Fully Laparoscopic Donor Nephrectomy
Bonnie E. Lonze
Dorry L. Segev
DEFINITION
Donor nephrectomy is defined as the en bloc removal of a native kidney, its renal artery and vein, and the majority of its ureter and mesoureter from a healthy individual for purposes of living donor renal transplantation. A fully laparoscopic donor nephrectomy is one in which the entirety of the operation is accomplished laparoscopically, through the peritoneal cavity, without the aid of a hand port.
PATIENT HISTORY AND PHYSICAL FINDINGS
Candidates for donor nephrectomy undergo a thorough evaluation to determine appropriateness for donation. This is initiated when an individual, of his or her own volition, presents expressing a desire to donate. The primary objective of the donor evaluation is to determine whether kidney donation is safe for the individual wishing to donate, to counsel the donor regarding risks of donation, and to ensure the decision to donate has been made free of coercion. Therefore, patients who are deemed high operative risk due to medical comorbidities or who are at risk to develop kidney disease after donation are not considered candidates for donation. Detailed donor selection criteria as well as a discussion of donor and recipient compatibility are outlined in the chapter entitled, “Chapter 4, Laparoscopic Hand-Assisted Donor Nephrectomy.”
IMAGING AND OTHER DIAGNOSTIC STUDIES
Candidates for living kidney donation undergo a computed tomography (CT) angiogram to delineate the vascular anatomy.1 Renal ultrasound may be used in addition to evaluate for the presence of stones or other abnormalities but is not invariably required.
SURGICAL MANAGEMENT
Preoperative Planning
Whether the right or the left kidney is donated is determined by the vascular anatomy and the presence of any imperfections, such as stones or renal cysts, in either kidney. In general, the anatomically and structurally “best” kidney should remain with the donor. If both kidneys are equal, the left kidney is preferentially chosen for donation. The left-sided nephrectomy is usually technically easier, in part because the liver makes a right-sided dissection more challenging. In addition, the left renal vein is longer, which is desirable for the subsequent transplant operation.
Prior to transportation to the operating room, patients are administered a single injection of subcutaneous heparin for deep venous thrombosis prophylaxis.
A Foley catheter is placed once the patient is under general anesthesia.
Positioning
For purposes of simplicity, a left nephrectomy is described in detail here. Specific differences relevant to the right nephrectomy are described at the end of the section.
Mark the kidney extraction incision while in the supine position—a 6- to 8-cm Pfannenstiel incision centered on a point 1 or 2 cm above the upper pubic symphysis. Once in the decubitus position, the incision can be inadvertently distorted, so it is important to mark the incision while supine.
Use a modified lateral decubitus position with the left side up. Extend the right arm and carefully pad and tuck it. Elevate the left arm, flex it at the elbow, and support it by a Krause arm board (FIG 1). Care must be taken to appropriately pad the elevated arm and avoid any traction at the shoulder. Other options for padding and supporting the patient in a lateral decubitus position such as using a beanbag or supporting the patient with pillows are appropriate alternatives.
Secure the patient to the bed across the chest and upper and lower legs, because the majority of the case is carried out with the operating table airplaned right side down approximately 45 degrees. A “test roll” should be carried out before the patient is draped to ensure stability of the patient.
 FIG 1 • Modified lateral decubitus positioning is used. For left nephrectomy, the right arm is tucked and the left arm is abducted, flexed at the elbow, and rested on an arm support. The table is rotated right side down for the majority of the operation. |
TECHNIQUES
ENTRY INTO THE ABDOMEN AND PORT PLACEMENT
Use chlorhexidine skin preparation. Administer cefazolin (or clindamycin if penicillin allergic) prior to incision. For a left-sided nephrectomy, place four ports (FIG 2). The umbilical and left lateral ports are 12 mm. A 5-mm port is introduced below the xiphoid in the midline. These three ports are secured to the skin with a suture to prevent sliding in and out of the skin, as instruments are frequently exchanged throughout the operation. Place the fourth port (12 mm) in the Pfannenstiel incision as described in the following text.
Make the Pfannenstiel skin incision and dissect down to the fascia with electrocautery. Raise suprafascial flaps over an area large enough to permit a vertical fascial incision at the time of kidney extraction. Introduce the port directly through the fascia in the center of this incision. An endo fan retractor can be inserted through this port for retraction, or the port can be replaced by the EndoCatch device, which can also function as a retractor.
