Key Words
hair loss, alopecia, baldness, hirsutism, polycystic ovary syndrome, anagen effluvium, loose anagen hair syndrome, trichotillomania, follicular degeneration syndrome, lupus, lichen planopilaris, pseudopelade, folliculitis decalvans, acne keloid, trichomycosis
Physicians are frequently confronted with hair-related problems. Most complaints are from patients with early-onset pattern baldness. The physician must be able to recognize this normal, inherited hair loss pattern so that detailed and expensive evaluations can be avoided. Other patients have complaints about abnormal hair growth; these diseases must be recognized and not dismissed as balding. The signs of hair loss or excess growth are at times subtle. The signs usually seen with cutaneous disease, such as inflammation, may be absent. A systematic approach to evaluation is essential.
Anatomy
Types of Hair.
There are three types of hair. Thick, pigmented hairs are called terminal hairs. Terminal hairs on the top of the head and in the beard, axillary, and pubic areas are influenced by androgens. Androgens are important in regulating hair growth. At puberty, androgens increase the size of follicles in the beard, chest, and limbs and decrease the size of follicles in the bitemporal region, which reshapes the hairline in men and many women.
Lanugo hairs are the fine hairs found on the fetus; similar fine hairs (peach fuzz) found on the adult are called vellus hairs. Vellus hair is short, fine, and relatively nonpigmented and covers much of the body. Hair on the rest of the body is independent of androgens.
Hair Structure.
The hair shaft is dead protein. It is formed by compact cells that are covered by a delicate cuticle composed of plate-like scales. The living cells in the matrix multiply more rapidly than those in any other normal human tissue. They push up into the follicular canal, undergo dehydration, and form the hair shaft, which consists of a dense, hard mass of keratinized cells. Normal hairs have a pointed tip. The hair in the follicular canal forms a cylinder of uniform diameter. Short hairs with tapered tips either have short growth cycles or have experienced the recent onset of anagen.
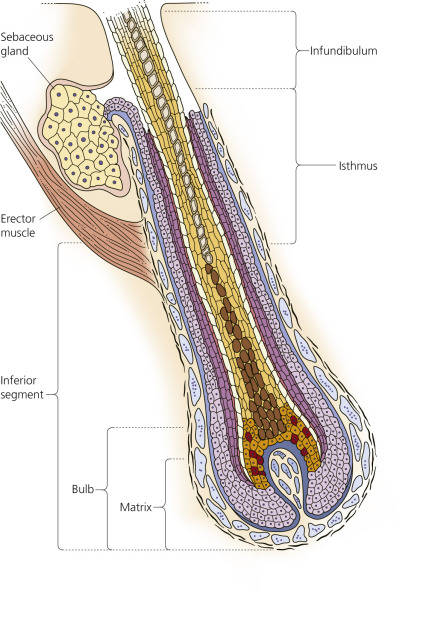
The growing shaft is surrounded by several concentric layers (see Fig. 24.2 ). The outermost glycogen-rich layer is called the outer root sheath. It is static and continuous with the epidermis. The inner root sheath (Henle layer, Huxley layer, and cuticle) is visible as a gelatinous mass when the hair is plucked. It protects and molds the growing hair but disintegrates before reaching the surface at the infundibulum.
The hair shaft that emerges has three layers – an outer cuticle, a cortex, and sometimes an inner medulla – all of which are composed of dead protein. The cuticle protects and holds the cortex cells together. Split ends result if the cuticle is damaged by brushing or chemical cosmetic treatments. The cortex cells in the growing hair shaft rapidly synthesize and accumulate proteins while in the lower regions of the hair follicle. Systemic diseases and drugs may interfere with the metabolism of these cells and reduce the hair shaft diameter. Pigment-containing melanosomes are acquired deep in the bulb matrix and are deposited in the cortical and medullary cells.
Hair Follicle.
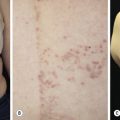
Humans have about 5 million hair follicles at birth. No follicles are formed after birth, but their size changes under the influence of androgens. The hair follicle is formed in the embryo by a club-shaped epidermal down-growth – the primary epithelial germ that is invaginated from below by a flame-shaped, capillary-containing dermal structure called the papilla of the hair follicle. The central cells of the down-growth form the hair matrix, the cells of which form the hair shaft and its surrounding structures. The matrix lies deep within the subcutaneous fat. The mature follicle contains a hair shaft, two surrounding sheaths, and a germinative bulb ( Fig. 24.1 ). The follicle is divided into three sections. The infundibulum extends from the surface to the sebaceous gland duct. The isthmus extends from the duct down to the insertion of the erector muscle. The inferior segment, which exists only during the growing (anagen) phase, extends from the muscle insertion to the base of the matrix. The matrix contains the cells that proliferate to form the hair shaft ( Fig. 24.2 ). The mitotic rate of the hair matrix is greater than that of any other organ. The cells begin to differentiate at the top of the bulb. The inner and outer root sheaths protect and mold the growing hair. The inner root sheath disintegrates at the duct of the sebaceous gland. Hair growth is greatly influenced by any stress or disease process that can alter mitotic activity.
Physiology
Cycling of hair follicles depends on the interaction of the follicular epithelium with the dermal papilla. The dermal papilla induces hair-follicle formation from the overlying epithelium at the onset of each new follicular cycle ( Fig. 24.3 ). The bulge consists of cells in the outer root sheath, which is located near the insertion of the arrector pili muscle. The dermal papilla interacts with germ cells in the hair-follicle bulge to regenerate the lower follicle. Stem cells in the bulge portion of the outer root migrate out of the follicle and regenerate the epidermis after injury.
