Fig. 26.1
(a) Clinical appearance of SPD-type IgA pemphigus and (b) IEN-type IgA pemphigus
26.4 Histopathology
Histopathologically, most IgA pemphigus skin lesions show minimal acantholysis [12]. In the SPD-type IgA pemphigus, pustules are observed at the subcorneal upper epidermis (Fig. 26.2a), while in the IEN-type IgA pemphigus, neutrophilic infiltration is observed throughout the entire epidermis (Fig. 26.2b) [1, 9]. These neutrophilic pustules are the hallmarks of IgA pemphigus.
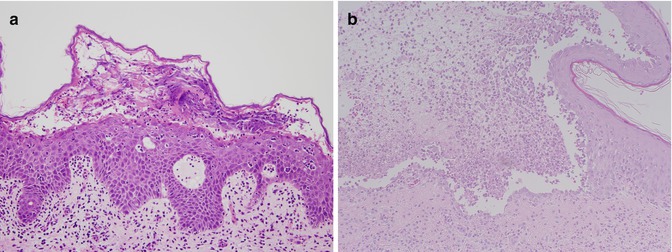
Fig. 26.2
(a) Histopathological features of SPD-type IgA pemphigus and (b) IEN-type IgA pemphigus
26.5 Electron Microscopy
The autoantigen in IgA pemphigus was analyzed by immunoelectron microscopy. In SPD-type IgA pemphigus, autoantibodies react with the extracellular space of desmosomes, which corresponds to the localization of desmocollin-1 (Fig. 26.3a, b) [13]. In contrast, in IEN-type IgA pemphigus, autoantibodies react with the extracellular space of inter-desmosomal areas of the cell membrane (Fig. 26.3c, d) [13, 14]. Therefore, the target molecule of IEN-type IgA pemphigus does not seem to be a desmosomal protein but may be adherens junction-related molecules.
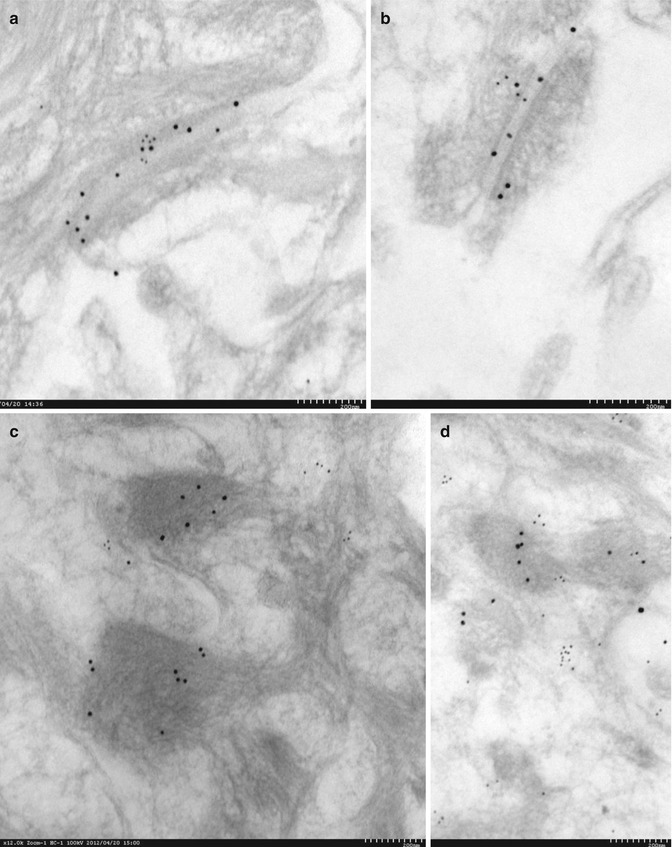
Fig. 26.3
(a, b) Results of immuneoelectron microscopic study of SPD-type IgA pemphigus and (c, d) IEN-type IgA pemphigus: 10 nm gold label, patient’s senrun: 15 nm gold label, desmocollin
26.6 Immunofluorescence
In direct immunofluorescence using perilesional patient skin section, IgA deposition in the cell surface of the keratinocytes was observed [1, 9]. IgG or C3 deposition is occasionally observed but is weaker than IgA deposition [1, 9]. In indirect immunofluorescence using patient sera and various substrates, including normal human skin, monkey esophagus, or other epithelia, circulating IgA anti-keratinocyte cell surface antibodies are detected in some sera [1, 9].
IgA antibodies in SPD-type IgA pemphigus react with keratinocyte cell surface in the uppermost epidermis, where desmocollin-1 exists (Fig. 26.4a). In contrast, IgA antibodies in IEN-type IgA pemphigus react with the whole epidermis (Fig. 26.4b).
