The abdominoplasty procedure poses a number of unique challenges. If the stigmata of the operation is to be avoided, careful planning and surgical execution are required. We describe our experience in full and mini abdominoplasties with a 360-degree approach, involving all muscular groups and body segments as described by high-definition liposculpture. Selective fat grafting is also safely performed in specific areas to improve projection and volume.
Key points
- •
Scarring, pigmentation, and asymmetries remain important patient concerns when excisional abdominal surgery is performed and have become challenging for plastic surgeons.
- •
Full and mini lipoabdominoplasties can be combined with high-definition liposculpture to improve results and also ameliorate most of these stigmata.
- •
Enhanced viability abdominoplasty is a reproducible and safe procedure with very low rate of complications.
- •
Neoumbilicoplasty is a new and very useful concept to avoid hyperpigmentation issues, allowing us to enhance the youthful appearance of the abdominal area.
- •
FIT Mommy procedure is an option for those patients who benefit of some excision in the abdominal wall but do not need an entire resection.
Introduction
Body contouring procedures continue to increase in number worldwide, in part due to lifestyle changes, weight loss surgery, and social media pressures. According to the 2018 American Society of Plastic Surgeons report on procedural statistics, tummy tuck (abdominoplasty) remains the fifth most common cosmetic procedure in the United States, with 130,081 cases.
Years ago, surgeons realized that removing excess skin and fat tissue facilitated hernia repair and improved both the surgical result and patient satisfaction, as described in early lipectomy reports. However, the proper term “abdominal lipectomy” was coined by Kelly in 1899, as the procedure was focused on adipose and skin flap resection. Since these early descriptions, the technique has been subject to multiple modifications and technical improvements enhancing the surgical results. ,
Recent publications have focused on technical variations and means of reducing surgical morbidity. ,
Mini abdominoplasty was introduced by Greminger in 1987 and Wilkinson in 1988. They reported a case series of women with skin laxity and fat excess in the lower mid-region of the abdomen on whom a “limited” abdominoplasty was performed with very reliable results, However, the procedure was not widely adopted and full abdominoplasty remained the overwhelmingly most common option. Today indications for dermolipectomy in postpartum women are defined by the presence of stretch marks and/or laxity of the skin. In patients with mild skin excess, a mini-lipectomy may be considered more appropriate, given the reduced morbidity and clear advantage of umbilicus preservation.
On the other hand, liposuction and newer technologies used alone or in conjunction with abdominoplasty have improved our results. Our experience includes the broad use of third-generation ultrasound (VASER, © 2018 Solta Medical – Bausch Health Companies Inc., Laval, Quebec, Canada) to perform selective fat emulsification, making fat extraction much easier, preserving flap vascularization, and improving long-term aesthetic results. A detailed understanding of the 3-dimensional anatomy combined with new surgical tools allows the surgeon to sculpt the abdomen and reproduce the natural “lights and shadows” of the abdominal area. This forms the basis of high-definition lipoplasty techniques. Although different techniques have been described, the major principles remain the same. The current authors have published their experience with 736 consecutive patients who underwent high-definition lipoabdominoplasty as well as the indications and results of patients who underwent mini-tummy tuck.
In the next sections we will describe our experience with abdominoplasty techniques in addition to 360-degree high-definition liposculpture, which has allowed us to go beyond the traditional procedures.
Anatomy
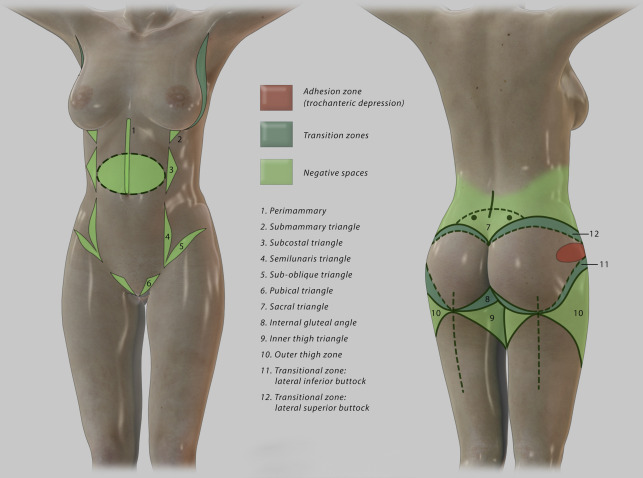
The first important step during preoperative evaluation for body contour surgery is the detailed acknowledgment of the variable aspects of the individual’s anatomy. The ideal abdomen is made of a complex combination of convexities and concavities created by the underlying muscle mass and bone prominences. In the female, the curvaceous, athletic, and slim appearance in the abdominal area is preferred, as this resembles youth and attractiveness. There are 3 areas of concavities recognized:
- 1.