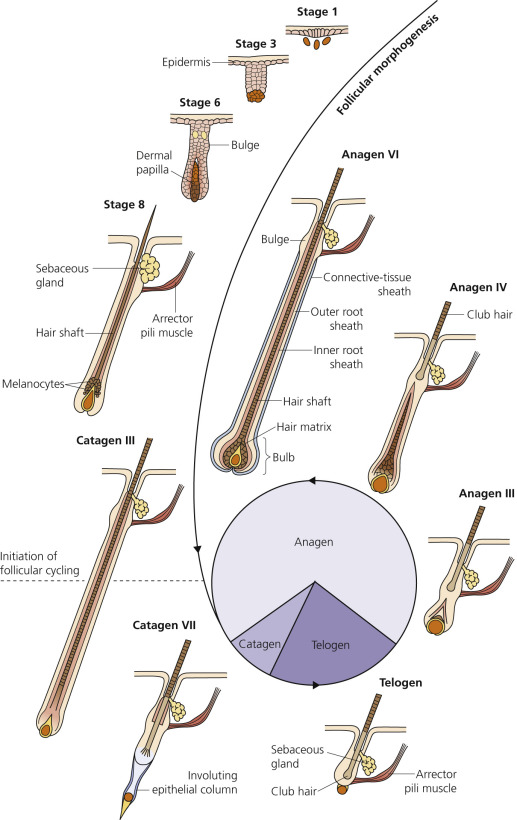
Rapidly proliferating matrix cells in the hair bulb produce the hair shaft. The matrix cells differentiate, move upward, and are compressed and funneled into their final shape by the rigid inner root sheath. The shape (curvature) of the inner root sheath determines the shape of the hair. The bulk of the hair shaft is called the cortex. Pigment in the hair shaft is produced by melanocytes interspersed among the matrix cells. The volume of the dermal papilla determines the diameter of the hair shaft.
Hair Growth Cycle
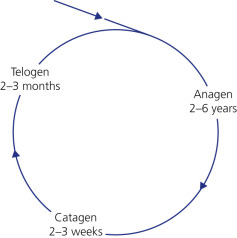
The average scalp has more than 100,000 hairs. The growth phase of scalp hair is approximately 1000 days (range, 2 to 6 years). Hair in other areas, such as the eyebrows and eyelashes, has a shorter growth phase (1 to 6 months). Scalp hair grows 0.3 to 0.4 mm/day, or approximately 6 inches a year.
Humans have a mosaic growth pattern; hair growth and loss are not cyclic or seasonal, as in some mammals, but occur at random, so that hair loss is continuous (see Fig. 24.3 ). Each hair follicle perpetually goes through three stages in the hair growth cycle: catagen (transitional phase), telogen (resting phase), and anagen (growing phase) ( Fig. 24.4 ). Approximately 90% to 95% of hairs are in the anagen phase, and 5% to 10% are in the telogen phase. Up to 100 telogen hairs are lost each day from the head, and about the same number of follicles enter anagen. The duration of anagen determines the length of hair, and the volume of the hair bulb determines the diameter.
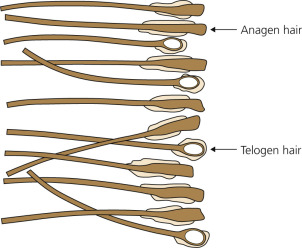
Anagen and telogen hairs from hair-plucked preparation are shown in Fig. 24.5 .
Anagen (Growth).
The anagen or growth phase begins with resumption of mitotic activity in the hair bulb and dermal papilla. Interactions between the dermal papilla and the overlying follicular epithelium are required for the onset of anagen. The follicle grows down and meets the dermal papilla, recapitulating the embryonic events of development of the hair follicle. A new hair shaft forms and forces the tightly held club hair out. During anagen, hair grows at an average rate of 0.35 mm/day, or 1 cm in 28 days; this rate diminishes with age.
Hair follicles in different areas of the body produce hairs of different lengths. The length is proportional to the duration of the anagen cycle. Scalp hair remains in an active growing phase for an average of 2 to 6 years. The active growing phase is much shorter and the resting stage is longer for hair on the arms, legs, eyelashes, and eyebrows (30 to 45 days), which explains why these hairs remain short. Approximately 90% to 95% of scalp hairs are in an active growing phase at any one time. Continuous anagen occurs in some dogs (e.g., poodles) and in merino sheep; these animals do not lose or shed hair.
Catagen (Involution).
Catagen is a process of involution that occurs with cell death in follicular keratinocytes. It is the phase of acute follicular regression that signals the end of anagen. Less than 1% of scalp hairs are in this 2 to 3 week transitional phase at any one time. Cell division in the hair matrix stops, and the resting, or catagen, stage begins. The outer root sheath degenerates and retracts around the widened lower portion of the hair shaft to become a club hair. The lower follicle shrinks away from the connective tissue papilla and ascends to the level of the insertion of the erector muscle. The dermal papilla condenses and moves upward, coming to rest underneath the hair-follicle bulge. The completion of catagen is marked by formation of the normal club hair.
Telogen (Rest).
All activity ceases and the structure rests during the telogen phase. The telogen phase in the scalp lasts for 2 to 3 months before the scalp follicles reenter the anagen stage and the cycle is repeated. The percentage of follicles in the telogen stage varies according to the body region. Approximately 5% to 10% of scalp hairs are in the telogen phase at any one time, and these follicles are randomly distributed. The telogen phase is much longer in eyebrow, eyelash, trunk, arm, and leg hair. Approximately 40% to 50% of follicles on the trunk are in the telogen phase. The inactive dead hair, or club hair, has a solid, hard, dry, white node at its proximal end; the white color is due to a lack of pigment. The club hair is firmly held in place and then ejected. A new anagen hair grows and replaces the shed telogen hair. Approximately 25 to 100 telogen hairs are shed each day; possibly twice this number are lost on the days the hair is shampooed. Seasonal shedding occurs in other animals but is random in humans.
