Key Words
DIEP flap, microsurgery, breast reconstruction, flaps
Introduction
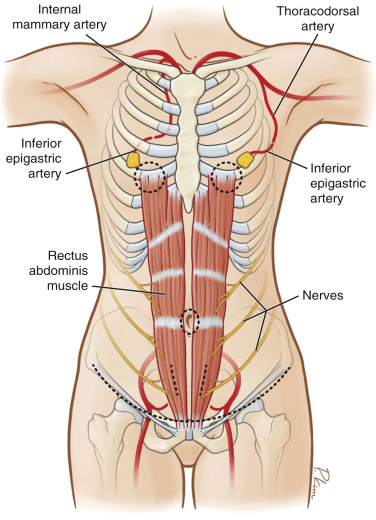
Breast reconstruction using the deep inferior epigastric perforator (DIEP) flap has become the gold standard for autologous breast reconstruction for most plastic surgeons. The principle benefit of the DIEP flap compared to other flaps is that the abdomen is the preferred and favorable donor site for most women because many will achieve an improvement in abdominal contour with minimal impairment in function. The DIEP flap utilizes the skin and fat from the lower abdomen but does not harvest any of the underlying rectus abdominis muscle. The deep inferior epigastric artery and vein are dissected away from the muscle, thus preserving the continuity and innervation of the rectus abdominis.
This chapter will provide an in-depth review of the DIEP flap and provide case examples to assist the reader with understanding the risks and benefits of this operation. Other relevant topics will include a review of algorithms, monitoring techniques, and the current technological advancements that have facilitated the ability to perform this operation.
Indications and Contraindications
Indications for the DIEP flap are numerous and include but are not limited to patient demand, dissatisfaction or failure of prosthetic devices, and previous radiation therapy. Although autologous reconstruction is performed less frequently than prosthetic reconstruction, many patients do not want prosthetic devices and prefer using their own tissues. DIEP flaps can be performed immediately following mastectomy or on a delayed basis. This flap is considered in patients with a variety of breast sizes and ultimately depends upon the amount of skin and fat available in the abdominal area to reconstruct a breast of desired shape, volume, and contour.
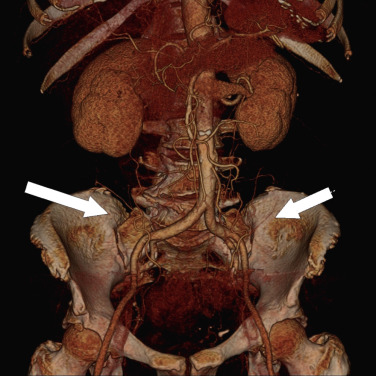
Contraindications to the DIEP flap are mildly controversial. Some surgeons feel that DIEP flaps should not be performed immediately following a mastectomy if postoperative radiation therapy is likely due to the possibility of flap shrinkage and soft tissue distortion; however, others feel that these adverse events are infrequent and therefore perform the DIEP flap regardless of radiation. Other contraindications to performing the DIEP flap include the lack of a suitable perforator. This can be assessed preoperatively using vascular imaging modalities such as computerized tomographic angiography (CTA) or magnetic resonance angiography (MRA). In patients with severe abdominal lipodystrophy with a large pannus, the DIEP flap may not be ideal due to the thickness of the flap and the likelihood of fat necrosis; however, proper tailoring of the flap can minimize these adverse events. Prior abdominal surgery is usually not a contraindication to performing a DIEP flap unless there is a paramedian incision that has violated the system of deep perforators. Midline abdominal incisions often facilitate the performance of bilateral DIEP flaps but may limit the amount of available tissue for unilateral DIEP flaps. Patients with elevated body mass index (BMI 30–35) are usually good candidates for this flap; however, when BMI exceeds 35, adverse events such as seroma, infection, and delayed healing may increase.
Advanced patient age (>65 years) is considered by some to be a relative contraindication for DIEP flaps. Active tobacco use is a relative contraindication and is typically associated with delayed healing of the mastectomy skin flaps as well as the abdominal donor site.
