Key Words
breast reconstruction, free flap breast reconstruction, abdominally based breast reconstruction, free TRAM, MS-TRAM
Introduction
Abdominally based reconstructions have been utilized for the last 40 years. In 1979, Holstrom used tissue normally discarded from abdominoplasty as a free flap for breast reconstruction. In 1982, Hartrampf described and popularized the pedicled TRAM (transverse rectus abdominis muscle) flap. In 1989, Grotting improved upon the design and began using free TRAM flaps based off the deep inferior epigastric artery (DIEA) as opposed to the superior epigastric arteries (as in the pedicled TRAM). The advantages included improved blood supply, more limited muscle harvest, and fewer complications than the pedicled version. The final iteration evolved into a perforator flap, described by Allen and Treece in 1994 as the deep inferior epigastric artery perforator (DIEP) flap, to minimize abdominal donor site morbidity.
As one can infer from the historical modification, there are many differing flaps that are available from the abdomen, ranging from pedicled versions to perforator-based free flaps. The pedicled TRAM flap based off the superior epigastric artery is associated with the most abdominal wall morbidity. It also has higher partial flap loss and fat necrosis rates, as the superior epigastric artery is the non-dominant blood supply. This option is likely better reserved for when microsurgery is not available or feasible. If microsurgery is an option, the free flap versions are preferable reconstructions, and are based off the blood supply from the DIEA. Advantages include improved blood supply, easier flap manipulation, and more mobility for flap inset. However, the use of microsurgery makes this option more challenging, resulting in a longer operation with a higher risk of total flap loss. In this chapter, we will discuss the indications for a free TRAM and the preoperative evaluation, describe the relevant surgical anatomy and the procedure, and review the postoperative care and management of complications.
Indications and Contraindications
In our practice, most patients are candidates for free or MS-TRAM breast reconstruction, presuming that they have an appropriate amount of abdominal donor tissue and do not have multiple of the previously mentioned risk factors. High-risk patients include active smokers, the obese, those requiring postoperative radiation, patients with hypercoagulable states, and those who have had prior abdominal surgery. Smokers are at higher risk of mastectomy skin necrosis, fat necrosis, and abdominal flap necrosis. Obese patients (BMI >30) are at higher risk for mastectomy skin necrosis, donor- and recipient-site complications, and partial flap loss. Patients who need radiation will experience dermal fibrosis and possible changes in flap volume. Patients with a prior history of abdominal surgery have a higher rate of delayed healing, typically requiring greater amounts of muscle to be harvested. Preoperative imaging should be considered in this patient group. Age has not shown to be a risk factor for autologous breast reconstruction, although patients over age 65 have a higher rate of venous thromboembolism and hernia.
Although not a contraindication to autologous reconstruction, a significant dilemma are patients with large breasts and small, insufficient donor sites to provide tissue to rebuild their mastectomy defect. We offer these patients several options, the most common of which is to use stacked flaps to reconstruct a unilateral breast, with one antegrade and one retrograde anastomosis. For bilateral reconstructions, a latissimus flap combined with an abdominal free flap, stacked free flaps from multiple donor sites, and free flaps with fat grafting and/or implants are all options.
Another challenging group are patients with a history of thrombotic conditions and/or a history of deep vein thrombosis (DVT)/pulmonary embolism (PE). Approximately 5%–10% of the population is estimated to have a hypercoagulable state, although in many it is unrecognized preoperatively. We still offer these patients microvascular breast reconstruction, but our perioperative management changes. These patients are counseled that they are about 5 times more likely to have a thrombosis than the average patient (approximately 20% of hypercoagulable patients at our institution) and have a much higher risk of flap loss if a thrombosis occurs (15.5% vs 1.8%). Our intraoperative management of these patients includes the addition of a heparin bolus and a heparin drip continued postoperatively. Our studies have shown that this reduces flap loss rates to the range seen in patients with normal coagulation profiles, but increases the risk of postoperative blood transfusion. Postoperative management ranges depending on the nature of their thrombotic conditions but typically includes heparin drips, therapeutic doses of enoxaparin, aspirin and/or clopidogrel.
Preoperative Evaluation
All patients undergo standard medical clearance for surgery, and patients with cardiac or pulmonary co-morbidities require subspecialty clearance. Obese patients are considered on a case-by-case basis depending on their body mass index and the distribution of their body fat. The only people we will not operate on are those who are not medically cleared for surgery.