Evaluation of Hair Loss
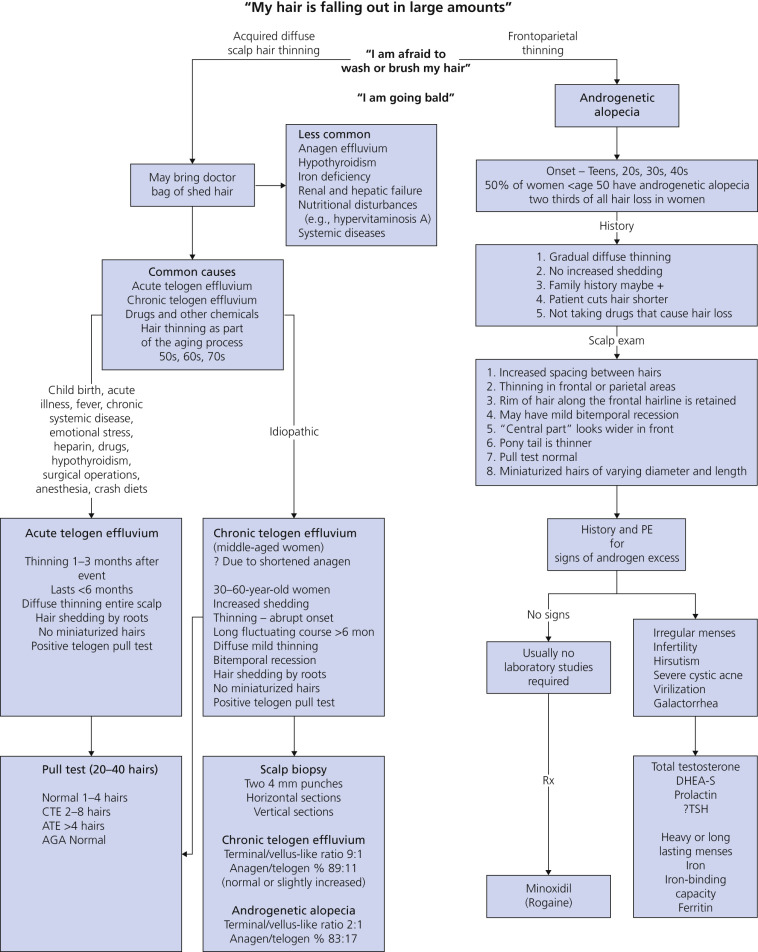
The causes of hair loss (alopecia) are numerous. Most hair problems seen by the practitioner are due to changes in hair-follicle cycling. Many inflammatory conditions permanently damage the hair follicle, resulting in scarring alopecia. A classification is used here that is based primarily on distribution and scarring (i.e., localized [patchy] versus generalized and scarring versus nonscarring). A systematic approach for evaluation of hair loss is outlined in Box 24.1 and Table 24.1 . The evaluation of the woman who observes that “My hair is falling out in large amounts” is presented in Fig. 24.6 . Alopecia occurs when hair shafts are fragile and break due to many inherited and acquired disorders.
|
|
| (This scheme will diagnose 97% of cases of alopecia.) | |||||
| Disease | Scalp | Pattern | Pull Test | Laboratory | Treatment |
| DIFFUSE LOSS (NONSCARRING) | |||||
| Telogen effluvium | Normal | Diffuse | Increased telogen | Disease specific | Disease specific |
| Diffuse alopecia areata | Normal | Irregularly diffuse | Increased telogen | – | Topical immunotherapy |
| Androgenetic alopecia (men) | Normal | Hamilton ( Fig. 24.8 ) | Negative | – | Minoxidil Finasteride 1 mg Surgery |
| Androgenetic alopecia (women) | Normal | Ludwig ( Fig. 24.9 ) | Negative | Testosterone DHEA-S | Minoxidil Oral contraceptives Spironolactone |
| Systemic disease (thyroid, iron deficiency, systemic lupus erythematosus, dermatomyositis) | Normal in most | Diffuse | Normal or increased telogen | Thyroid function Iron/IBC ANA | Disease specific |
| PATCHY LOSS (SCARRING) | |||||
| Discoid lupus erythematosus | Atrophy, dyspigmentation, follicular plugging | Patchy | Negative | Biopsy | Intralesional steroids Hydroxychloroquine |
| Lichen planopilaris | Hairs trapped in “islands” | Patchy | Negative | Biopsy Immunofluorescence | Intralesional steroids Hydroxychloroquine |
| Frontal fibrosing alopecia | Advancing edge perifollicular papules | Develops on frontal hairline, extends backward | Negative | Biopsy Immunofluorescence | Same as lichen planopilaris |
| Pseudopelade | Scarring, noninflammatory | Moth-eaten pattern | Negative | Biopsy Immunofluorescence | Topical steroids Hydroxychloroquine |
| Central centrifugal cicatricial alopecia | Scarring in localized pattern | Patchy over crown | Negative | Biopsy | Avoid hair traction |
| Folliculitis decalvans | Pustules at periphery Bogginess | Patchy | Negative | Biopsy Immunofluorescence | Antibiotics |
| Dissecting cellulitis/ folliculitis | Abscess formation | Diffuse | Negative | Biopsy, culture | Antibiotics |
| Acne keloid | Pustules and dense follicular papules | Occipital scalp | Negative | Biopsy, culture | Antibiotics |
| Tufted folliculitis | Many hairs arise from a giant follicle | Occipital scalp | Negative | Biopsy | Antibiotics |
| PATCHY LOSS (NONSCARRING) | |||||
| Alopecia localized | Normal | Patchy + exclamation mark hairs | May be + at margins | KOH (children) | Intralesional steroids Minoxidil Anthralin |
| Tinea capitis | Scale or papules or pustules | Patchy | Hair breakage | KOH Fungal culture | Oral antifungal antibiotics |
| Traction alopecia | ± Scarring | Patchy, marginal | Hair breakage | – | Avoid |
| Trichotillomania | ± Scarring, normal | Patchy with stubble | Usually negative | – | Fluoxetine, others Psychotherapy |
| Syphilis | Normal | Moth-eaten | Increased telogen | RPR | Penicillin |
| Hair breakage | Normal | Patchy or marginal | Broken hairs | – | – |
Diagnosis of Hair Disease
History.
