behind the photographer with a uniformly bright background color enhances the viewing of the scalp by creating contrast, thus outlining the peripheral boundaries of the hair. Highdefinition video is often a more convincing media for viewers leery of misleading photographic tricks.
 FIGURE 52.1. A 32-year-old man shown before (A) and 16 months after (B) treatment with 2,450 FU throughout the frontal third of his scalp. A 52-year-old female as seen before (C) and 14 months after treatment with 1,573 FU (D). |
TABLE 52.1 METHODS OF MEASURING HAIR CHARACTERISTICS. INVASIVE, SEMI-INVASIVE, AND NON-INVASIVE TECHNIQUES CAN HELP EVALUATE SUBTLE DIFFERENCES IN HAIR DENSITY, HAIR CALIBER, AND EVEN HAIR GROWTH RATES | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
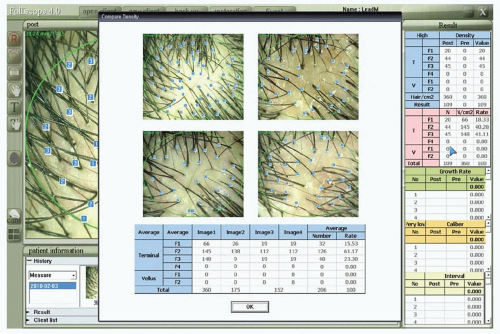 FIGURE 52.2. Folliscope evaluation for density comparison as well as total vellus and terminal hair number. This figure displays four digital images captured at 50-fold magnification and includes the area of 0.34 cm2 (ovals in box) in which quantitative analyses are performed. Calculations of hair density, growth rate, caliber, and spacing are illustrated in numerical format (right-hand panel). |
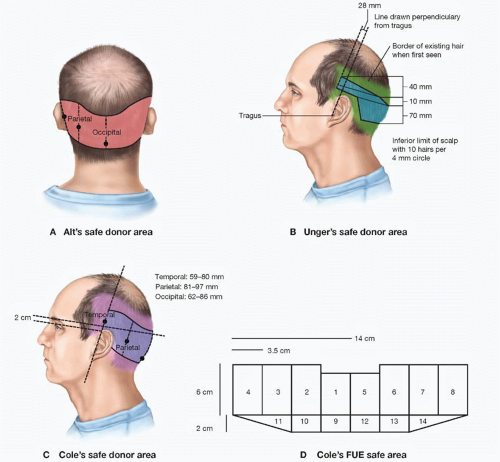 FIGURE 52.3. A. The safe donor area (SDA) according to Alt. B. Unger’s safe donor area for 80% of patients under the age of 80 years, as determined from a study of 328 men aged 65 years or older. C and D. Cole’s FUE safe area. (Images courtesy of J. Devroye, M.D. and J. Cole, M.D. Redrawn from Unger WP, Shapiro R, Unger R, Unger M, eds. Hair Transplantation 5E. London and New York: Informa Healthcare; 2011.) |
have its superior and inferior blood supply somewhat reduced because it is surrounded by virgin scalp tissue rather than bordered by previous scarring. Old scars also bind down the adjacent edge of the neighboring donor strip harvest, which may result in increased closing tension or a reduced available donor strip width. If a new strip is harvested superior (rather than inferior) to a linear scar from a previous surgery, lymphatic drainage will be compromised, leading to more severe and prolonged edema around the new wound. Compounding the probable less-optimal scar that results is the increased likelihood of telogen effluvium in the area between the old and new scar.
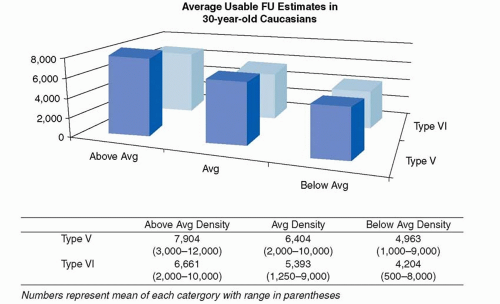 FIGURE 52.4. A total of 34 experts with over 900 years combined experience in hair restoration surgery responded to the question: “Keeping in mind that over the years, the hairs closest to the superior, inferior, and anterior borders of the fringe will be lost, how many FU containing very likely permanent hairs can be harvested from (a) a 30-year-old patient who you believe is destined to develop Norwood type V MPB and has: (1) higher than average hair density; (2) average hair density; (3) less than average hair density; (b) the same question but for a patient you believe is destined to evolve to type VI MPB.” While these data should not be viewed as dogmatic limitations, they may provide helpful guidelines when evaluating the lifetime donor yield of young Caucasian male patients.10 |
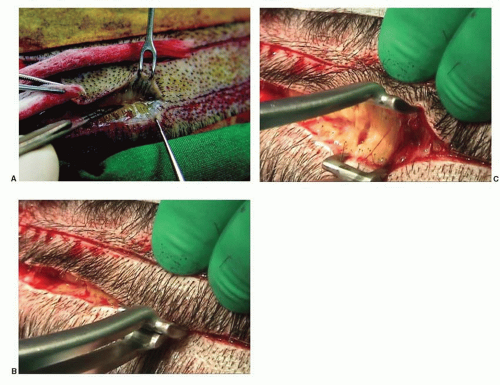 FIGURE 52.5. A. Two skin hooks for one assistant. B. Spreader inserted into scoring incision and (C) the spreader open, showing intact hair follicles at the edge of the wound. (Courtesy of D. Pathomvanich, M.D. and R. Haber, M.D. From Unger WP, Shapiro R, Unger R, Unger M, eds. Hair Transplantation 5E. London and New York; Informa Healthcare; 2011.) |
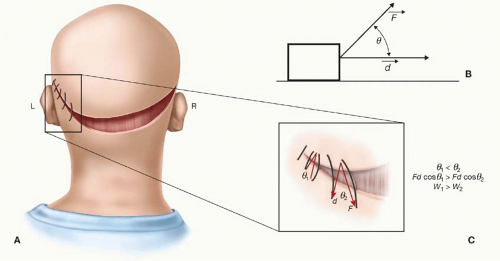 FIGURE 52.6. A. The mastoid region, where scalp tension is often greatest, is the zone in which a wedge suture may be advantageous. A magnified panel illustrating how the placement of wedge sutures is slightly wider along the interior edge of the donor area. B. A block is pulled by a force (F) at an angle (y) to a horizontal vector (d). The work (W) required to pull the block along the horizontal plane (W = Fd cos y) is reduced as y increases. C. The work of a suture to bring two wound edges together is minimized as the placement of sutures along the inferior donor edge widens, increasing the angle (y) along the superior edge. |
the technique employed is, a surgeon’s ability to properly position the punch according to the follicle’s angle of exit from the skin surface typically requires 5× to 6.5× magnification. In addition, as mentioned earlier, use of sterile saline tumescence increases predictability of hair follicle angle deep to the skin surface by making the follicles more erect and separates the follicle bulb from the underlying vascular and nerve plexus.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