The subcostal area, between the lateral border of the rectus abdominis and the lower costal margin.
- 2.
Between the inguinal ligament and the lower border of the semilunaris line.
- 3.
The midline above the umbilicus.
These concavities as well as other areas in the torso and lower back are special landmarks that we need to have in mind when performing body contour surgery in the abdominal area, as they will ensure the optimum and natural athletic look ( Fig. 1 ).
Women experience different changes in their skin and abdominal wall during pregnancy, due to different mechanical, hormonal, immunologic, metabolic, and vascular changes. This includes pigment alterations, stretch marks, glandular hyper-function, acne and dermatitis, excessive connective tissue relaxation, and diastatic rectus abdominis muscles. Weight gain, skin laxity, and excess of selective fat deposits remain the principal characteristics in women postdelivery. On the other hand, women with excessive weight gain or some grade of obesity also experience some of these concerns. For these patients, to whom liposuction is not suitable because of the postoperative excess skin flap, evident stretch marks, and other issues described previously, excisional abdominal cosmetic surgery is indicated. A 360-degree high-definition liposculpture in addition to mini or full lipoabdominoplasties can be performed according to individual patient characteristics.
Variations among patients are multiple and complex, but the more the deformity the clearer and more aggressive the treatment should be. A detailed preoperative assessment will help to plan the appropriate procedure for each patient. Liposuction may be the best treatment for thin women with minor skin excess and fat deposits, whereas abdominoplasty is best for obese women with severe skin laxity, umbilical ptosis, and abundant abdominal fat deposits.
The difficult group to classify could be the patients who do not fit the criteria for liposuction or abdominoplasty, as they could be just “too little” and “too much,” respectively. Today because of the emphasis on diet, health, and fitness, many women seeking abdominoplasty are less likely to be overweight. Also, more women are having their first pregnancy in their late 30s and early 40s under optimal conditions of medical care. As a consequence, these women require minimally invasive procedures with less obvious scars. So, we have considered these as specific indications for a minimum excisional procedure or FIT Mommy lipoabdominoplasty. On the other hand, there are some women who are marginal candidates for these procedures, but simply will not accept any other surgery (eg, due to large scars or risk concerns), making this technique a relative indication. These patients must be warned about the possibility of having suboptimal results.
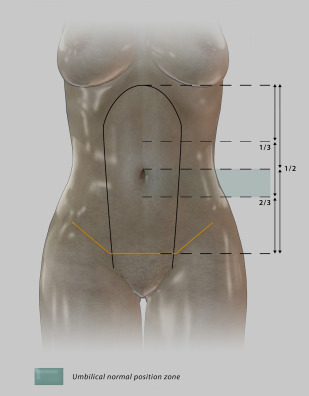
The full abdominoplasty has constantly undergone new improvements reducing the complications associated with the procedure. Stigma about the umbilicus discoloration, and significant and obvious scarring make many think twice about undergoing such a procedure. In particular, the preoperative umbilicus position has been a controversial indication for mini versus full abdominoplasty. Different reports have attempted to standardize umbilical location but many differences exist among populations. We have described an area rather than a unique position as follows : First, we draw a point in the middle of the line between the xiphoid process and the pubic symphysis, then a second point in the intersection of the upper two-thirds and lower one-third of this same line. The zone limited by these 2 points is the one we consider would be optimal for umbilicus placement. In our experience, a straightforward indication for mini-tummy tuck should be the patient with a high umbilicus location and little supraumbilical skin redundancy. In contrast, If the umbilicus was in or below the second drawn point, it would be a better candidate for a full lipoabdominoplasty.
Another important consideration regarding high-definition liposculpture is the dynamic concept of abdominal muscles. All of our muscles move and create different contours in our core structure, allowing our body to be in ceaseless motion. Abdominal muscles are constantly helping in the respiration process as well as the movement of the torso. This dynamic behavior has helped us design an aesthetic approach to avoid the standard “steady” appearance of the belly after liposuction, but rather improve the natural results in high-definition liposculpture. In abdominal excisional surgery, we always perform an active test of abdominal muscle contraction to determine the position of the rectus bellies and underlying anatomy of each patient. If we observe that the new umbilical position may be below the lower one-third of the xiphoid-pubic line, then a full abdominoplasty would be a better choice. Additional explanation is found in the markings section.