Inquire about medication use, calorie restriction, vitamin A supplementation, and thyroid symptoms. Determine the precise onset and the duration of hair loss. Abrupt-onset telogen effluvium is most often related to a specific traumatic event. Gradual or imperceptible onsets are more complicated and involve possible shortened anagen, as well as a differential diagnosis that includes alopecia areata (AA), androgenetic alopecia, and diffuse primary scarring alopecias.
Physical Examination.
Examine the scalp surface and hair shafts. Microscopically examine hair ends and hair shaft diameters. Hair density may be reduced by 50% before hair thinning becomes clinically apparent; therefore observation is an inaccurate method of evaluating hair density and loss. Examine all nonglabrous skin, teeth, and nails. Findings in these areas may lead to diagnostic clues.
Hair Pull Test.
For the hair pull test, obtain a sample 3 cm above the auricle. Tightly grasp 20 to 40 hairs firmly between the thumb and forefinger. Exert a slow, constant traction to slightly tent the scalp, and slide the fingers up the hair shafts. There should be fewer than six club hairs extracted. Repeat the count on the opposite side of the head and in two other areas. Examine the hair bulbs.
Daily Counts.
The patient collects hair lost in the first morning combing and includes those lost during washing for 14 days, saving them in clear plastic bags. The patient counts the hairs and records the number on the bags. Examine the hairs under the microscope to determine if the bulbs are anagen or telogen. Daily hair shed counts are not necessary if the pull test is positive. It is normal to lose up to 100 hairs daily and 200 to 250 hairs on the day of shampooing. If the hair is shampooed daily, the counts should be less than 100.
Part Width.
Make a coronal part with a comb over the vertex. Note the part width. Make a series of parallel parts over the vertex and visually compare the part diameter. Do the same over the occipital and temporal scalp. Visually compare the part diameters in the different anatomic scalp areas. Hair density is greatest in childhood and decreases progressively with age. The hair is less dense in the vertex in both genders, and thinning increases with age.
Hair Shaft Examination (Clip Tests).
Grasp 25 to 30 hairs between the thumb and forefinger just at the scalp surface. Cut the hair between the fingers and the scalp. Hair just above the fingers is cut and discarded. Float the hairs onto a wet microscope slide and cover with another slide. Evaluate hair shaft diameter and structure. There are many rare diseases that produce shaft structural abnormalities, such as pili torti in which the hair is twisted on its axis.
Hair Growth Window.
Select an area where the hair fails to grow and an area that can be covered by the remaining hair. Cut the hair short; then shave a 2.0 cm 2 area. Cover the area with an occlusive dressing and remove it in 1 week if trichotillomania (TTM) is suspected. Normal growth is 2.5 mm in 1 week and 1 cm in 1 month. This test proves to the patient that the hair is growing.
Hair Pluck – Trichogram.
This is a painful technique but is still used by some clinicians. Abruptly extract hairs from the scalp with a rubber-tipped needle holder. Cut the excess hair 1 cm from the roots, float the hairs onto a wet microscope slide or Petri dish, and examine with a hand lens (see Fig. 24.5 ).
Telogen hairs have small, unpigmented, ovoid bulbs and do not contain an internal root sheath. Anagen hairs have larger, elongated, pigmented (if hair is pigmented) bulbs shaped like the end of a broom, surrounded by a gelatinous internal root sheath.
There are diseases in which hair fragments with absent bulbs are obtained during a hair pull. Processes that interfere with cell division cause the shaft to be poorly formed and therefore apt to break under tension. Alopecia areata, antimetabolite therapy, and small doses of ionizing radiation interrupt the mitotic activity in the cells that normally contribute to the growing hair.
Trichoscopy.
Magnification of the scalp with a dermatoscope allows for in situ observation of the follicular ostia, hair shafts, blood vessels, and for the presence or absence of subtle scale and erythema.
Generalized Hair Loss
Diffuse hair loss ( Box 24.2 and Table 24.2 ) usually occurs without inflammation or scarring. The loss affects hairs throughout the scalp in a more or less uniform pattern. The hair pull test is important for differential diagnosis.
Generalized *
* Diffuse, uniform loss, but many hairs left randomly distributed in area of loss.
- •
Acute blood loss
- •
Childbirth
- •
Crash diets (inadequate protein)
- •
Drugs
- •
Coumarin
- •
Retinoids (isotretinoin, acitretin)
- •
Anticoagulants (particularly heparin)
- •
Amantadine
- •
Lithium
- •
Penicillamine
- •
Βeta-blockers (e.g., propranolol)
- •
Amiodarone
- •
Vitamin A excess
- •
Captopril
- •
Antiinflammatories (e.g., colchicine, cimetidine)
- •
Antineoplastic agents
- •
Antihyperlipidemics
- •
Antithyroid (e.g., propylthiouracil, methimazole)
- •
Anticonvulsants (e.g., valproic acid, carbamazepine, phenytoin)
- •
- •
High fever
- •
Hypothyroidism and hyperthyroidisms
- •
Physical stress (e.g., surgery)
- •
Physiologic stress (e.g., neonate)
- •
Psychologic stress
- •
Severe illness (e.g., systemic lupus erythematosus)
- •
Cancer chemotherapeutic agents
- •
Poisoning
- •
Thallium (rat poison)
- •
Arsenic
- •
- •
Radiation therapy
- •
Secondary syphilis: “moth eaten” alopecia
Localized †
† Most or all hair missing from involved area.
