Hypopigmented Scars
Rebecca Baxt
Euphemia W. Mu
BACKGROUND
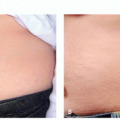
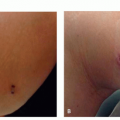
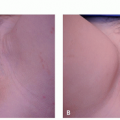
Scars or cicatrices are the end result of wound healing following disease or trauma.1 These skin defects exhibit great variation in characteristics, such as pigmentation, thickness, pliability, and vascularity.2 Hypopigmented scars are among the most common (Figure 2.3.1). Studies have documented the psychosocial impact hypopigmented scars can have on patients including distress and social isolation.3,4 As no 2 hypopigmented scars are exactly alike, the study and treatment of these scars have proved challenging. This chapter will discuss the etiology, pathogenesis, and treatment of hypopigmented scars.
PRESENTATION
Patients present with a complaint of white or light marks or scars after injury, a skin condition, or a treatment. Patients complain of an area of loss of pigment to the skin. In hypopigmented scars, these areas are usually associated with a textural change, such as overgrowth of tissue or atrophy.
DIAGNOSIS
Clinical Diagnosis
On clinical examination, a hypopigmented scar is a depigmented or hypopigmented patch or plaque in a shape that is suggestive of trauma, such as linear. In the majority of cases, a textural change, such as atrophy or hypertrophy, is associated with the pigmentary change.
As compared with keloids or hypertrophic scars, hypopigmented scars are patches or plaques that are less pigmented than the surrounding skin. The surface change may be minimal or pronounced. Hypopigmented surgical scars are covered in chapter 8.1; keloids and hypertrophic scars in chapter 8.2; burn scars in chapter 8.3, and acne scars in chapter 8.4. Vitiligo is covered in chapter 2.1. Idiopathic guttate hypomelanosis is covered in chapter 2.2.
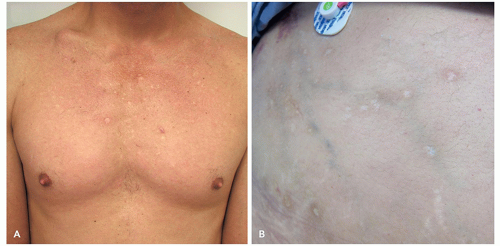 FIGURE 2.3.1 Hypopigmented scars are skin defects resulting from wound healing following disease or trauma. Hypopigmented scars due to acne (A) and surgery (B). |
Histopathology
The loss or destruction of hair follicles has been suggested as a cause of the common hypopigmentation seen in incisional epidermal scars.5 In contrast, immunohistochemical investigations with melanocyte markers and Fontana-Masson silver stain comparing scars with normal skin demonstrated normal numbers of melanocytes and normal melanin transfer to keratinocytes, suggesting that vascular and optical factors may account for the hypopigmentation.6,7 Alexiades et al6 reported that the hypopigmentation in most striae alba and some scars fails to enhance or fluoresce on Wood (black) light examination, suggesting no detectable decrease in ultraviolet (UV) absorption by melanin in these lesions. In the same study, reflectance spectroscopy data supported the finding that increased lightness in some scars and striae alba are due to increased reflectance and decreased vascularity rather than diminished melanin levels.6
Subtypes
Posttraumatic hypopigmented scars include those due to trauma, burns, surgery, lasers, peels, and other injuries to the skin where melanocytes are irreversibly injured or eliminated.
Postinflammatory hypopigmentation is due to progressive or delayed loss of melanocyte function due to inflammation.
Hypopigmented acne scars are due to reduced or absent pigment within acne scars.
Differential Diagnosis
Vitiligo
Pityriasis alba
Tinea versicolor
Nevus depigmentosum
Nevus anemicus
Lupus vulgaris
Sarcoidosis
Granuloma annulare
Striae alba
Pityriasis rosea
Syphilis
Leprosy
Hypomelanosis of Ito
Hypopigmented mycosis fungoides
Nummular eczema
Post-kala azar leishmaniasis
Lichen planus depigmentosus
PATHOGENESIS
Hypopigmented scars result from cutaneous repair after injury, which can occur from numerous different etiologies, including trauma, burn, post surgery, or post laser treatment. Following damage to the skin, wound healing occurs through well-documented vascular,
inflammatory, proliferative, and tissue remodeling phases.5 Scar tissue forms during the final phase, which can last for several months.1 During this stage, underlying granulation tissue and vascular structures regress and provisional extracellular matrix is remodeled into the final scar tissue. Many of these scars heal with decreased pigmentation.1,6
inflammatory, proliferative, and tissue remodeling phases.5 Scar tissue forms during the final phase, which can last for several months.1 During this stage, underlying granulation tissue and vascular structures regress and provisional extracellular matrix is remodeled into the final scar tissue. Many of these scars heal with decreased pigmentation.1,6
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


