Genodermatoses include a variety of skin conditions due to underlying genetic mutations with and without associated systemic findings. New gene mutations are being discovered rapidly and allow for more definitive diagnoses in many of these conditions; however, recognizing the salient features on physical examination allows for more directed genetic testing.
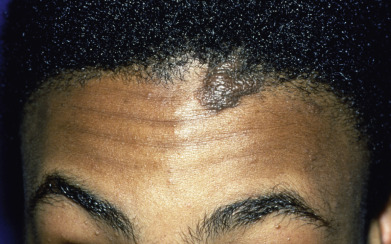
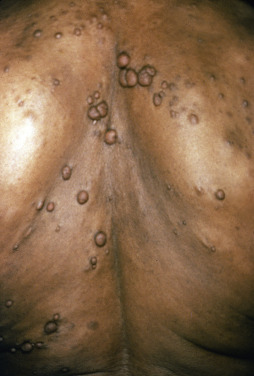
Some genodermatoses will present at birth, such as epidermolysis bullosa with skin fragility or congenital ichthyoses with the presence of a collodion membrane. Other conditions manifest distinctive clinical findings in the neonatal period, as seen in the Blaschko linear vesicular and verrucous eruptions indicative of incontentia pigmenti. Childhood onset is more common for conditions like tuberous sclerosis (TS) or neurofibromatosis when patients begin to demonstrate more noticeable clinical stigmata such as angiofibromas or neurofibromas, respectively. Still other genodermatoses can present later during adolescence or early adulthood, including Darier disease with keratotic and crusted papules and plaques and Hailey-Hailey disease (familial benign chronic pemphigus) with reticulated, eroded flexural plaques.
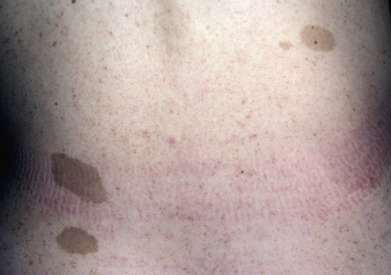
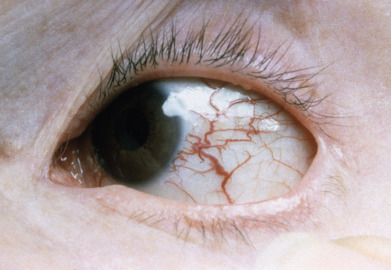
Photosensitivity can be seen in several genodermatoses, including the telangiectatic patches of Bloom syndrome; the poikiloderma of Rothmund-Thomson syndrome; and the lentigines, sun damage, and early skin cancers seen in xeroderma pigmentosa.
A thorough evaluation of these conditions should include examination of the hair, nails, mucosa, and teeth. Screening for associated symptoms is important, such as lack of sweating present in several forms of ectodermal dysplasia or developmental delays and seizures that can be present in several genodermatoses such as epidermal nevus syndrome or TS. Finally, family history can be useful in determining the inheritance pattern and to narrow genetic testing.
This portion of the atlas includes a wide variety of genodermatoses and congenital anomalies to aid the clinician in identifying the clinical clues that help differentiate these diseases and often guide genetic testing when appropriate.








































Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