- •
Androgenetic alopecia
- •
Male pattern
- •
Female pattern
- •
- •
Hirsutism
- •
Alopecia areata
- •
Trichotillomania
- •
Traction alopecia
- •
Scarring alopecia
- •
Developmental defects: aplasia cutis
- •
- •
Physical injury: burns, pressure
- •
Infection
- •
Fungal: kerion
- •
Bacterial: folliculitis, furuncle
- •
Viral: herpes zoster
- •
- •
Neoplasms
- •
Metastatic carcinoma
- •
Sclerosing basal cell carcinoma
- •
- •
Lupus erythematosus
- •
Lichen planus
- •
Cicatricial pemphigoid
- •
Scleroderma
| Clinical Presentation | Telogen | Anagen |
|---|---|---|
| Onset of shedding after insult | 2–4 months | 1–4 weeks |
| Percent of hair loss | 20–50 | 80–90 |
| Type of hair loss | Normal club (white bulb) | Anagen hair (pigmented bulb) |
| Hair shaft | Normal | Narrowed or fractured |
Telogen Effluvium.
A number of events have been documented that prematurely terminate anagen and cause an abnormally high number of normal hairs to enter the resting, or telogen, phase (see Box 24.2 ). The follicle is not diseased but has had its biologic clock reset and undergoes a normal involutional process. Usually no more than 50% of the patient’s hair is affected. Scarring and inflammation are absent. Resting hairs on the scalp are retained for approximately 100 days before they are lost; therefore telogen hair loss should occur approximately 3 months after the event that terminated normal hair growth.
Kligman explained this process and identified the various precipitating events (see Box 24.2 ). The most common causes are briefly discussed here. High fever from any cause may result in a sudden, diffuse loss of club hairs 2 to 3 months later. Hair loss begins abruptly and lasts for approximately 4 weeks. Hair pluck tests show telogen counts that vary from 30% to 60%. Full recovery can be expected.
Severe emotional and physical traumas have been documented to cause diffuse hair loss. Hair loss has been reported to occur 2 weeks after severe psychologic or physical trauma, but because that is too short a time for the induction of the telogen phase, the loss must have occurred by another mechanism. Some individuals may experience increased shedding caused by idiopathic shortening of anagen (a short anagen syndrome). They have increased shedding and decreased hair length. For every 50% reduction in the duration of anagen, there is a corresponding doubling of follicles in telogen.
Chronic Telogen Effluvium.
Chronic telogen effluvium (CTE) refers to a diffuse hair loss all over the scalp and persists for more than 8 months. Patients present with hair loss with increased shedding and thinning of abrupt onset and fluctuating course. There is diffuse thinning over the entire scalp, frequently accompanied by bitemporal recession. CTE usually affects 30- to 60-year-old women. It may be distinguished from classic acute telogen effluvium by its long fluctuating course and from androgenetic alopecia by its clinical and histologic findings. CTE lasts from 6 months to 7 years.
Many physicians test patients with hair loss for iron deficiency and thyroid abnormalities. Iron deficiency is commonly found in CTE but treatment for it seldom reverses the hair loss. Perform a ferritin and a transferrin saturation evaluation if iron deficiency is suspected. The long, fluctuating course is different than that seen in acute telogen effluvium. The presence of 20% to 30% telogen hairs and 15% to 35% dystrophic hairs on the trichogram (plucked hair) confirms the diagnosis. A biopsy can support the diagnosis but is usually not necessary. CTE is distinguished from androgenetic alopecia by distribution, trichogram and a biopsy.
Men are treated with 5% minoxidil solution. Premenopausal women are prescribed 5% minoxidil solution plus cyproterone acetate (CPA) (not available in the United States) 50 mg, from day 5 to day 15 of their menstrual cycle, always taken together with ethinyl estradiol 0.035 mg/day. Postmenopausal women are treated with 5% minoxidil solution plus CPA 50 mg/day. Alternatives to CPA 50 mg/day could be spironolactone 50 to 100 mg/day.
Biopsies confirm the diagnosis but are usually not necessary. Two 4-mm punch biopsy specimens are taken from the mid or posterior parietal scalp. Specimens are sectioned horizontally and vertically. The findings are shown in Fig. 24.6 .
Postpartum Hair Loss.
The percentage of follicles in telogen progressively decreases during pregnancy, particularly during the last trimester. Diffuse but primarily frontotemporal hair loss occurs in a significant number of women 1 to 4 months after childbirth. The loss can be quite significant, but recovery occurs in less than 1 year. Hair growth usually returns to the pre-pregnancy state. Postpartum hair loss is thought to be due to a prolongation of the anagen phase due to stimulating factors; when the factors are removed, more hairs enter the telogen phase and hair falls out at once (delayed anagen release).
Drugs.
Cytotoxic drugs that directly affect hair matrix cell proliferation cause profound hair loss, inducing an anagen effluvium. A large number of drugs probably cause telogen effluvia. These are listed in Box 24.3 .
Acitretin
Aminosalicylic acid
Amphetamines
Bromocriptine
Captopril
Carbamazepine
Cimetidine
Coumadin
Danazol
Enalapril
Levodopa
Lithium
Metoprolol
Propranolol
Pyridostigmine
Trimethadione
Anagen Effluvium.
Anagen effluvium (see Box 24.2 and Table 24.2 ) is the abrupt loss of hair from follicles that are in their growing phase. An abrupt insult to the metabolic and follicular reproductive apparatus must be delivered to create such an event. Cancer chemotherapeutic agents and radiation therapy are capable of such an insult. The rapidly dividing cells of the matrix and cortex are affected. The insult causes a change in the rate of hair growth but does not convert the follicle to a different growth phase, as occurs in telogen effluvium. High concentrations of antimetabolites or radiation bring the entire metabolic process to an abrupt halt, and the entire hair and hair root are shed intact. The only hairs left are those in the telogen phase ( Fig. 24.7 ). These are dead, wedged into the hair canal, and unaffected by any acute event. The stem cells of the hair follicles are spared because of their slow cycling, and they generate a new hair bulb. Insults of less intensity slow the mitotic rate of the bulb and cortex cells, causing bulb deformity and narrowing of the lower hair shaft. Narrow, weakened hair shafts are easily broken and shed without bulbs. Since 90% of scalp hairs are in the anagen phase, a large number of hairs can be affected. Patients with 10% to 20% of their hair remaining after an insult almost certainly have had an anagen effluvium.

