Indications and Technique for Transconjunctival Fat Removal and Redraping in the Lower Eyelids
Francisco G. Bravo
DEFINITION
Patients with good skin quality who present with prominent lower eyelid bags and evident nasojugal and palpebromalar grooves may benefit from transconjunctival fat removal and redraping of excess fat over the inferior orbital rim.1,2,3,4
This procedure avoids the need for external incisions, which may be visible in younger patients and may be associated with a higher incidence of complications such as lower lid retraction, scleral show, and prolonged swelling.
The need for routine use of canthal support techniques is also generally avoided through this approach.
A recessed lower orbital rim and an evident tear trough deformity may be augmented and attenuated, respectively, with the patient’s own prominent lower eyelid bags without the need for fat grafting or synthetic filler injections.
ANATOMY
Skin and the orbicularis oculi muscle form the anterior lamella.
The orbital septum, orbital fat, and suborbicularis adipose tissue form the middle lamella.
The tarsal plate, lower eyelid retractors (capsulopalpebral head and fascia), and the conjunctiva form the posterior lamella.
The orbicularis oculi muscle is subdivided into the pretarsal, preseptal, and orbital components.
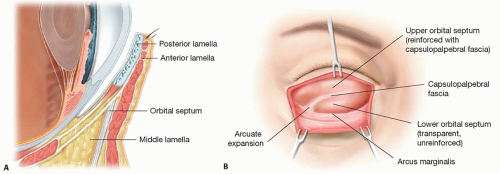
FIG 1 • A. The lower eyelid consists of an anterior, middle, and posterior lamella. B. There are three postseptal fat compartments in the lower eyelid.
There are three postseptal fat compartments in the lower eyelid (FIG 1B).
Nasal and central fat pads are separated by the inferior oblique muscle.
Central and lateral fat pads are separated by the arcuate expansion of the Lockwood ligament (FIG 1C).
The orbicularis retaining ligament or orbitomalar ligament attaches the palpebral orbicularis oculi muscle to the underlying maxilla (FIG 2A).
PATIENT HISTORY AND PHYSICAL FINDINGS
The preoperative evaluation for patients seeking lower eyelid surgery includes a detailed assessment of the patient’s medical history and a thorough physical examination.7
Medical history
Special attention should be paid to risk factors that may predispose to postoperative complications.
Thyroid pathology, diabetes, hypertension, heart disease, coagulopathy, and any previous periorbital surgery or trauma should be documented.
Vision disorders such as impaired visual acuity or the need to use corrective glasses or contact lenses should be noted before surgery.
The use of medications such as aspirin and other nonsteroidal anti-inflammatory drugs, anticoagulants, and
certain vitamins and herbal supplements such as vitamin E and ginkgo should be recorded and suspended 2 weeks prior to surgery.
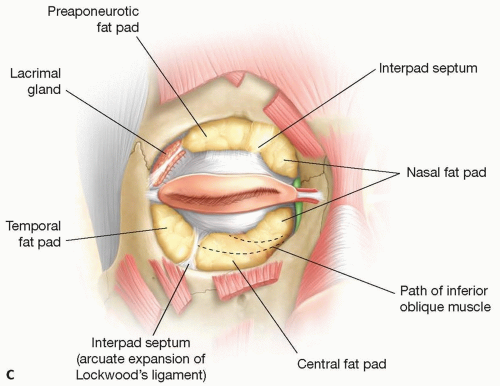
FIG 1 (Continued) • C. Central and lateral fat pads are separated by the arcuate expansion of the Lockwood ligament.
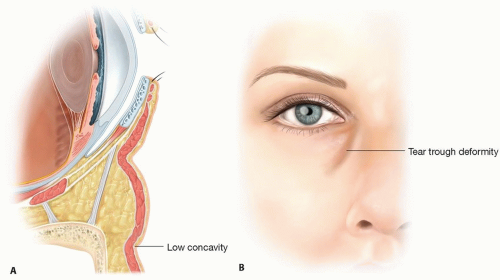
FIG 2 • A. The orbicularis retaining ligament or orbitomalar ligament attaches the palpebral orbicularis oculi muscle to the underlying maxilla. B. The tear trough or nasojugal groove and the lid-cheek junction or palpebromalar groove extend below the orbital rim and are explained by anatomical features in the subcutaneous plane.
Smoking history should also be documented and interrupted preferably for 4 weeks prior and 2 weeks after surgery.
A history suggestive of dry eye syndrome should be clarified, and if present, the decision to proceed should be discussed carefully with the patient.
Physical examination
Evaluation should be performed with three goals in mind:
To document preoperative eye function
To identify anatomical features that may predispose patients to developing postoperative complications
To identify the specific anatomical features that are causing the patient’s concern in order to customize the procedure
Functional evaluation should include an examination and documentation of visual acuity, extraocular muscular movements, Bell phenomenon, pupillary response, and adequate tear production through a Schirmer or tear break-apart time test.7
Anatomic features that may predispose to postoperative complications such as lower eyelid retraction, ectropion, or malposition8 include the following:
A negative vector caused by a prominent eye or a retruded maxilla, which may be measured by a Hertel exophthalmometer
Tarsoligamentous or horizontal lid margin laxity with a measurable lag in the snapback test and a greater than 6-mm distraction test
A negative canthal tilt in which the lateral canthus lies at a lower position in relationship to the medial canthus
Scleral show in which the lid margin rests below the corneoscleral limbus
Specific anatomic features9,10 that need to be identified as possible causes of the morphological concerns the patient might wish to address are as follows:
Orbital fat herniation or prolapse due to fat pad hypertrophy or to excessive laxity of the orbital septum and orbicularis oculi muscle
Tear trough deformity and a deep lid-cheek junction
Dark circles due to skin pigmentation or prominent intramuscular vasculature in patients with thin, translucent skin and subcutaneous fat atrophy
Dermatochalasis or skin excess and rhytides
Orbicularis prominence or hypertrophy
Malar bags and festoons
IMAGING
The use of high-quality preoperative photography is a key element to plan and carry out eyelid surgery, as well as to document and serve as reference for clinical examination.
Standardization in patient positioning, lighting, lens focal length, and background is crucial to avoid misinterpretation and distortion of the patient’s anatomic features.11
The photographic series should include frontal, oblique, and profile views (FIG 3), as well as frontal views while smiling, rising the eyebrows, frowning, gazing upward, closing the eyes, and also with slight posterior and anterior head tilts while looking into the lens.
High-quality video capture should also be considered to appropriately document ocular and eyelid function preoperatively.
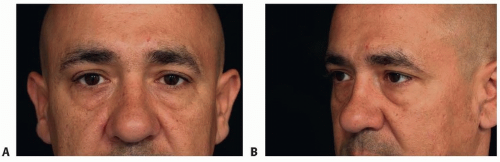
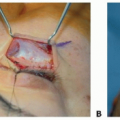
FIG 3 • A. Preoperative frontal. B. Preoperative three-quarters views of a male patient with protruding eyelid bags and marked nasojugal and palpebromalar grooves.
Digital imaging software may be an important adjunct to precisely evaluate eyelid morphology and to detect asymmetries, which are common in the lower eyelid.12
NONOPERATIVE MANAGEMENT
With the popularity and appeal of noninvasive procedures among cosmetic surgery patients, a thorough and earnest discussion should be maintained regarding the advantages and disadvantages of such techniques versus surgical options by attending to the patient’s particular anatomic features and concerns.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree