After massive weight loss (MWL), patients present with deformities that are more severe and often different than those observed in standard cosmetic abdominoplasty. The first step is careful consideration of the special factors involved in preoperative screening of patients with MWL presenting for body contouring surgery. Once these patient factors are optimized and surgery is considered, careful analysis of anatomic deformities should ensue. Technical variations of standard abdominoplasty are often required. With proper attention to safe screening, analysis of the anatomic deformities, and application of relevant techniques, plastic surgeons can have a positive impact on the lives of these patients.
Key points
- •
A careful evaluation of body mass index and medical comorbidities relevant to patients with massive weight loss (MWL) is essential.
- •
Careful analysis of the anatomic deformities in the abdominal/trunk region guides the choice of procedures to maximize patient satisfaction and avoid complications.
- •
The fleur-de-lis abdominoplasty is a useful operation in patients with MWL and is offered whenever there is significant horizontal skin laxity. If a patient is unsure about this option, it is always possible to perform a procedure with a transverse-only incision and selectively add in the vertical resection in a subsequent stage.
- •
Attention to mons ptosis, as well as excessive pubic fullness, leads to favorable outcomes. Deformity of the pubic region is often neglected in patients with MWL, but correction of the mons should be incorporated with the abdominoplasty technique.
Introduction
For patients with massive weight loss (MWL) presenting for plastic surgery consultation, the evaluation should start with the weight loss history. This conversation begins by gaining an understanding of the mechanism of weight loss, which could involve diet and exercise, sometimes supplemented with pharmacologic agents to induce weight loss, or weight loss surgery. If weight loss surgery has been performed, the type of procedure should be documented, and the plastic surgeon should classify the weight loss procedure as malabsorptive or simply restrictive. The most common malabsorptive procedure is the Roux-en-Y gastric bypass. Restrictive procedures may include vertical gastroplasty or lap band. The patient’s starting weight before embarking on the weight loss journey should be documented, as well the patient’s current weight and body mass index (BMI). The time course of the weight loss should also be noted. If the patient is actively losing weight, generally denoted by weight loss of more than 2.3 kg (5 pounds) a month over the preceding 3 months, surgery should be delayed until the patient has reached a plateau. Any patient who has had weight loss surgery should be queried about symptoms of dumping and nausea/vomiting. These findings are both indications that malnutrition (protein and/or micronutrient deficiency) may be present. Patients generally plateau between 12 and 18 months after weight loss surgery.
The question of screening patients by BMI thresholds always arises. The authors use the following general framework for screening. If a patient has a BMI of 40 or more, the indications for operation should be very compelling, including a disabling giant pannus and/or severe recurrent soft tissue sepsis requiring antibiotic treatment. Chronic open wounds can be another indication for operation. Otherwise, BMI should be optimized with assistance from a nutritional counseling team and the patient’s bariatric surgeon, if applicable. If a patient has a BMI between 35 and 40, similar strict criteria should be applied, and the patient should be encouraged to embark on further weight loss before surgery is strongly considered. Patients presenting with a BMI of 30 to 35 are in a watershed area in which it is important to consider their overall body habitus and fat distribution in the truncal region. The most important factor is intra-abdominal adipose burden, which makes it difficult to obtain a reasonable contour on the abdomen. In contrast, patients with a BMI between 30 and 35 who have more of a gynoid body shape, with a waist-to-hip ratio of less than 1, are more suitable candidates. For patients with a BMI of 30 to 35, with significant intra-abdominal adipose tissue, further weight loss is encouraged. Patients presenting with a BMI of 25 to 30 are generally good candidates for abdominoplasty after weight loss. Some of the overall body weight is an overhanging pannus, which will be removed during surgery. Although patients with a BMI less than 25 are exceptional success stories after bariatric surgery, this end point is uncommon. When BMI is very low (eg, in the range of 20 or 21), suspicion for malnutrition should be high. It is important to keep in mind that many patients presenting for body contouring after weight loss do not have an optimized BMI and it is common to defer surgery while further weight loss is pursued ( Table 1 ).
| BMI (kg/m 2 ) | Surgical Considerations |
|---|---|
| <25 | Generally excellent surgical candidates; consider nutritional deficiencies for extremely low BMI after bariatric surgery |
| 25–30 | Generally excellent surgical candidates |
| 30–35 | Surgery is considered if intra-abdominal fat burden/body habitus lend themselves to satisfactory results |
| 35–40 | Surgery is typically deferred until more weight loss is achieved; limited aesthetic results and higher risk of complications |
| >40 | Surgery should only be considered in cases of severe functional impairment |
Other medical comorbidities associated with obesity should be considered, including diabetes, hypertension, obstructive sleep apnea, severe arthritis, and cardiovascular disease. Presence of these morbidities may prompt further preoperative evaluation by medical consultants, as indicated. It is our practice to require patients cease use of tobacco and nicotine products at least 6 weeks before surgery.