Scalp hypothermia decreases the amount of chemotherapy delivered to the scalp and minimizes anagen effluvium, especially in breast cancer patients. DigniCap ( www.dignicap.com , Food and Drug Administration approved in the United States) and Paxman Scalp Cooling System are two available devices.
Minoxidil 2% topical has no benefit in the prevention of chemotherapy-induced alopecia.
Loose Anagen Hair Syndrome.
The loose anagen hair syndrome (LAS) is a rare sporadic or familial hair disorder that affects children but may be seen in adults. The female-to-male ratio is 6 : 1. LAS is due to a defective anchorage of the hair shaft to the follicle that results in easily and painlessly pluckable hair.
LAS may result from premature keratinization of the inner root sheath that produces an impaired adhesion between the cuticle of the inner root sheath and the cuticle of the hair shaft.
The typical patient with LAS is a young girl with short blond hair that does not grow long, but LAS can affect children with dark hair. The signs are reduced hair length, increased hair shedding, and altered hair texture. These patients may have sparse hair that does not grow long and have patches of dull, unruly hair. Others just have increased hair shedding. The child needs few haircuts, and the hair is difficult to manage. Examination shows diffuse thinning and irregular bald patches attributable to traumatic painless extraction of hair tufts. Hair is dull, unruly, or matted. Up to 300 hairs are shed daily. Most cases are isolated, but it can occur in hereditary or developmental disorders including coloboma, Noonan syndrome, and hypohidrotic ectodermal dysplasia.
Microscopic examination shows anagen hair without sheath. The bulb is often misshapen, and its proximal portion often shows a visible ruffled cuticle. The pull test in children with LAS shows more than 3 and often more than 10 loose anagen hairs. The pull test in normal children shows one or two loose anagen hairs. The trichogram in LAS shows at least 70% loose anagen hairs and no telogen hairs. Most patients improve with age.
Short anagen syndrome due to a short duration of the anagen phase (4 to 10 months) results in short hair and has a similar presentation to loose anagen syndrome. The short duration of anagen causes synchronization of the hair cycle with periods of diffuse hair shedding. Parents often note that the child’s hair remains short despite not having a haircut. After a hair pull test, hairs have pointed tips and do not have hockey stick–shaped hair bulbs with proximal ruffling of the cuticle as is seen in loose anagen syndrome. Table 24.3 compares loose anagen and short anagen syndromes. Patients may see improvement in hair density, but most patients do not grow long hair.
| Short Anagen Syndrome | Loose Anagen Syndrome | |
|---|---|---|
| Chief complaints | Hair that does not grow long Excessive shedding | Hair that does not grow long Patchy, diffuse hair loss Unruly hair |
| Pull test | Positive | Usually negative |
| Physical examination | Very short hair (<6 cm) | Short hair (<shoulder length) |
| Trichoscopy | No specific features | Black rectangular structures |
| Microscopic examination | Short tapered telogen hairs | Anagen hairs devoid of sheaths, ruffled cuticles |
| Treatment | Reassurance, minoxidil | Reassurance, minoxidil, gentle styling |
| Prognosis | Improves with age Unlikely to grow long hair | Improves with age |
Localized Hair Loss
Androgenetic Alopecia in Men (Male Pattern Baldness)
Baldness in men is not a disease, but rather a physiologic reaction induced by androgens in genetically predisposed men. The pattern of inheritance is probably polygenic. Thinning of the hair begins between the ages of 12 and 40 years, and about half the population expresses this trait before the age of 50.
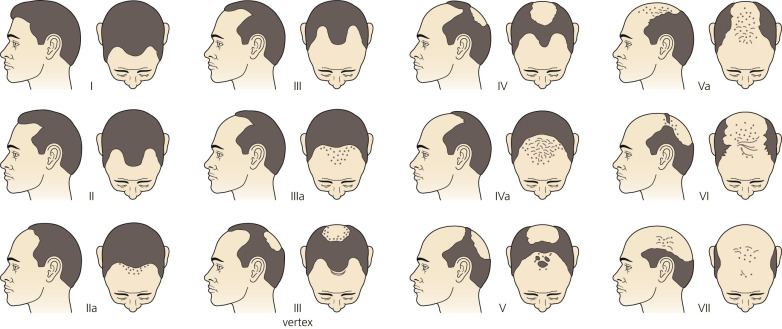
Hamilton Patterns.
The progression and various patterns of hair loss are classified by the Hamilton male baldness classification system ( Fig. 24.8 ). Triangular frontotemporal recession occurs normally in most young men (type I) and women after puberty. The first signs of balding are increased frontotemporal recession accompanied by midfrontal recession (type II). Hair loss in a round area on the vertex follows, and the density of hair decreases, sometimes rapidly, over the top of the scalp (types III through VII). Approximately 10% of men have hair loss that looks like female pattern hair loss with sparing of the frontal hairline and hair loss on the central scalp.
Pathophysiology.
Androgenetic alopecia is due to the progressive shortening of successive anagen cycles. There are two populations of scalp follicles: androgen-sensitive follicles on the top and androgen-independent follicles on the sides and back of the scalp. In genetically predisposed individuals, and under the influence of androgens, predisposed follicles are gradually miniaturized, and large, pigmented hairs (terminal hairs) are replaced by thin, depigmented hairs (vellus hairs).