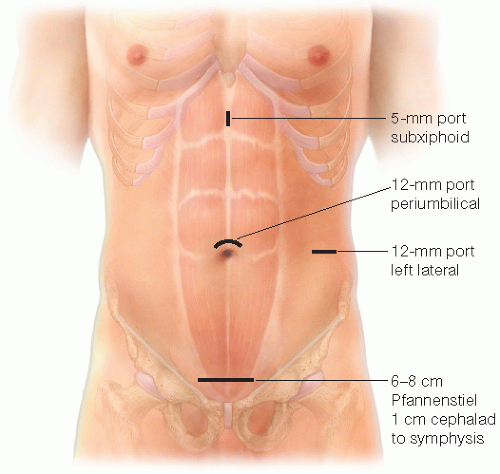 FIG 2 • Port placement for left laparoscopic donor nephrectomy. |
MOBILIZATION OF THE COLON
Gently grasp and retract the left colon medially and divide any attachments to the lateral abdominal wall (FIG 3). Perform a medial visceral rotation whereby the left colon is separated from the kidney and ureteral pedicle. Care must be taken not to injure the transverse mesocolon (FIG 4). Mesenteric defects, if created, must be closed. If performed properly, medialization of the colon can be accomplished in a bloodless fashion.
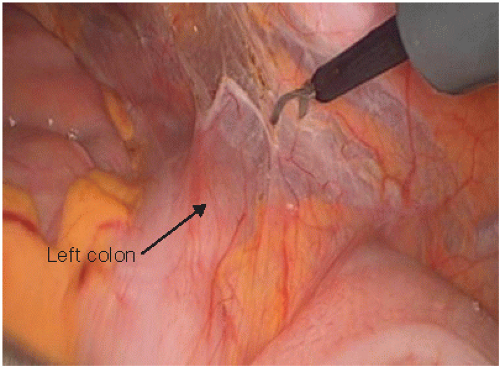 FIG 3 • Mobilization of the colon is initiated by medial retraction of the colon and division of attachments to the lateral abdominal wall. |
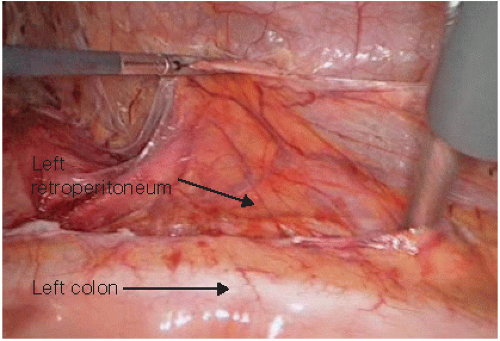 FIG 4 • The mesocolon is bluntly separated from the mesoureteral structures in an avascular plane. |
MOBILIZATION OF THE URETERAL PEDICLE
Develop a plane medial to the ureteral pedicle using blunt dissection. Mobilize the ureter, mesoureter, and gonadal vein off of the psoas muscle, which lies posteriorly (FIG 5). Begin the mobilization distally at the point of eventual transaction of the ureter near where it crosses over the iliac vessels. Work proximally toward the hilum of the kidney (FIG 6).
As the renal hilum is approached, identify the insertion of the gonadal vein into the renal vein (FIG 7). A small artery is often identifiable and encountered as the ureteral pedicle approaches the renal hilum. Ligate this artery with clips and divide it. Small lumbar branches off the gonadal vein or renal vein are frequently present. Divide these veins either between clips, seal and divide them with a thermal device such as the LigaSure, or staple them with an endovascular stapler if of large enough caliber. When ligating lumbar veins, care should be placed to position clips so that they do not interfere with the eventual need to staple the renal hilar vessels.
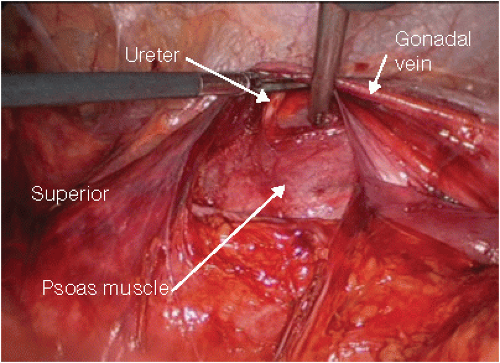 FIG 5 • The ureteral pedicle is elevated off of the psoas muscle. |
 FIG 6 • The ureteral pedicle is mobilized along its length, working proximally toward the hilum of the kidney.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|