Chapter 80 Gait Analysis in Anterior Cruciate Ligament Deficient and Reconstructed Knees
Introduction
Anterior cruciate ligament (ACL) rupture is a common injury of the knee joint that usually results in surgical reconstruction.1,2 The goal of ACL reconstruction and subsequent rehabilitation is to restore the knee to an acceptable muscular strength and joint stability.3,4 The stability of the knee thought to have an ACL injury is traditionally evaluated with an arthrometer (i.e., KT-1000) while the patient is in a standard static position. The arthrometer provides the clinician with a quantitative measure of the amount of passive movement between the femur and the tibia. A minimal amount of joint laxity during the test is considered to be clinically and functionally acceptable. However, such an evaluation is a measure of passive joint stability and does not provide a measure of the joint’s stability during daily physical activities.5–7 Dynamic functional joint stability is defined as the condition in which the joint is stable during daily physical activities.5 Previous research has indicated that there is lack of a relationship between passive and dynamic functional joint stability.5,8–10
Recently, gait analysis has been used to quantify the dynamic functional knee stability after ACL reconstruction.11–14 Gait analysis can be defined as an advanced laboratory process by which present day electronics (i.e., video cameras) are used to integrate information from a variety of inputs in order to demonstrate and analyze the dynamics of gait (Fig. 80-1). For example, gait analysis can offer a more in-depth evaluation of movement patterns by providing information on each joint. Such information has also become common practice in many other orthopaedic areas where the effects of surgical procedures (i.e., joint arthroplasty, cerebral palsy) are evaluated to identify gains in mobility.15–19
The use of this technology allows the development of normal joint movement profiles that can be used to identify abnormalities, helping in this way to improve diagnosis, treatment, design, and performance of reconstructive surgery and rehabilitation programs. Gait analysis, using advanced computerized systems in conjunction with multiple high-speed (i.e., 200 frames per second) video cameras, can document three-dimensional (3D) knee joint movement profiles.20 Thus all six degrees of freedom of the knee joint can now be discerned, and the dynamic functional levels of individuals performing everyday activities can be objectively measured and evaluated. This is accomplished by obtaining data from surface markers that are placed on specific anatomical bony landmarks. The position of the markers in space is recorded, and then joint movement profiles can be acquired.
A possible limitation of gait analysis is that surface markers may not accurately represent the underlying bone motion during highly dynamic activities,21 as the markers are attached on the skin and not directly on the bone. As skin movement increases, the location of the marker and of the underlying bone differs. As a result, error is introduced.21–26 One way to avoid these limitations is to directly measure skeletal motion with intracortical pins.25 However, the applicability of this method is limited because the implantation of intracortical pins is a highly invasive procedure that may cause discomfort or pain to the patient and result in restriction of movements. In addition, implantation of intracortical pins is a method that is limited by the sample size, as an effective number of volunteers cannot be found.
These suggestions can solidify conclusions drawn from gait analysis. Thus gait analysis is widely accepted at the present time and is considered a well-established and reliable method.28,29 This methodology allows the in vivo evaluation of the ACL deficient and reconstructed knee during dynamic activities (i.e., walking, pivoting), something that static measures (i.e., arthrometer) are unable to do.
Importance of in Vivo Biomechanical Research to Quantify Success of Surgical Techniques
Example 1: Tibial Rotation
Our investigations have examined knee joint rotational movement patterns during high- and low-demand activities in both ACL deficient and reconstructed individuals. In our first study, we evaluated ACL deficient and reconstructed individuals during a low-demand activity such as walking.14 We examined 13 individuals with unilateral ACL deficiency, 21 individuals who had undergone ACL reconstruction, and 10 healthy controls. ACL reconstruction was done arthroscopically using a bone–patellar tendon–bone (BPTB) autograft. We found that the ACL deficient group exhibited significantly increased tibial rotation range of motion during the initial swing phase of the gait cycle when compared with the ACL reconstructed and control groups. Thus our results demonstrated that ACL deficiency produced rotational differences at the knee during walking. These differences did not exist when we compared the ACL reconstructed group with the control. Thus, in this low-demand activity, the surgical reconstruction restored tibial rotation to normal levels.