Neo Umbilicoplasty
The umbilicus shape and structure has been a matter of debate in multiple societies and cultures. In fact, some religious beliefs surround this remnant of the umbilical cord. The umbilical scar is the foremost stigma that women worry about in lipoabdominoplasty. Its appearance changes through life due to aging and pregnancy: stretching, shape distortion (vertical to horizontal), presence of hernias, and hyperchromia due to hormonal changes in pregnancy may all occur. These factors and its prime visible location give the umbilicus a very important role in abdominal aesthetics that should always be considered. Lipoabdominoplasty undoubtedly affects its position and shape on the abdominal wall. It almost always has a skin tone that is different from the surrounding skin after implantation. Performing a neoumbilicoplasty has consistently changed our patients’ thoughts about full lipoabdominoplasty and has solved all these issues.
Gaudet and Morestin provided the first description of umbilical reconstruction in 1905; however, it was not until 1960 that the research focused on improving abdominal contour. Pitanguy (1975), Baroudi (1975), Regnault (1975), and Psillakis (1984) highlighted the benefits of a lower location of the incision, making the umbilicus smaller and achieving acceptable long-term results. Hence, investigators have focused on describing different techniques for neoumbilicoplasty and we have described our own, which we believe yields optimal results. ,
With regard to umbilical placement, 3 main locations have been described in women: (1) a line drawn from xiphoid to pubis, the umbilicus is then located 60% of the distance from the xiphoid; (2) the umbilicus is located between the anterior-superior iliac spines ; (3) approximately 15 cm measured from the midpoint of the pubic bone upward. These locations have been widely used among plastic and general surgeons in reconstructing and/or relocating the umbilicus. However, a standard measure has not yet been defined. We have considered the location as a dynamic concept that should fit the particularities of the patient’s body distribution and height. So, the specific measures from pubis and iliac spines are not accurate because they do not take into account the height variations and/or the iliac shape. Because the xiphoid-pubis measurement varies according to the individual’s height, youthfulness, and other anatomic considerations, we considered a better choice to describe an “umbilical zone” rather than a single point for each patient ( Fig. 2 ).
Surgical technique
Enhanced Viability Abdominoplasty
According to the book of Genesis from the Bible, Eve was born form Adam’s rib. However, as she did not have an umbilical cord, the umbilicus was nonexistent. This singular biblical deduction inspired us to create a full tummy-tuck procedure enhanced by VASER extraction that increases viability (enhanced viability abdominoplasty [EVA]) to perform high-definition liposculpture in addition to neoumbilicoplasty. It is conceived as a 3-phase procedure that starts with liposculpture, followed by abdominoplasty and ending with umbilicoplasty.
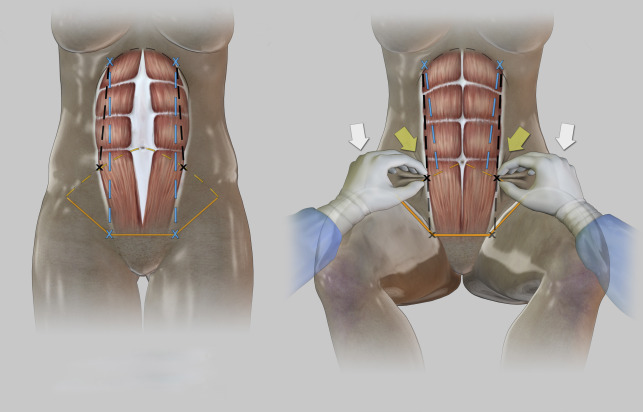
Markings
In standing position, general areas of extra fat deposits are marked on the trunk, abdomen, buttocks, thighs, and arms for deep liposuction. The negative zones for smooth liposuction are marked with another color following our own code. Prohibited zones are also marked in the gluteal and lumbar anatomic regions. The abdominal midline is marked by palpation of the linea alba. The surgeon must predict where the rectus abdominis muscle will be placed after plication. As we discussed previously, we must consider the dynamic concept of the muscular movement on the marking process: this should be done with the patient in a standing position paying attention to the muscle insertions. Do not guide its markings by the superficial landmarks because of the muscular diastases caused by pregnancy. First, in resting muscular position we draw the muscle limits to determine the diastases zone; then, the patient is asked to perform an active muscle contraction to mark the upper and lower insertions of the rectus abdominis muscle. Once these points are referenced, a line is drawn from the upper to the lower direction to predict where the lateral border of the muscle is going to be placed after plication ( Fig. 3 ).