Abdominoplasty is a commonly performed aesthetic procedure but has one of the highest risks for venous thromboembolism (VTE) events in aesthetic surgery. Surgeons can face challenging decisions when performing combination procedures and deciding on appropriate methods of VTE prophylaxis. This article summarizes the current evidence for the incidence of VTE events in abdominoplasty and abdominoplasty combined with other procedures, the current recommendations for risk stratification and management, and options available for mechanical and chemical VTE prophylaxis.
Key points
- •
Abdominoplasty has one of the highest risks for venous thromboembolism events in aesthetic surgery.
- •
Risk for venous thromboembolism is increased when concurrent intra-abdominal, circumferential, or liposuction procedures are performed with abdominoplasty. However, the data on abdominoplasty combined with liposuction are conflicting.
- •
There are no specific recommendations for venous thromboembolism risk reduction in abdominoplasty patients. Mechanical and chemical prophylaxis are at the discretion of the surgeon for each individual patient.
- •
The 2005 Caprini Thrombosis Risk Factor Assessment Form can be useful for risk stratification.
Introduction
Abdominoplasty is one of the most commonly performed aesthetic procedures in plastic surgery, with more than 130,000 procedures being performed in 2018. Despite being one of the most popular plastic surgery procedures, there is a well-known increased risk of venous thromboembolism (VTE) consisting of deep venous thrombosis (DVT), pulmonary embolism (PE), or both, compared with other commonly performed aesthetic surgery procedures.
Although the increased risk of abdominoplasty is well known, management of this risk is a contentious subject. The American Society of Plastic Surgeons (ASPS) has released general VTE prevention guidelines for plastic surgery procedures, but specific recommendations for higher-risk procedures such as abdominoplasty do not exist. This omission leaves management up to individual surgeons, allowing a wide variation in practices for risk reduction.
Incidence
It is generally accepted that abdominoplasty has an increased risk of VTE events compared with other plastic surgery procedures. The exact risk varies by report in the literature because most articles published on the topic are retrospective reviews of large databases or cumulative data. A recent review of the literature with a combined statistical analysis reported the VTE rate for abdominoplasty alone at 0.34%, or 1 in 3000 procedures. Another, more recent, study looked at VTE risk using the American Association for Accreditation of Ambulatory Surgery Facilities’ Internet Based Quality Assurance Program database and reported an incidence of 0.06% for abdominoplasty alone.
Abdominoplasty is frequently performed concurrently with other procedures, and this has been shown to confer additional risk for VTE. The amount of increased risk depends on the type of procedure performed, with additional risk primarily being conferred with intra-abdominal or circumferential procedures. , , Abdominoplasty plus another concurrent plastic surgery procedure (not circumferential or intra-abdominal) does not seem to increase the risk of a VTE event compared with abdominoplasty alone. In addition, this does not seem to depend on the number of concurrent procedures, with an additional 1 to 3 procedures reportedly having the same level of VTE risk. The addition of liposuction to the abdominoplasty procedure may be an exception to this statement. The addition of liposuction specifically may increase the risk of a VTE event, although this topic has been greatly debated and reports are conflicting. , ,
More definitive evidence has shown that patients are subject to substantially higher risks of a VTE event when there is a concurrent intra-abdominal procedure performed with the abdominoplasty. For patients undergoing abdominoplasty with a concurrent intra-abdominal procedure, the risk of a VTE event is estimated at 2.17%. In addition, circumferential abdominoplasty (also known as belt lipectomy) confers a substantially increased risk of VTE events, estimated to be approximately 3.4%. Surgeons and patients need to be knowledgeable of the risks of VTE events, particularly as they relate to concurrent procedures, in order to offer safe surgery and appropriate care postoperatively.
Risk stratification
Potentially Modifiable Risk Factors
Given that abdominoplasty already presents a high risk for VTE events, surgeons must be aware of techniques and scoring models for patient risk stratification in order to inform proper decision making. Abdominoplasty is an elective surgery, providing surgeons with an opportunity to insist on modifiable risk factors being improved before operating. Nonmodifiable risk factors that are present may also need to be addressed preoperatively, which may best be accomplished by including other consultants in the patient work-up before the operation in order to maximize patient safety.
The most commonly referenced and frequently studied score assessment model for VTE risk stratification is the 2005 Caprini Thrombosis Risk Assessment Model ( Fig. 1 ). , The Caprini score is a weighted risk-assessment model that allows validated risk stratification based on numerous factors increasing the risk of a postoperative VTE event.