Patients who require postoperative radiation are still candidates for free MS-TRAM flaps. In these patients, timing of the reconstruction in relation to radiation is a consideration. Traditionally, these patients were only offered delayed reconstruction about 6 months after completion of post-mastectomy radiation. Many patients who present to our practice have been treated with mastectomy and radiation at outside institutions and are candidates for delayed breast reconstruction. In patients who present to us before they undergo mastectomy and radiation, we offer them a choice of delayed or immediate reconstruction. Those who choose immediate reconstruction are advised about the potential for radiation to cause changes to their flap that may alter the final aesthetics.
Another consideration when assessing these patients before surgery is whether imaging is required for surgical planning. Many surgeons choose to preoperatively image patients with a computed tomography angiogram (CTA) to aid in surgical planning, as it can help with perforator row choice, spare muscle, and speed dissection. However, this is controversial due to cost, nephrotoxicity of the contrast dye, and radiation exposure. We do not routinely image patients as we feel we can identify intraoperatively which row or rows of perforators to take with or without a small amount of rectus muscle. The exception is patients with multiple abdominal surgeries where perforators or deep inferior epigastric (DIE) vessel patency are questionable. In most instances, patients are offered or undergo an MS-TRAM. Essentially, we no longer perform a free TRAM unless the perforators are violated and we feel the flap requires the entire muscle to achieve viability.
There are a few clear-cut indications for MS-TRAM over DIEP, and these include patients with multiple small perforators scattered throughout the rectus muscle, patients requiring large reconstructions (>1000 g), patients who smoke and/or those who will require post-mastectomy radiation therapy. Because of the inclusion of more muscle and therefore blood supply, perfusion of MS-TRAM is better than for the DIEP. Studies assessing muscle function have shown muscle harvest to be associated with weakness, but the clinical correlation has not been proven and patient questionnaire studies have been equivocal.
Surgical Techniques
Relevant Surgical Anatomy
Donor Site Blood Supply
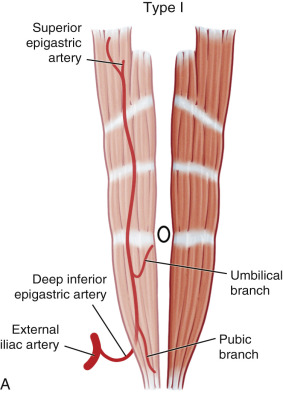
The blood supply of the free and MS-TRAM flaps are based on the DIEA. The difference between the two flaps depends on how much muscle is taken with the flap, as described in the introduction. The DIEA has three different branching patterns ( Fig. 2.1 ): type I, where the DIEA is a single intramuscular vessel; type II (the most common), where the DIEA splits into two distinct intramuscular branches; and type III, where the DIEA divides into three branches. The most common pattern is currently described as the medial and lateral rows, and it is from these rows that the perforators branch into the adipose tissue and supply the flap skin via the subdermal plexus. As you would expect based on their location, medial perforators are more likely to perfuse across the midline, while lateral perforators are more likely to perfuse the lateral/distal portion of the flap. Venous drainage follows the arterial system and typically both the superficial epigastric and deep epigastric veins are connected by the venae comitantes to drain the flap.
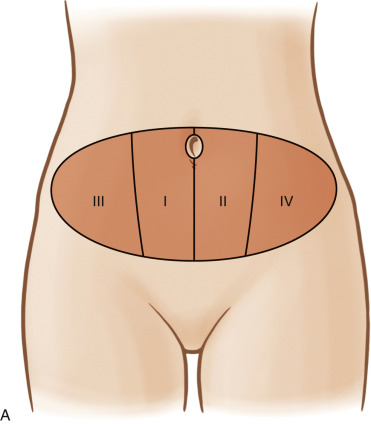
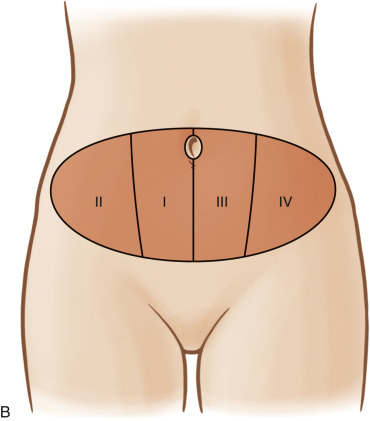
Classically, the arterial supply has been documented into cutaneous zones ( Fig. 2.2 ). Originally, these zones were named by Hartrampf and were considered for pedicled TRAM flaps, with zone I being directly on top of the muscle, zone II on the contralateral muscle, zone III lateral to zone I, and zone IV lateral to zone II. Ninkovic and Holm re-classified to have zone I directly on muscle and zone II the adjacent lateral zone, which is more pertinent to free flap morphology.