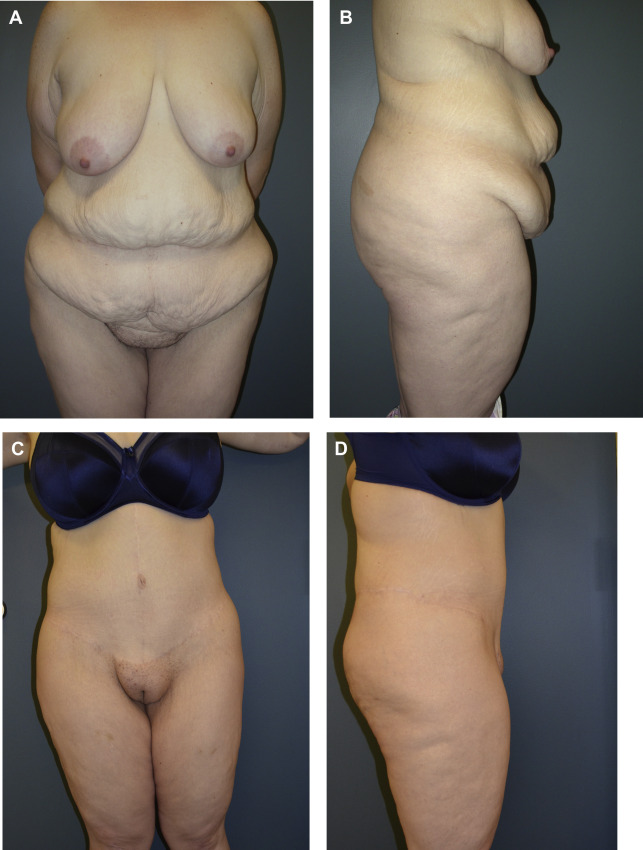
The anatomic evaluation is very important and dictates the choice of procedure and surgical plan. Abdominal wall laxity should be assessed, as well as intra-abdominal adipose tissue mass. Prior scars should be noted. The amount of overhang of the pannus should be evaluated and the tissues under the fold of the pannus inspected for signs of chronic irritation and intertrigo. The mons region should be inspected for evidence of ptosis and excessive fullness. As an examination maneuver, the mons can be elevated manually during the examination with the patient in a standing position, to assess how much surgical elevation will be required. Importantly, the degree of horizontal laxity in the midabdomen and epigastrium should be assessed as patients are considered for a fleur-de-lis abdominoplasty. First described in 1967 by Castanares and Goethel, and later popularized by Dellon, the fleur-de-lis procedure should be considered in 3 circumstances: (1) excessive laxity of the epigastrium that will not be adequately corrected by inferior transposition alone; (2) presence of a prominent subcostal scar, because undermining the scar will threaten the blood supply to the inferior tissues; and (3) an assessment that a highly aggressive plication of the abdominal wall fascia is required. , Patients with extensive protrusion of the abdominal wall fascia may manifest excess skin in the epigastrium after plication, as the skin drapes unevenly over the new smaller contour of the torso. This finding should be discussed with the patient preoperatively so the patient can be involved in the decision-making process to add a vertical scar to the abdomen if necessary. The abdomen should also be assessed for a high double roll. A double roll on the midabdomen is usually easily removed with the abdominoplasty and unfurling of the abdominal flap. However, a high double roll that is just under the inframammary fold is much more difficult to eliminate with a traditional abdominoplasty approach. Additional inspection of the lateral flanks for excess adipose tissue that may be amenable to liposuction should be undertaken. In addition, the extent of circumferential skin laxity should be examined, and, as appropriate, a circumferential lower body lift approach discussed with the patient. During discussion with the patient, it is vital to point out which areas will be corrected and, just as importantly, which areas will not be affected by the planned procedure. Patients may have expectations that the operation will correct rolls or loose skin on the lateral torso. Regions beyond the scope of the abdominoplasty should be pointed out and discussed in the context of potential staged or concurrent additional body contouring procedures. Likewise, in the discussion of the surgical plan, a shared decision-making approach is used and patients are given the option to defer the vertical component of an abdominoplasty if they are unsure about whether to accept the scar. Of course, when it is clearly indicated, the most cost-efficient approach for patients is to undergo a fleur-de-lis in a single-stage abdominoplasty ( Fig. 1 ).