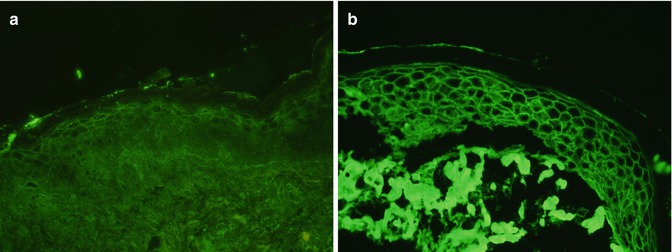
Fig. 26.4
(a) Direct immunofluorescence features of SPD-type IgA pemphigus. (b) Direct immunofluorescence features of SPD-type IgA pemphigus
In addition, cultured COS7 cells transfected with cDNA vectors for human desmocollin, 1–3 are used as substrates for indirect immunofluorescence study to detect autoantibodies to desmocollin, 1–3 [15–18]. By this method, IgA antibodies of SPD-type but not IEN-type IgA pemphigus show positive signal exclusively with desmocollin-1 obtained as dotted fluorescent signals (Fig. 26.5a), while IgA antibodies in IEN-type IgA pemphigus do not react with any desmocollins (Fig. 26.5b).
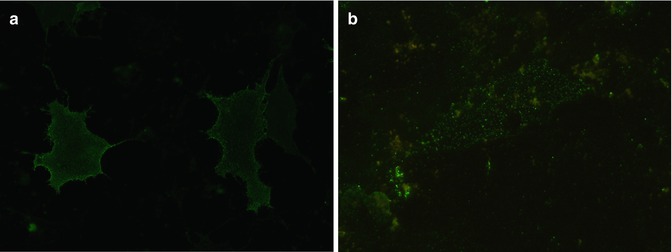
Fig. 26.5
(a) Positive IgA reactivity of SPD-type IgA pemphigus to cell surfaces of COS7 cells transfected with cDNA of human desmocollin-1. (b) IEN-type IgA pemphigus does not react with any desmocollins
26.7 Enzyme-Linked Immunosorbent Assay (ELISA) for Immunodiagnosis
ELISA for desmogleins and desmocollins is available for the diagnosis of IgA pemphigus. Some particular IgA pemphigus patients occasionally show IgA autoantibodies to either desmoglein-1 or desmoglein-3 in ELISA [17]. The usefulness of ELISA using baculovirus-producing recombinant proteins of desmocollins was questionable in terms of both specificity and sensitivity [3]. We have recently established a novel ELISA using eukaryotic recombinant Dsc proteins, which showed the results consistent to those by a cDNA transfection study (Kwesi et al. in preparation).
26.8 Immunoblotting
Immunoblotting of normal human epidermal extract is not useful for the diagnosis of IgA pemphigus, in contrast to that of other autoimmune bullous diseases.
26.9 Pathophysiology
The autoantigen is desmocollin-1 in SPD-type IgA pemphigus. IgA antibodies to desmoglein-1 and desmoglein-3 were found in rare types of IgA pemphigus foliaceus and IgA pemphigus vulgaris, respectively [13, 15, 19–21]. However, autoantigens for most cases of IEN-type IgA pemphigus were unknown.
The pathogenesis of IgA pemphigus is unknown, but a few reports suggest some mechanisms for the initiation of skin lesions in IgA pemphigus. Activation of interleukin-5 and involvement of γδT cells are reported in IgA pemphigus [9, 14]. In addition, binding of IgA antibodies to IgA-Fc receptor, CD89, is considered to cause neutrophil accumulation and proteolytic cleavage of the keratinocyte cell-cell junction in IgA pemphigus [22]. However, there have been no direct evidences of acantholysis caused by IgA autoantibodies in IgA pemphigus.
26.10 Associated Diseases
Chronic inflammation in IgA pemphigus may enhance the development of cancers. IgA pemphigus is reported to be associated with internal malignancies, particularly IgA gammopathy and lung cancer [23].
The other complications for IgA pemphigus are disease- or treatment-related infections. Disease-related infections occur in the blister and erosion, whereas treatment-related infections occur from systemic immunosuppressions by oral steroids or other immunosuppressants [9].
26.11 Prognosis
26.12 Treatment
IgA pemphigus is mainly treated by oral and topical corticosteroids [24]. Corticosteroids can decrease inflammation by reversing increased capillary permeability and suppressing neutrophil activity [25, 26]. In addition, corticosteroids stabilize lysosomal membranes and, therefore, can suppress lymphocytes and antibody production [27]. In addition to corticosteroids, dapsone, isotretinoin, acitretin, mycophenolate mofetil, and adalimumab are also reported useful in treating IgA pemphigus [1, 15, 28–30].
Related posts:
 Kindlin-1 and Its Role in Kindler Syndrome
Kindlin-1 and Its Role in Kindler Syndrome
 Cyclophosphamide in Autoimmune Blistering Diseases: Safety, Efficacy and Evidence Base
Management of Bullous Systemic Lupus Erythematosus
Cyclophosphamide in Autoimmune Blistering Diseases: Safety, Efficacy and Evidence Base
Management of Bullous Systemic Lupus Erythematosus
 Using Intravenous Immunoglobulins in Autoimmune Bullous Diseases
Using Intravenous Immunoglobulins in Autoimmune Bullous Diseases
 Living with Epidermolysis Bullosa: Reviewing the Impact on Individuals’ Quality of Life
Living with Epidermolysis Bullosa: Reviewing the Impact on Individuals’ Quality of Life
 How to Take a Skin Biopsy Correctly to Diagnose Epidermolysis Bullosa and Autoimmune Bullous Diseases
How to Take a Skin Biopsy Correctly to Diagnose Epidermolysis Bullosa and Autoimmune Bullous Diseases
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