Recipient Vessels
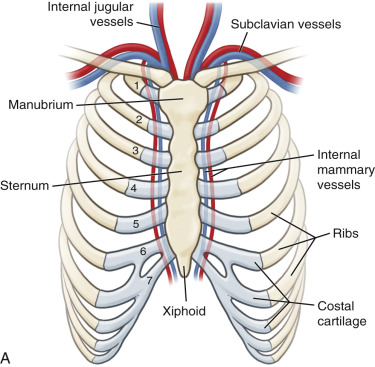
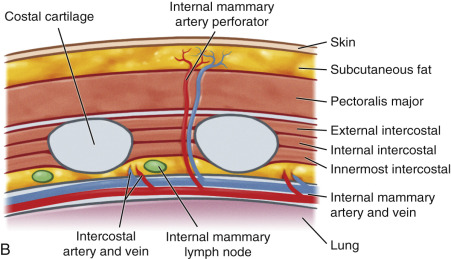
There are options to choose from in terms of recipient vessels to anastomose the flap. Historically, the thoracodorsal vessels were used but there has been a shift to using the internal mammary (IM) vessels. Either vessel is usable but IM flow is higher, which is preferable if a retrograde anastomosis is necessary. IM and thoracodorsal vessels are similarly sized (1–2.5-mm artery and 1–4-mm vein) and are both considered large vessels with reliable flow. The IM artery has consistent size between 3rd and 5th interspace with a vein bifurcating at 4th interspace. The IM vessels have a predictable location, they are usually in a low scarred area and easy to get to, and they can help with breast aesthetics by allowing the flap to be inset in a more medial position to re-create cleavage. Conversely, inflow injury can happen if the patient has a thoracodorsal anastomosis and ends up needing an axillary dissection, although there is a small risk of inadvertent pleural entry and pneumothorax with the IM vessels. Fig. 2.3 shows the internal mammary artery anatomy.
Different Varieties of the Free TRAM
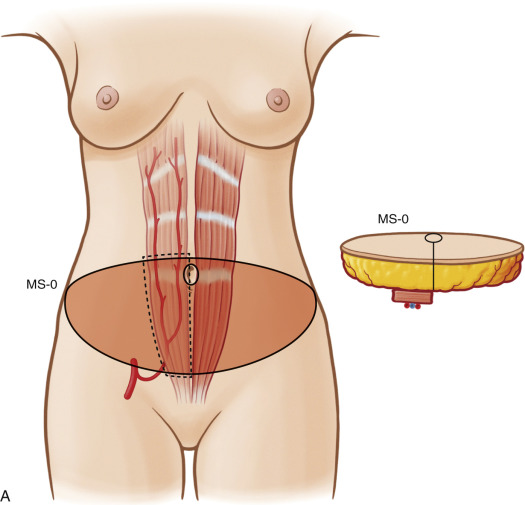
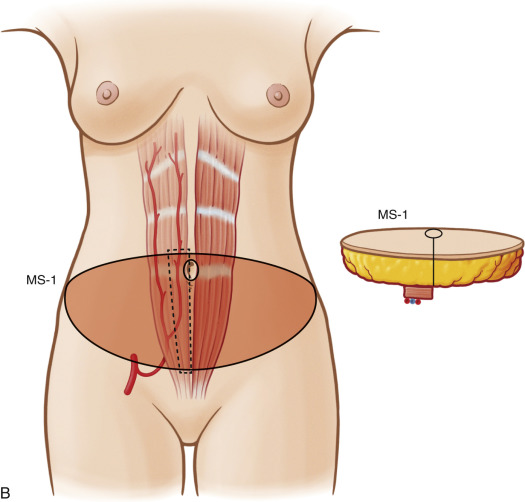
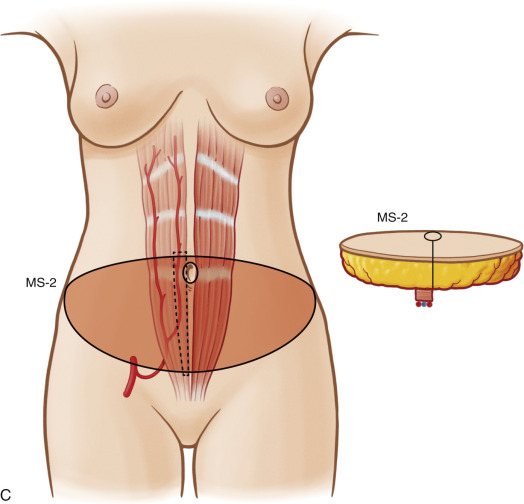
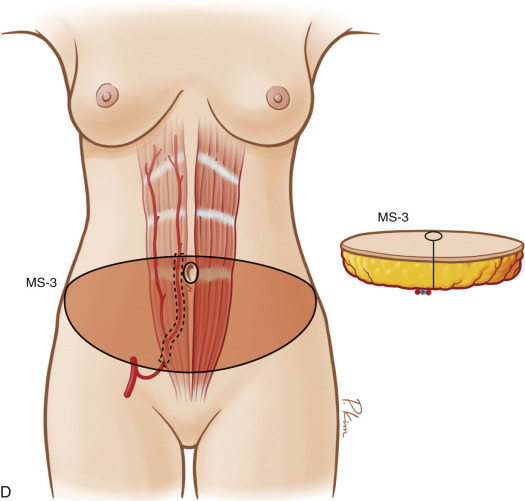
There are different varieties of the free TRAM depending on how much of the muscle is either utilized or spared. Following the classification system described by Nahabedian ( Fig. 2.4 ), the MS-0 takes full width of rectus, MS-1 preserves lateral or medial segment, MS-2 preserves some of both lateral and medial segments, and MS-3 preserves the whole muscle (a perforator flap like the DIEP). There are specific advantages and disadvantages for each option. The MS-0 free TRAM takes the entire width of the muscle, therefore preserving the entire vascular supply. This option is best for patients who may be at risk for partial flap loss with the more muscle-sparing techniques. It sacrifices the entire width of muscle like the pedicled TRAM but is less prone to fat necrosis. These patients are more likely to be able to perform a sit-up than a patient with a pedicled TRAM, although most studies showed no objective difference in muscle strength. Overall, free TRAM patients report good satisfaction and would have made the same reconstructive decision again. Muscle-sparing versions (MS-1 and MS-2) of the free TRAM maintain