Introduction
“Many handis make light warke ” John Heywood (1497–1580)
Hand surgery is always teamwork between the surgeon, the patient, and the therapist. One cannot get a successful outcome without the cooperation of the other two.
Interestingly there are exceedingly few randomized controlled trials in the management of hand fractures despite this being a common injury. Hand fractures are often considered to be a soft tissue injury with an underlying bone injury.
This chapter deals with the diagnosis and management of fractures of the phalanges and metacarpal bones in adults and children. The majority of these digit injuries can be treated effectively with conservative management and early therapy intervention. This chapter identifies the injuries that may need surgical intervention and the options available.
Pediatric Fractures of the Digits
Assessment, Classification, Management, and Complications
The differences between pediatric and adult hand fractures lie in the elasticity of children’s bones and the potential disruption of their growth.
Children’s bones have increased water content and plasticity, and tend to fracture incompletely with trauma. Incomplete fractures are seen as bows (bending forces), buckle fractures (one cortex buckles with compression), or green-stick fractures (one cortex ruptures under tension, the other is intact or buckles). The plastic deformation may prevent complete reduction of the fracture when manipulated, but most fractures still do not require open operations, but can be managed with closed or percutaneous techniques, due to the remodeling potential.
The assessment of the fracture is clinical and radiological. The child will have point tenderness in the nondisplaced fracture over the physis, which should increase suspicion of a fracture. If plain X-rays in two, if not three planes, cannot explain pain or deformation, MRI or CT will. The tenodesis test adequately demonstrates any rotational deformity, as the fingers should all be pointing towards the scaphoid tubercle. If in doubt, compare with the other hand. Angular deformities in children may remodel, rotational will not and needs to be corrected.
Any fracture interfering with the growth-plate has a potential for disrupting normal growth. Pediatric fractures involving growth plates are classified according to Salter and Harris. Ogden expanded the classification in 1984 ( Table 56.1 ). ,
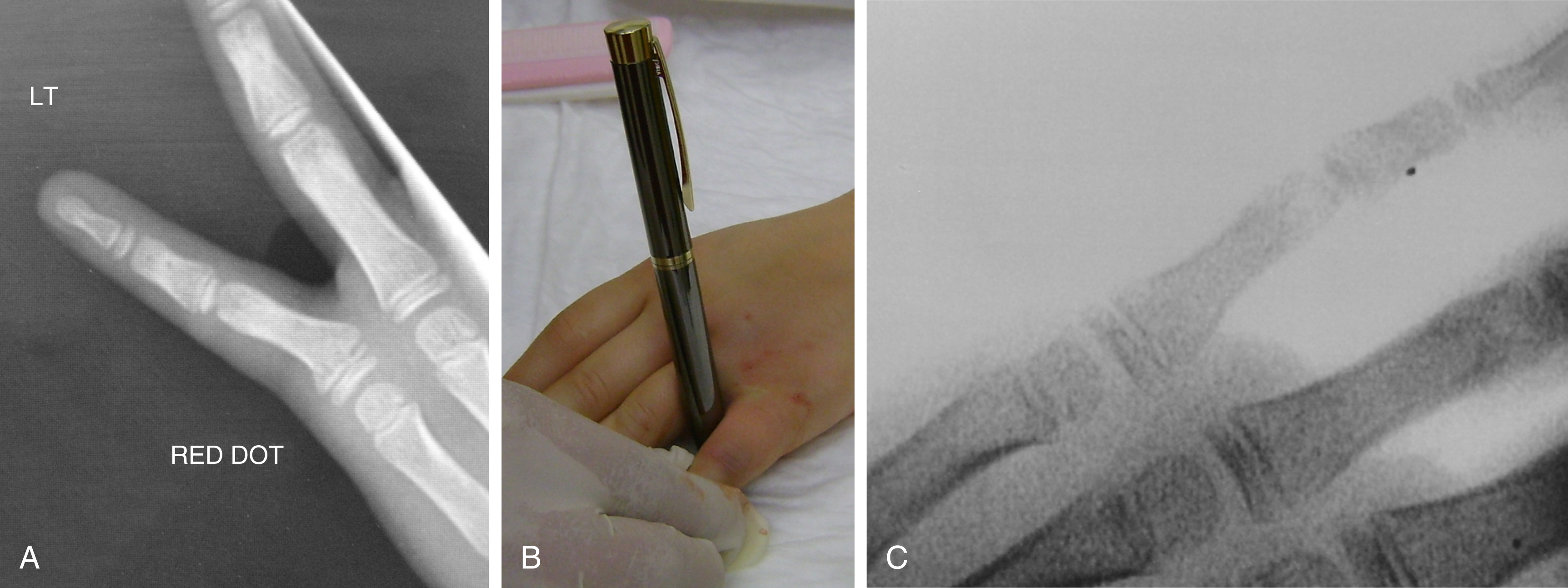
The most common fracture pattern encountered in the fingers is a Salter–Harris II, which is satisfyingly corrected with a simple maneuver with a pen, over which the finger is manipulated ( Fig. 56.1 ).
