zygomatic arch as two or three branches. These branches are entirely deep to the frontalis muscle and are on the underside of the superficial temporal fascia. Therefore, they are completely safe during the raising of a subcutaneous forehead skin flap.
Vessels
The anterior branch of the temporal artery and accompanying veins coursing superficial to the frontalis muscle and the superficial temporal fascia. These may require cauterization during the raising of a subcutaneous forehead flap.
PATHOGENESIS
Please refer to the pathogenesis of eyebrow ptosis in the coronal brow chapter.
The desired eyebrow shape and position vary with ethnicity, gender, and the era in which we live. In this era, the elevated lateral eyebrow is the preferred configuration with the lateral end of the eyebrow ideally being higher than the medial end.
As mentioned, the lateral portion of the eyebrow has two causes for inferior displacement (lateral orbicularis contraction and gravity) balanced against the only force that
can lift: the frontalis. Despite this apparent imbalance, many patients (40% in one study) do not develop lateral brow ptosis over time.2 The likely explanation for their brow stability is the strength of the underlying soft tissue attachments.
Soft tissue fixation to bone is inconsistent in the lateral eyebrow. Laterally along the supraorbital rim, the galeal fat pad is separated from the preseptal fat (ROOF, retro orbicularis oculi fat) by one of the layers of galea. However, in the lateral brow, this galeal layer is thought to be variable, with some individuals having limited soft tissue attachment to bone. As a result, the galeal fat pad is contiguous with the preseptal fat (ROOF), and the lateral brow is relatively free to descend over time.3
Many patients who develop lateral brow ptosis do so as a relatively early sign of facial aging.
PATIENT HISTORY AND PHYSICAL FINDINGS
Please refer to the patient history and physical examination in the coronal brow chapter (Chapter 20).
Patients with lateral brow ptosis may present with a request for upper eyelid blepharoplasty, or they may request a facelift procedure, hoping it will improve their brow position. Both scenarios provide the surgeon with an opportunity to teach the patient about the dynamics of eyebrow aging.
The laxity of the lateral forehead skin is assessed by manually manipulating the tail of the brow. Patients best suited for a subcutaneous lateral brow lift are those with loose skin and a relatively lax attachment between their lateral forehead skin and the underlying frontalis and superficial temporal fascia.
The eyebrow itself is a cutaneous structure, and shifting the deep plane tissues with a deeper procedure may not translate well to the overlying skin if that skin is loose. Conversely, a successful procedure to shift the skin will directly shift the eyebrow.
The ptotic lateral eyebrow is a common physical finding in the patient demographic who seek facial rejuvenation surgery. Consequently, a subcutaneous lateral brow lift can be an excellent adjunctive procedure for the patient who is a candidate for a facelift or blepharoplasty (FIG 2).

FIG 2 • This 56-year-old woman presents for blepharoplasty and facelift surgery. She has downturned lateral eyebrows that were not present in youth. The position of her medial and central brow is well maintained. In conjunction with the procedures she is requesting, a repositioning of the lateral eyebrows will be a useful adjunctive procedure.
An examination of the temporal hairline will often demonstrate a triangular widow’s peak where the hair is thin; this can be an ideal area to extend a hairline incision into the peak laterally.
NONOPERATIVE MANAGEMENT
Nonoperative strategies to elevate the lateral eyebrow include the following:
Nonmedical: eyebrow plucking, cosmetic makeup, tattooing
Medical: botulinum toxin injection to the lateral orbicularis and the medial brow depressors, thread lifting
SURGICAL MANAGEMENT
Preoperative Planning
The planned repositioning and degree of eyebrow elevation are reviewed with the patient who may have specific requests regarding eyebrow position and shape.
The location of the hairline will affect the incision planning. The normal hairline will lend itself to an incision along the anterior hairline in the widow’s peak area. Patients with a low hairline may benefit from an incision behind the hairline, which will shift the anterior hairline posteriorly. Patients in whom the temple hairline is positioned above (superior to) the lateral eyebrow may benefit from an incision placed in the temple hair.
The presence of transverse forehead lines and the quality of forehead skin is assessed. The patient with thick corrugated skin may benefit from an incision made in a transverse forehead crease. This is often the case with middle age or older men.
With the patient awake in the upright position and the forehead in repose, the desired amount and direction of lateral eyebrow elevation are assessed by manually elevating the lateral eyebrow. A mark is made on the skin, and the eyebrow is allowed to drop, thus determining the degree of elevation required.
The most effective vector for eyebrow advancement is determined when the examiner manually repositions the brow. Most commonly, the desired vector runs along the axis of the temporal crest line.
Positioning
The patient is placed on the operating table in the supine position with the head on a small pillow or soft donut.
The head of the bead is raised slightly to help reduce venous engorgement.
Approach
As described for preoperative planning, possible locations for subcutaneous lateral brow lifting are
At the hairline
Just behind the hairline
Lateral extension of a transverse forehead line
Directly adjacent to the eyebrow (FIG 3)
All of these approaches are “skin deep” with varying degrees of subcutaneous dissection. For the first three incisions (hairline, behind the hairline, transverse forehead line), the dissection plane is subcutaneous, immediately superficial to the frontalis muscle. In the fourth option (adjacent to eyebrow), there is no skin undermining.
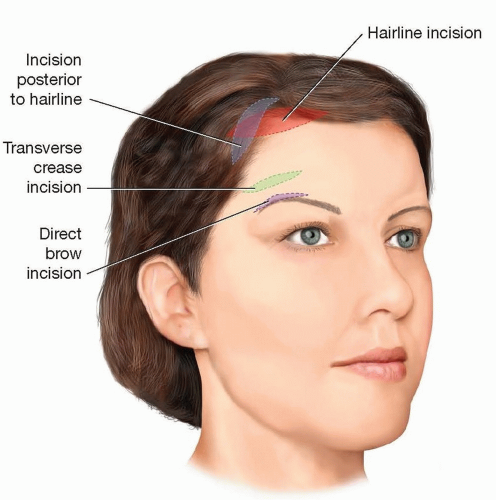
FIG 3 • Incision options for subcutaneous brow lifting are shown. An incision posterior to the hairline involves the removal of hair-bearing skin posterior to the incision. An incision at the hairline involves the removal of forehead skin inferior to the incision. The transverse crease incision involves subcutaneous dissection on the eyebrow side of the incision, with skin excision on the inferior side of the crease. The direct brow incision does not involve undermining. The ideal vector for lateral eyebrow lifting is shown. This will be slightly different in every case but typically will follow the temporal crest line.Related posts:
 Injection of Botulinum Toxin to the Depressor Anguli Oris
Injection of Botulinum Toxin to the Depressor Anguli Oris
 Indications and Technique for Skin Pinch Skin Excision in the Lower Eyelids
Indications and Technique for Skin Pinch Skin Excision in the Lower Eyelids
 Indications and Techniques for Upper and Lower Blepharoplasty With Microfat Injections
Indications and Techniques for Upper and Lower Blepharoplasty With Microfat Injections
 Indications and Techniques for Buccal Fat Pad Excision
Indications and Techniques for Buccal Fat Pad Excision
 Technique for Treating the Long Nose
Technique for Treating the Long Nose
 Alar Contour Grafts
Alar Contour Grafts

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access