a portion of the neurovascular supply, therefore preserving more muscle and decreasing abdominal wall morbidity. The DIEP (MS-3) spares all muscle. The major advantage of this technique is less abdominal wall morbidity, yet this operation has decreased vascularity with a higher risk of venous insufficiency, partial flap loss, and fat necrosis compared with free TRAM flaps. In addition, this operation is more technically challenging and time consuming.
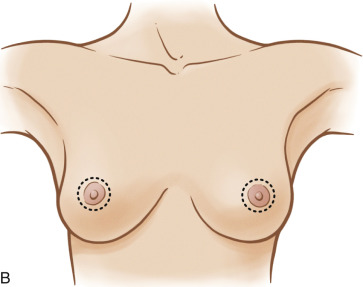
Preoperative Markings
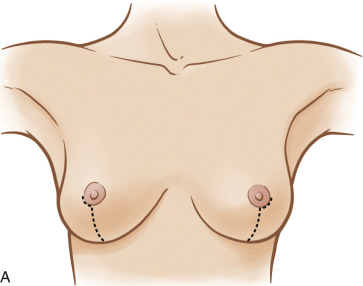
We mark our patients in a standard fashion and make modifications depending on the patient’s body habitus. For immediate reconstruction patients, we mark the midline and the inframammary fold (IMF) with a solid line and sometimes use hash marks to define the upper breast borders when the patient is in standing position. The mastectomy incision pattern is marked in a variable fashion depending on whether the patient is a candidate for nipple-sparing mastectomy, skin-sparing mastectomy, or whether she needs skin resected to treat her malignancy. For nipple-sparing mastectomy patients we favor a periareolar incision that starts a quarter of the way around the areola and extends inferiorly. For skin-sparing mastectomy patients, the patient’s degree of ptosis will also dictate the type of incision to be made. For those with no or mild ptosis, we choose a periareolar incision, and for moderate or severe ptosis, we utilize a circumvertical incision pattern ( Fig. 2.5 ). The abdomen is marked with the patient in the standing position. The superior incision is marked to incorporate the periumbilical perforators. The inferior incision is marked with the pinch test and confirmed intraoperatively with the patient in the Fowler position.
Related posts:
 Free Transverse Upper Gracilis Flap Breast Reconstruction
Free Transverse Upper Gracilis Flap Breast Reconstruction
 Immediate Implant Breast Reconstruction – One-Stage
Immediate Implant Breast Reconstruction – One-Stage
 Partial Breast Reconstruction With Local Tissue Rearrangements
Partial Breast Reconstruction With Local Tissue Rearrangements
 Immediate Prepectoral Implant Breast Reconstruction
Immediate Prepectoral Implant Breast Reconstruction
 Fat Grafting for Total Breast Reconstruction
Fat Grafting for Total Breast Reconstruction
 Partial Breast Reconstruction With Flaps
Partial Breast Reconstruction With Flaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