Inflammation surrounds the bulge area of the outer root sheath. The inflammation may damage the follicle stem cells, which results in a decrease in hair-follicle density. Hair follicles are still present, but removing androgens or treatment with minoxidil or finasteride does not result in the conversion of miniaturized follicles back to terminal ones.
Skin Androgen Metabolism.
Testosterone (T) is converted to the more potent dihydrotestosterone (DHT) by 5α-reductase. Skin cells contain 5α-reductase (types I and II). The type I enzyme is found in sebaceous glands, and the type II enzyme is found in hair follicles and the prostate gland. Testosterone and DHT act on androgen receptors in the dermal papilla. They increase the size of hair follicles in androgen-dependent areas such as the beard area during adolescence, but later in life DHT binds to the follicle androgen receptor and activates transformation of large, terminal follicles to miniaturized follicles. The duration of anagen shortens with successive hair cycles, and the follicles become smaller, producing shorter, finer hairs. Androgenetic alopecia does not develop in men with a congenital absence of 5α-reductase type II. Finasteride, which inhibits 5α-reductase type II, slows or reverses the progression of androgenetic alopecia.
Treatment.
The desire for treatment varies. Some men accept the inevitable; others find baldness intolerable. Topical treatment (minoxidil), oral treatment (finasteride), and several surgical procedures are available. The drugs can enlarge existing hairs and retard thinning in the vertex and the frontal regions. They have no benefit for men who are bald or those with bitemporal recession without hair. Benefits are seen in 6 to 12 months. Treatment must be continued indefinitely. If treatment is stopped, benefits are lost within 6 to 12 months, and hair density will be the same as before treatment. Patients who begin balding at an early age are most distressed and are tempted to consult nonphysician “experts” at hair clinics. These clinics offer a variety of topical preparations, none of which has any value. Selected patients may be referred for hair transplants, plastic surgical rotation flaps, or wigs.
Minoxidil.
Minoxidil was developed to treat hypertension. It increases the duration of anagen, causes follicles at rest to grow, and enlarges miniaturized follicles. These effects occur in only a minority of patients. Minoxidil 2% (Rogaine) and 5% (Extra Strength Rogaine) are available over the counter in a solution or foam preparation. Generic brands of the 2% solution are available. One milliliter of solution is applied twice daily and spread lightly with a finger. An applicator conveniently and effectively applies the medication. Minoxidil increases nonvellus hairs. Spontaneous reversal to the pretreatment state occurs in 1 to 3 months after stopping treatment. Ideal candidates are men younger than 30 years of age who have been losing hair for less than 5 years. The solutions produce a modest increase in hair on scalps of young men and women with mild to moderate hair loss, with continuous twice daily application for years to maintain the effect. In men with androgenetic alopecia, 5% topical minoxidil was clearly superior to 2% topical minoxidil in increasing hair regrowth, and the magnitude of its effect was marked (45% more hair regrowth than 2% topical minoxidil at week 48).
One 48-week study in women showed that 5% topical minoxidil was superior to 2% topical minoxidil in the patient assessment of treatment benefit. Application of 2% topical minoxidil in this study showed that differences in patient assessment of hair growth at week 48 were not significantly different from those for the placebo. A 48-week study in men found a mean increase in hairs per square centimeter of 12.7 with 2% minoxidil, and 18.5 with 5% minoxidil. One study found that topical use of 2% minoxidil caused small but statistically significant increases in left ventricular end-diastolic volume, cardiac output, and left ventricular mass. Dizziness and tachycardia have been reported with 2% solution. Local irritation, itching, dryness, and erythema may occur and are likely attributable to the vehicle of alcohol and propylene glycol. The medication is applied to a dry scalp twice a day. The hair should not be wet for at least 1 hour afterward. About one third of these patients grow hair that is long enough to be cut or combed. Hair growth is evident in 8 to 12 months. Minoxidil may stop or retard the progression of male pattern baldness. In one large study of long-term use, almost all patients gradually avoided continuing the treatment. The causes of discontinuation in the majority of patients were the insignificant cosmetic effect and an aversion to this topical treatment method.
Finasteride.
Finasteride (Propecia 1 mg) taken daily is an effective oral therapy for androgenetic alopecia in men. Some physicians prescribe finasteride (Proscar 5 mg) and instruct patients to split the 5-mg tablet with a pill splitter into four equal parts. The cost savings is considerable. Based on global photographic assessment, finasteride (1 mg) is able to increase hair growth in all areas of the scalp affected by male pattern hair loss.
Androgenetic alopecia (male pattern hair loss) is caused by androgen-dependent miniaturization of scalp hair follicles, with scalp DHT level implicated as a contributing cause. Finasteride blocks 5α-reductase type II, which inhibits the conversion of T to DHT and decreases serum and cutaneous DHT concentrations. This slows further hair loss, inhibits androgen-dependent miniaturization of hair follicles, and improves hair growth and hair weight in men with androgenetic alopecia.
In men with male pattern hair loss, finasteride 1 mg/day slowed the progression of hair loss and increased hair growth in clinical trials over 2 years. Therapy leads to slowing of further hair loss.
Efficacy is evident within 3 months of therapy. The drug produces progressive increases in hair counts at 6 and 12 months. Finasteride treatment for 4 years leads to sustained improvement in hair weight. Hair weight increased to a larger extent than hair count. Finasteride is effective in men with vertex male pattern hair loss and hair loss in the anterior/mid area of the scalp. It may not be effective for men who are older than 60 years of age because type II 5α-reductase activity in the scalp may not be as high as that in younger men.
In postmenopausal women with androgenetic alopecia, finasteride 1 mg/day taken for 12 months did not increase hair growth or slow the progression of hair thinning. Finasteride is contraindicated in women who are or may potentially be pregnant because of the risk that inhibition of conversion of fetal T to DHT could impair virilization of a male fetus. Approximately 20% to 30% of men do not respond. Treatment must be continued indefinitely.
Side Effects.
