| Poor levator function ptosis, <5 mm |
|
| Amblyopia in visually maturing children |
| Functional ptosis affecting vision |
| Prior facial surgery or trauma |
| Dry eye symptoms/lagophthalmos present |
| Quality of Bell’s phenomenon (particularly with myogenic etiologies) |
| Prior refractive surgery |
| Co-existent dermatochalasis |
| Amount of levator function (consider for less than 5 mm function) |
| Extraocular motility (may unmask diplopia with ptosis repair) |
| Brow position and frontalis muscle function |
| Allergy/prior reaction to silicone |
| Corneal examination |
| Cardiac clearance with Kearns–Sayre syndrome |
| Potential for revision/asymmetry |
| Maximize medical management of myasthenia gravis |
Introduction
Frontalis suspension surgery is primarily indicated for ptosis associated with poor levator function (less than 5 mm). Table 15.1 summarizes some of the indications for surgery. In this ptosis repair technique, the powerful lifting ability of the frontalis muscle is coupled to the tarsal plate to provide eyelid elevation. The quality of the Bell’s phenomenon should be carefully evaluated preoperatively to minimize corneal damage from postoperative lagophthalmos. A poor Bell’s phenomenon is often seen with double elevator palsy, CPEO, OPMD, myotonic dystrophy, cranial nerve III palsy and myasthenia gravis, so exercise caution in these patients. Unmasking of binocular diplopia may also occur with eyelid elevation, necessitating careful preoperative evaluation of extraocular motility and ocular misalignment. For patients with Kearns-Sayre syndrome, preoperative clearance should be obtained to rule out associated cardiac arrhythmias. Medical management of patients with myasthenia gravis should be maximized first prior to considering frontalis suspension.
For congenital ptosis with levator function greater than 5 mm, consider levator resection as a primary operation first ( Chapter 14 ). Two commonly used sling materials include silicone rod and autologous or donor fascia. Autologous fascia lata should not be harvested in patients younger than 5 years of age. The benefits of autologous fascia lata are biocompatibility and durability, but are complicated by the difficulty with revision and donor-site morbidity. Silicone rod allows for postoperative eyelid height adjustment and no donor-site complications but may be susceptible to breakage, extrusion, and allergic reactions.
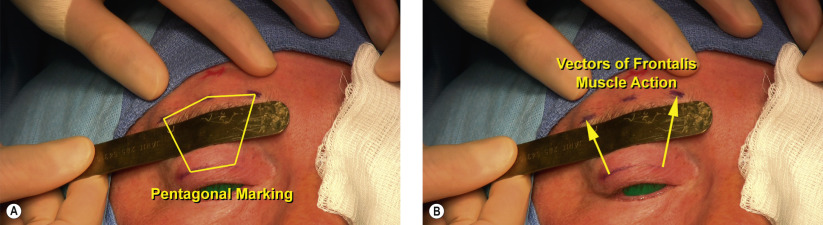
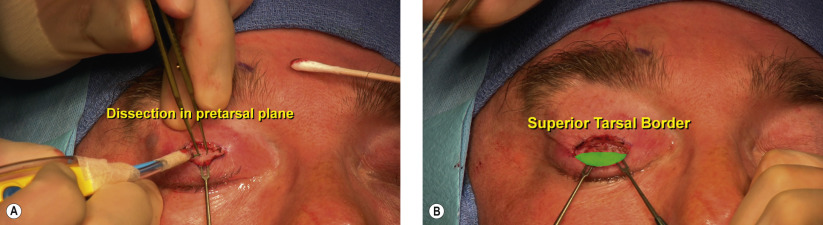
Surgical Technique
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