Next, we wanted to identify whether this is also the case in a higher-demand activity that can apply increased rotational loading at the knee. Therefore we examined 18 ACL reconstructed individuals and 15 controls during a high-demand activity (descending stairs and subsequent pivoting).27 The ACL reconstruction was done arthroscopically, again using a BPTB autograft. The evaluation was performed at an average of 12 months after reconstruction. The individuals were asked to descend three steps and then immediately pivot on the landing leg at 90 degrees and walk away from the stairway while kinematic data were collected. The tibial rotation range of motion during the pivoting period was found to be significantly larger in the ACL reconstructed leg compared with the contralateral intact leg and the healthy control. No significant differences were found between the healthy control leg and the intact leg of the ACL reconstructed group. Therefore our results demonstrated that tibial rotation remained abnormal and significantly increased 1 year after ACL reconstruction during high-demand activities such as pivoting after descending from stairs.
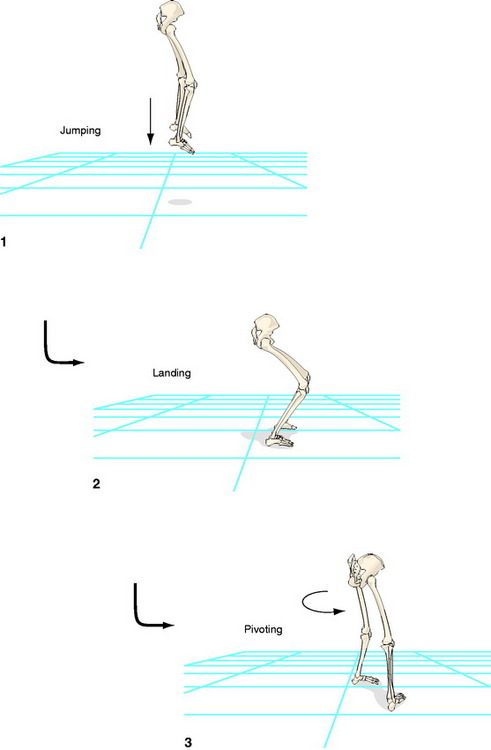
To verify our findings, we performed an additional experiment in which we evaluated another high-demand activity.30 Data were collected while the subjects jumped off a 40-cm platform and landed on the ground; following foot contact, they immediately pivoted at 90 degrees and walked away from the platform. We chose this activity because landing from a jump is a task that places higher demands on the knee than walking or even stepping down.31,32 We combined landing with a subsequent pivoting to create rotational loads on the knee. The subjects were 11 patients, all ACL reconstructed with the same arthroscopic technique using a BPTB autograft, 1 year after the surgery; 11 ACL deficient subjects who had sustained the injury more than 1 year prior to testing; and 11 controls. The same dependent variable was evaluated as in the previous study.27 Both the reconstructed leg of the ACL group and the deficient leg of the ACL deficient group had significantly larger tibial rotation values than in the healthy control group. We also found no significant differences between the deficient leg of the ACL deficient group and the reconstructed leg of the ACL reconstructed group. It was concluded that current ACL reconstruction using the BPTB autograft is inadequate to restore excessive tibial rotation during an activity such as landing and subsequent pivoting, which practically simulates sport activities.
Next, we wanted to identify whether tibial rotation remains excessive for a longer period: 2 years following the reconstruction. We speculated that it is possible adaptations will set in and the patients will compensate. Thus we performed a follow-up evaluation33 in nine ACL reconstructed subjects who had participated in our previous study.30 We examined them with the same methodology and for both activities that we used in our previous work.27,30We also incorporated a control group of 10 individuals. We found that tibial rotation remained significantly excessive even 2 years after the reconstruction. This result was verified with comparisons conducted with both the intact contralateral knees of our patient group and with the healthy controls. Furthermore, we found that tibial rotation of the intact knee of our patient group was similar to those recorded from the healthy control group.