Approximately 1.5% of men will experience sexual problems (impotence, decreased libido, and ejaculatory dysfunction) with finasteride use. In most men, these side effects resolve when the medication is stopped, however in some, the sexual symptoms and others persist. These persistent symptoms and physical findings are referred to as post-finasteride syndrome ( Table 24.4 ). The mechanism for post-finasteride syndrome is unknown, but may be related to decreased production of central neurosteroids, which regulate sexual desire and function, impaired T metabolism, and a relative excess of estrogen. The risk for finasteride sexual difficulties appears to increase with age and other side effects such as gynecomastia, testicular pain, and depression appear to be more common at higher doses (5 mg/day) used to treat benign prostatic hypertrophy. Further studies are needed to evaluate the true incidence and risk factors for post-finasteride syndrome.
| Sexual Symptoms | Physical Symptoms | Mental and Neurologic Symptoms |
|---|---|---|
|
|
|
Minoxidil Versus Finasteride.
A study showed that 2% minoxidil produced faster initial improvement in midfrontal/vertex AA in up to one third of treated patients, whereas finasteride produced marginally better results with increasing duration of treatment. Both agents were equally effective in stopping the progression of AA.
Dutasteride.
Dutasteride (Avodart) is a dual inhibitor of both type I and type II 5α-reductases, and thus inhibits conversion of T to DHT. Finasteride inhibits only type II 5α-reductase. Dutasteride is three times more potent than finasteride at inhibiting type II 5α-reductase. A study of men with male pattern hair loss, 20 to 50 years old, treated with dutasteride (0.5 mg) and finasteride 1 mg was conducted. In this study, dutasteride 0.5 mg was statistically superior to finasteride 1 mg and placebo. Dutasteride improved hair growth and was well tolerated.
Hair Transplants.
Hair transplants have been used successfully for years to permanently restore hair. Age is not a determining factor. Androgen-independent hairs from the lateral and posterior areas of the scalp are used. The surgeon must have a sense of aesthetics to properly design the anterior hairline. There are many techniques used for harvesting and implanting the grafts. The techniques are constantly changing and improving.
Scalp Reduction and Flaps.
An anterior–posterior elliptic excision of bald vertex scalp with primary closure can provide an instant hair effect. The procedure can be repeated every 4 weeks until hair margins converge or scalp tissue becomes too thin. Grafts or flaps may be used later to fill any remaining void. Alternately, several types of flaps can be designed by the creative surgeon to fill voids.
Hair Weaves.
Hair weaves have been refined by the Hair Club ( www.hairclub.com ) in the United States. They create a matrix of crisscrossing, transparent fibers, fitted and shaped to the client’s thinning area. The matrix is porous, allowing the scalp to “breathe.” New hair is added to the matrix strand by strand to recreate the pattern and hair flow of the client’s own hair. The matrix is then fused to the client’s remaining growing hair using a medical adhesive called Polyfuse. The client returns to Hair Club for haircuts and to replace the Polyfuse every 5 weeks.
Newer treatments include low level laser light therapy and platelet-rich plasma. Further studies will determine the efficacy to these treatments.
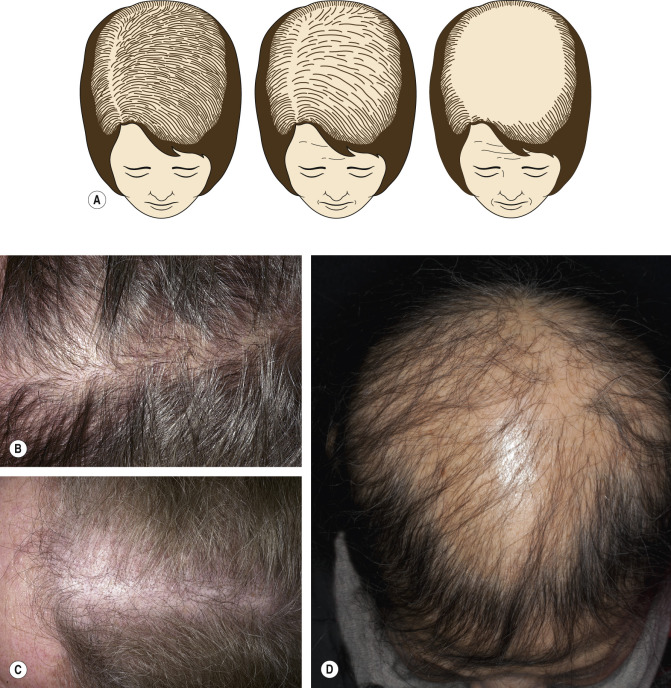
Female Pattern Hair Loss (Androgenic Alopecia in Women)
Chronic, progressive, diffuse hair loss in women in their twenties and thirties is a frequently encountered complaint. These women, who usually have a normal menstrual cycle and lack any abnormalities on physical examination and have normal androgen levels, have been classified as having “male pattern baldness,” a genetic trait, and have been dismissed without further evaluation. Studies have shown that some of these women have increased levels of the serum adrenal androgen dehydroepiandrosterone sulfate (DHEA-S) and a distinct pattern of central scalp alopecia, which has been called adrenal androgenic female pattern alopecia. Female pattern hair loss is more common in endocrine disorders resulting in androgen excess, such as polycystic ovarian syndrome (PCOS).
Male pattern baldness results in a gradual regression of the hair on the central scalp and gradual frontotemporal recession, as well as a gradual decrease in hair shaft diameter in the areas of hair loss. In contrast, most women with diffuse alopecia experience a gradual loss of hair on the central scalp, with retention of the normal hairline without frontotemporal recession. There are a variety of anagen hair diameters. With advancing age, the central thinning becomes more pronounced; in contrast to male pattern baldness, a fringe of hair along the frontal hairline persists ( Fig. 24.9 ). In exceptional cases, a course similar to that in men is seen, with deep frontotemporal recession.