Preoperative Evaluation and Special Considerations
Patient selection includes a thorough history and physical examination, review of the reconstructive options, an understanding of patient expectations, and surgeon recommendations. Important details of the physical examination include body weight, patient height, body mass index (BMI), and estimated breast volume. Given the variation in breast size and body habitus, an understanding of symmetry following the first operation or subsequent operations is determined. The abdomen is the preferred donor site for most surgeons and patients and the DIEP flap is usually the best option. The most important physical finding related to the abdomen is a sufficient quantity of skin and fat to reconstruct the desired breast volume. Most women have experienced childbirth and have an excess of abdominal skin and fat. Although a woman may be slender, with a paucity of abdominal fat, she may still be a candidate for a DIEP flap if the reconstructive requirements are low. In women who are overweight or obese, a DIEP or free TRAM flap may be considered; however, the flap must be tailored to sustain adequate perfusion throughout to minimize the incidence of fat necrosis.
The decision as to whether to use a perforator flap or a musculocutaneous flap can be difficult. The author’s original algorithm was based on breast volume, abdominal fat volume, perforator diameter, number of perforators, patient age, tobacco use, and whether the reconstruction is unilateral or bilateral. In general, a DIEP flap is performed when the volume requirement is less than 1000 cc and the patient has mild to moderate abdominal lipodystrophy. A muscle-sparing free TRAM flap is usually performed when the volume requirement exceeded 1000 cc or if the patient has severe abdominal lipodystrophy ( Table 3.1 ). The author’s indications for a pedicle TRAM and superficial inferior epigastric artery perforator flap are also included. In this author’s practice, the DIEP flap constitutes approximately 70% of all abdominal flaps followed by the muscle-sparing (MS-2) free TRAM ( Fig. 3.1 ).
| Factor | Pedicle TRAM | Free TRAM | DIEP | SIEA |
|---|---|---|---|---|
| Breast Volume Requirement | ||||
| <1000 g | Yes | Yes | Yes | Yes |
| >1000 g | Yes with delay | Yes | Maybe | No |
| Quantity of Abdominal Fat | ||||
| Mild to moderate | Yes | Yes | Yes | Yes |
| Severe | Yes with delay | Yes | Maybe | Maybe |
| Perforators | ||||
| None | Yes | Yes | No | No |
| One | Yes | Yes | Yes | Yes |
| Two or more | Yes | Yes | Yes | Yes |
Preoperative Imaging
With the introduction of perforator flaps, preoperative imaging has proved to be useful to identify the location and caliber of the perforating vessels. Preoperative imaging enables surgeons to identify suitable perforators and to determine the patency of primary source vessels, namely the inferior epigastric and internal mammary vessels. There are several modalities that are currently available, which include Doppler and color duplex ultrasound, CTA, and MRA ( Table 3.2 ). One study shows that paramedian incisions invoked the most damage to the vascular supply, negatively impacting the perforators, superficial inferior epigastric artery (SIEA), and deep inferior epigastric artery (DIEA). On the contrary, laparoscopic incisions invoked the least damage ( Table 3.3 ).
| Test | XR | Contrast | Caliber | Location | Flow | Course | Accuracy |
|---|---|---|---|---|---|---|---|
| Doppler | No | No | No | Yes | No | No | Low |
| Color duplex | No | No | No | Yes | Yes | No | Moderate |
| CTA | Yes | Yes | Yes | Yes | No | Yes | High |
| MRA | No | Yes | Yes | Yes | No | Yes | High |
| Scar | N | SIEA Disruption | DIEA Disruption | Perforator Disruption |
|---|---|---|---|---|
| Laparoscopy | 20 | None | None | None |
| Open appendectomy | 20 | All (ipsilateral) | None (ipsilateral) | Medial row of DIEA |
| Pfannenstiel | 35 | Medial branch (30/35) | None | NR |
| Paramedian | 3 | All (ipsilateral) | All (ipsilateral) | All (ipsilateral) |
| Open choly | 1 | None | None | None |
| Midline | 17 | None | None | Crossover |
Surgical Technique
Selection of Perforator for DIEP Dissection
When considering the DIEP flap, many surgeons will assess of the vascular anatomy using the methods described above ( Fig. 3.2 ). Intraoperative assessment is equally effective in identifying the abdominal wall perforating vessels. Reliance solely on intraoperative assessment requires more experience because of the variability associated with perforator location, caliber, and number. There are 5 types of perforators that are typically encountered. These perforators are direct (no muscle perforation, e.g. SIEA) and indirect (muscle perforation). In general, for a perforator flap to be successfully harvested and transferred, a single perforating artery and vein of at least 1.5 mm in diameter with a palpable pulse is recommended, although not absolute. If a dominant perforator arising from the deep system is not identified, one can consider performing an SIEA flap or a muscle-sparing free TRAM that incorporates several arterial and venous perforators.
