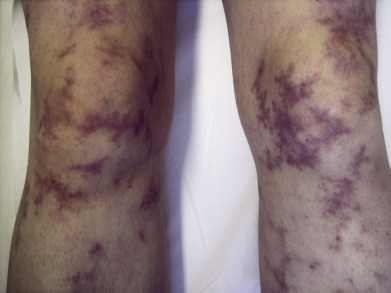
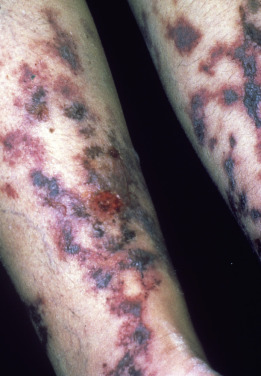
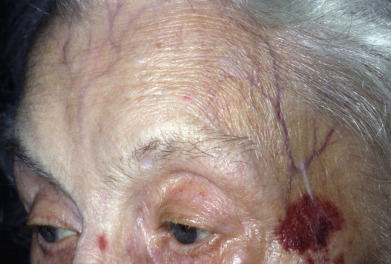
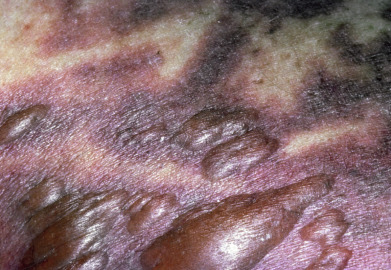
This section of the atlas will focus on vascular disorders of the skin, including such entities as Raynaud disease, erythromelalgia, livedo racemosa, livedoid vasculopathy, cryoglobulinemia, purpura fulminans, superficial thrombophlebitis, purpura, and vasculitis. As with other disorders of skin, the color, morphology, and distribution of skin lesions are critical to establishment of an accurate diagnosis. Immune complex–mediated disease often affects dependent areas of skin, whereas embolic and vasoconstrictive phenomena affect acral sites. Diseases affecting the post–capillary venule or capillaries seldom result in cutaneous necrosis and tend to produce lesions with a round-to-oval configuration, whereas diseases affecting arterioles commonly result in angular stellate infarcts and retiform purpura. Postcapillary venule disease results in petichiae, or palpable or macular areas of purpura, whereas chronic capillaritis presents with hemosiderin staining and thumbprint, annular, eczematous, or lichenoid-containing petechiae. Forms of vasculitis associated with a stellate or retiform morphology include antineutrophil cytoplasmic antibody–associated vasculitis, rheumatoid vasculitis, and septic vasculitis. Ischemic disease is often associated with pain, and severe or prolonged ischemia results in necrosis. Vasodilatation may relate to temperature regulation, abnormal shunting of blood, or small-fiber neuropathy, as in the case of erythromelalgia. The morphology and distribution of the lesions suggest the correct site and appropriate depth for a biopsy.