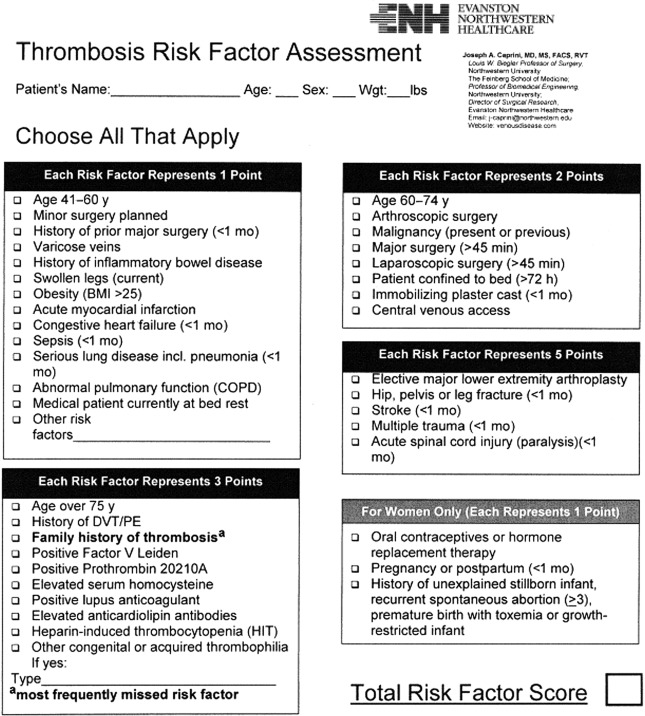
Obtaining a preoperative Caprini score can be valuable for plastic surgeons to properly manage VTE risk postoperatively. Many of the risk factors included within the scoring model are potentially modifiable, and, for patients deemed high risk, insisting on lifestyle modification or other factors can dramatically change the individual’s score. Some of the most notable modifiable components of the Caprini score are increased body mass index (>25), timing of surgery, oral contraceptive use, and recent pregnancy. Previous studies have shown that a reduction of 1 to 2 points in a patient’s Caprini score can cause a 2-fold to 4-fold decrease in the risk of a VTE event. This finding clearly shows that these modifiable factors can have a significant impact. Recent studies by Pannucci and colleagues suggest that effective prophylaxis with enoxaparin may require altering dosage depending on body weight rather than mere standard dosing. This work is preliminary and ongoing. For the nonmodifiable factors, elements such as previous history of DVT/PE or known hypercoagulable disorders may prompt a hematology consultation before surgery to ensure proper patient risk management. This decision should be up to the surgeon’s discretion and each individual patient.
Surgical Factors Increasing Risk
Despite the modifiable risk factors present in many patients, there remain inherent risks with the abdominoplasty procedure. Historically, much of this risk has been attributed to rectus plication creating an increase in intra-abdominal pressure, resulting in venous stasis, a critical component of the Virchow triad. However, more recent studies have evaluated abdominal pressures before and after rectus plication in abdominoplasty and found that the statistically significant increase in abdominal pressure was of questionable clinical significance. ,
Other factors relatively specific to abdominoplasty that have been shown to increase abdominal pressure include skin closure, bed flexion, and the use of an abdominal binder postoperatively. In addition, limited ambulation postoperatively because of pain, waist flexion, or any other factors may increase the risk of VTE events and should be avoided. , , From a global perspective, surgeons should take all of these factors into consideration when performing abdominoplasty and adjust accordingly to reduce patient VTE risk as much as possible.
Prevention
Mechanical Prophylaxis
Little has been specifically studied regarding the use of mechanical prophylaxis in abdominoplasty. However, the ASPS has published a consensus statement recommending intermittent pneumatic compression stockings perioperatively for plastic surgery patients to reduce VTE risk. They also specify that intermittent pneumatic compression stockings are superior to elastic compression stockings in the perioperative setting. They do not provide recommendations for whether or not an extended duration of pneumatic compression stockings or elastic compression stockings is beneficial given a lack of publications on this topic. In a survey of 1106 plastic surgeons, Spring and colleagues reported that most surgeons used intermittent pneumatic compression stockings for patients of all risk profiles (63% for low risk, 82% for moderate risk, and 85% for high risk). Although it may go beyond guideline recommendations, pneumatic compression stockings clearly are a commonly used method for VTE risk reduction in aesthetic surgery regardless of the patient’s risk factors. ,
Chemoprophylaxis
The use of chemoprophylaxis in abdominoplasty has been studied using a variety of different agents, including unfractionated heparin, low-molecular-weight heparin, and oral anticoagulants such as rivaroxaban. , In general, the research is widely varied and with small sample sizes. In addition, most surgeons do not use chemoprophylaxis routinely, although the rate of usage is higher with high-risk patients. , However, previous studies have shown that there is a significant risk reduction with the use of chemoprophylaxis in high-risk plastic surgery patients without an increased risk of bleeding. In addition, recent guidelines published in JAMA recommend low-molecular-weight heparin rather than unfractionated heparin, primarily in critically ill patients, although this may be less specific for plastic surgery outpatient procedures. For abdominoplasty patients, other studies have shown that unfractionated heparin and low-molecular-weight heparin do not increase bleeding risk with perioperative administration, and they reduce the risk of VTE events in high-risk patients. ,
For oral anticoagulants, most of the research has evaluated factor Xa inhibitors. These results are mixed. One small study reported a higher incidence of hematoma when using rivaroxaban, although dosages were not reported by the investigators. Other studies have compared rivaroxaban and apixaban with lower-molecular-weight heparin for body contouring procedures and found similar rates of VTE events, along with similar (rivaroxaban and low-molecular-weight heparin) or lower (apixaban) rates of hematoma. The largest study to date was a multicenter retrospective review of rivaroxaban prophylaxis for abdominoplasty with low rates of VTE events (0.76%) and hematomas (2.3%). Future studies are warranted to more fully evaluate the safety of oral anticoagulants for VTE prophylaxis, although initial results point toward its safety and efficacy.
Formal recommendations
For situations such as abdominoplasty, a common aesthetic procedure with a higher risk of VTE events, surgeons often look to the literature for more formal recommendations to help decide on the most effective prophylaxis protocol, including form of prophylaxis and duration. However, no such guideline exists specifically for abdominoplasty. Surgeons must decide each patient’s individual risk for thromboembolic events and create or adjust their protocols accordingly.
ASPS has released guidelines for VTE prophylaxis in plastic surgery patients, which can be a useful starting point for surgeons deciding on a postoperative protocol. In a 2011 systematic literature review, the ASPS VTE task force focused specifically on the 2005 Caprini Risk Assessment Model rather than the 2010 model to avoid potentially overscoring patients for plastic surgery procedures. After review, the task force found that there was not enough evidence to provide recommendations on specific prophylaxis medications, dosages, or durations, but it did provide a generalized guideline for when to risk stratify patients and when to consider additional prophylaxis ( Table 1 ).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