Operative Technique – DIEP Flap Harvest
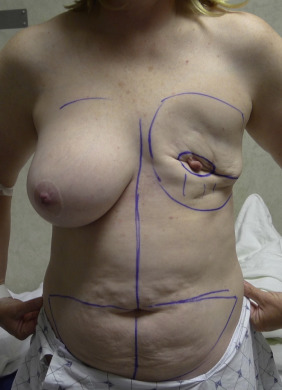
The preoperative markings are made with the patient standing and include the anterior superior iliac spine as well as the upper and lower transverse proposed incisions ( Fig. 3.3 ). In the operating room, patients are placed in the supine position under general anesthesia with the arms abducted to 75 degrees. A Foley catheter is inserted, pneumatic compression devices are applied to both lower extremities and the appropriate medications are administered (antibiotics, chemoprophylaxis). The upper abdominal incision is created first and the suprafascial adipocutaneous layer is elevated towards the xiphoid process. The patient is flexed at the waist approximately 30 degrees to determine the level of the inferior abdominal incision. The umbilicus is incised at its periphery and dissected along its stalk to the anterior rectus sheath. In the case of a bilateral reconstruction, the midline is divided along the linea alba.
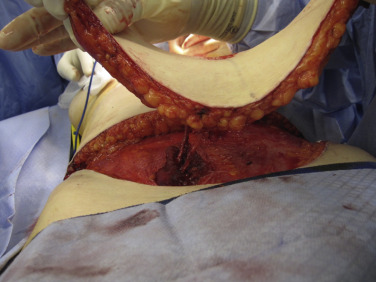
Following the initial incisions, the right and left hemi-abdomen is elevated from a lateral to medial direction. The selected perforator should ideally be located near the center of the flap in order to obtain equidistant perfusion ( Fig. 3.4 ). Perforator diameter should be 1.5 mm or greater and have a palpable pulse. When several perforators are available, sequential occlusion can be performed to assist with the selection process ( Fig. 3.5 ). If preoperative angiography was performed, the dissection can proceed immediately to the predetermined dominant perforator. Multiple perforators can be considered when they are aligned in series or in close proximity ( Fig. 3.6 ). Medial row perforators are preferred when the flap will include zone III or zone IV. Lateral row perforators can be considered; however, dissection of these perforators can be associated with an increased incidence of motor nerve injury due to proximity. When initiating the perforator dissection, including a small cuff of the anterior rectus sheath (1–2 mm) around the perforator is sometimes recommended, especially if the perforator is piercing the anterior rectus sheath at a tendinous inscription. During the dissection it is important to preserve the lateral intercostal nerves as they pierce the rectus abdominis muscle at the junction of the lateral and central longitudinal segments to avoid denervation injury ( Fig. 3.7 ). Intramuscular motor nerve branches that cross the perforator or the source vessel can be sharply divided ( Fig. 3.8 ). Whether or not to coapt the severed nerve is controversial. Some advocate using a micro-suture for coaptation; however, others prefer not to coapt but rather allow the transected nerve to neurotize into the adjacent muscle.
Related posts:
 Free Transverse Upper Gracilis Flap Breast Reconstruction
Free Transverse Upper Gracilis Flap Breast Reconstruction
 Immediate Implant Breast Reconstruction – One-Stage
Immediate Implant Breast Reconstruction – One-Stage
 Partial Breast Reconstruction With Local Tissue Rearrangements
Partial Breast Reconstruction With Local Tissue Rearrangements
 Immediate Prepectoral Implant Breast Reconstruction
Immediate Prepectoral Implant Breast Reconstruction
 Fat Grafting for Total Breast Reconstruction
Fat Grafting for Total Breast Reconstruction
 Partial Breast Reconstruction With Flaps
Partial Breast Reconstruction With Flaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