In all of our previous work, ACL reconstruction was performed with a BPTB autograft. Thus it was logical to question whether tibial rotation will remain excessive if an alternative autograft is used. Such an autograft is the quadrupled hamstring tendon (semitendinous and gracilis [ST/Gr]). Originally we hypothesized that the ST/Gr autograft would be able to restore tibial rotation during our experimental protocols due to its superiority in strength and linear stiffness34–37 and because it is closer morphologically to the anatomy of the natural ACL.34–36 We examined 11 individuals who were ACL reconstructed with an ST/Gr autograft, 11 individuals who were ACL reconstructed with a BPTB autograft, and 11 healthy controls.38,39 The experimental protocol was identical to our previous studies. Tibial rotation was found to be significantly larger in both ACL reconstructed groups when compared with the healthy controls. Therefore our hypothesis was refuted, and we concluded that ACL reconstruction using the ST/Gr autograft is as inadequate as the one using the BPTB autograft in terms of restoring excessive tibial rotation.
The results of our studies were also supported by in vitro research work in which the biomechanical efficiency of the ACL reconstruction has also been questioned.40–43 These studies showed that ACL reconstruction was successful in limiting anterior tibial translation in response to an anterior tibial load but was insufficient to control a combined rotatory load of internal and valgus torque. Furthermore, our tibial rotational values were in close agreement with the in vitro work.40
Example 2: Dynamic Functional Knee Stability Using Nonlinear Analysis
Biomechanists have recently proposed that the use of stride-to-stride variability, defined as fluctuations on the walking movement patterns from one stride to the next, provides a quantitative measure of functional joint stability.44–47 This proposal is based on scientific evidence that neuromuscular pathology is related to an increased amount of stride-to-stride variability.44–47 Hence a “biomechanical” hypothesis has been formed in which neuromuscular pathology is related to an increased amount of variability and deterioration of functional stability. However, this biomechanical hypothesis lacks support in other medical domains. Numerous studies in diverse medical areas have shown that a decreased amount of variability is related to pathology. These investigations include medical domains such as heart rate irregularities, sudden cardiac death syndrome, blood pressure control, brain ischemia, and epileptic seizures.48–55 Hence a contradictory hypothesis has been proposed in which variability is described as “healthy flexibility.”56–58 These investigations indicate that variations in the behavior of the biological system may be necessary to provide flexible adaptations to everyday stresses placed on the human body. Alternatively, a lack of healthy flexibility is associated with rigidity and inability to adapt to stresses. Based on this logic, it is possible that injury or pathology can result in a loss of healthy flexibility that may not be regained despite surgical treatment (loss of complexity hypothesis).
This contradiction in the literature may be due to the usage of linear tools (i.e., standard deviation) to assess stride-to-stride variability.44–47 Linear tools only provide a measure of the amount of variability that is present in the gait pattern and may mask the true structure of motor variability. Masking occurs when strides are averaged to generate a “mean” picture of the subject’s gait. This averaging procedure may lose the temporal variations of the gait pattern. Additionally, the statistical processing of linear measures requires random and independent variations between subsequent strides.
Recent studies have overcome the problems of linear measures by using nonlinear tools such as the Approximate Entropy.59–62 These studies have determined that variations in the gait pattern are distinguishable from noise and have a deterministic origin. A deterministic origin indicates that stride-to-stride variations are neither random nor independent. Rather, these variations have a meaningful pattern that characterizes the behavior of the locomotive system. Linear tools are not able to provide such information. Thus the ability to quantify the characteristic features of these variations has been the strength of using nonlinear tools to support the “loss of complexity” hypothesis.
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
 Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
 High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