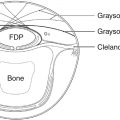
Crush distal phalanx fractures and nailbed injuries are the most common pediatric fracture. These occasionally need a Kirschner-wire (K-wire) or an orange needle to pin a larger distal fragment in place, but often the fragment is too small. A special type of nailbed injury is the Seymour fractures, which are displaced distal phalanx Salter I or II fractures, with avulsion of the proximal edge of the nail from the eponychial fold and the germinal matrix often interposed in the fracture itself ( Fig. 56.2 ). Accurate and timely debridement and repositioning of all tissues is therefore paramount to allow adequate growth of both digit and nail. The clinical presentation can be confused with a mallet finger (because the extensor tendon inserts itself in the epiphysis whilst the flexor tendon inserts itself in the metaphysis), but a true lateral X-ray and a thorough examination under anesthetic should reveal the injury.

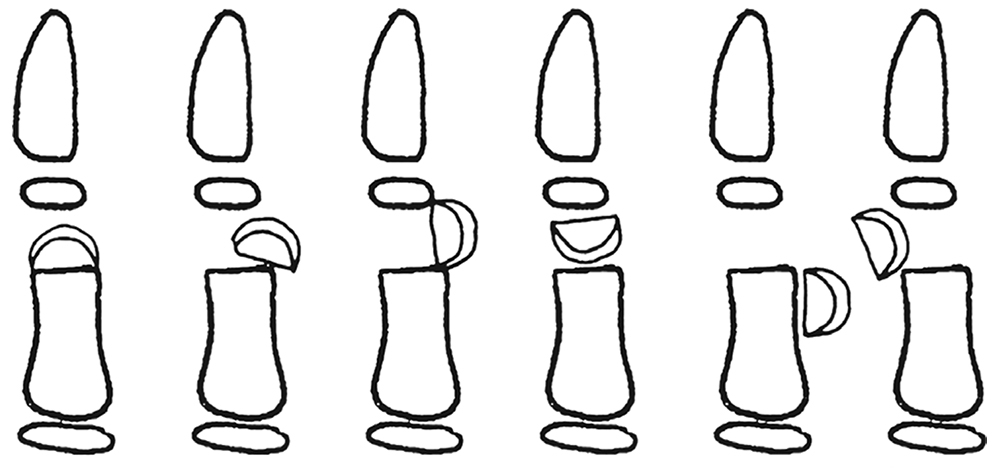
Fractures through the neck of the phalanges are usually only found in children and mostly involve some unfortunate interface between fingers and doors. Al-Qattan divided them into three categories, which determined prognosis and treatment: type I fractures are undisplaced, type II fractures are displaced, but maintain some bone-to-bone contact, whilst type III fractures have no bone-to-bone contact. Type III is furthermore subdivided according to the location of the distal fragment, type IIID especially being associated with an avascular fingertip ( Fig. 56.3 ). Since the smallest displacement is poorly tolerated, all types apart from type I require open reduction and K-wiring, but have progressively worse prognoses.
Hand therapy intervention for these patients is minimum as younger children rarely become stiff at the DIP joint and instinctively start functional use once the bulky bandage or splint has been removed. Older children may require a volar splint of the affected digit until pain has settled alongside edema control work.
It is worth remembering that there is no gain in changing the dressings in nailbed injuries before 10 days, unless you are worried about infections, which of course is a different matter.
Adult Fractures
Hand fractures account for ∼17% of all fractures in adults, with 59% of hand fractures occurring in the phalanges, 33% in the metacarpals, and 8% in the carpal bones.
It is the authors’ practice always to speak to patients about bone grafts and obtain consent for this option before the operation, even though it is rarely needed.
Metacarpal Fractures
Metacarpal fractures can be divided into their anatomical location or configuration, but most commonly occur in the little or ring fingers and the thumb.
Neck
Neck fractures of the fourth and fifth metacarpal are usually treated conservatively and many surgeons now state they will never treat these surgically, whatever the angulation of the fracture is. They can be manipulated and the digit neighbor-strapped, accepting that the patient will lose the knuckle and may have some extensor lag. If there is rotation of the digit this should be corrected surgically.
Neck fractures where the head is completely off the metacarpal and involves the index or little fingers may be fixed with minicondylar plates. In other fingers, H-plates or T-plates (the two-hole fixation on each side of the fracture can be transverse remember) can be used or perhaps even better, intramedullary K-wiring.
Intraarticular
Intraarticular metacarpal head fractures are best seen on Brewerton’s views and can be fixed with countersunk screws, if the fragments are large enough. The fragment must be three times the size of the screw head to hold it. If this is not possible a primary joint replacement or a free joint from the second toe may be considered at a later date if function is compromised. Very rarely does this joint get considered for fusion in the fingers.
Shaft
Metacarpal shaft fractures can be divided according to their configuration into transverse, spiral, short and long oblique, butterfly fragments, and comminuted.
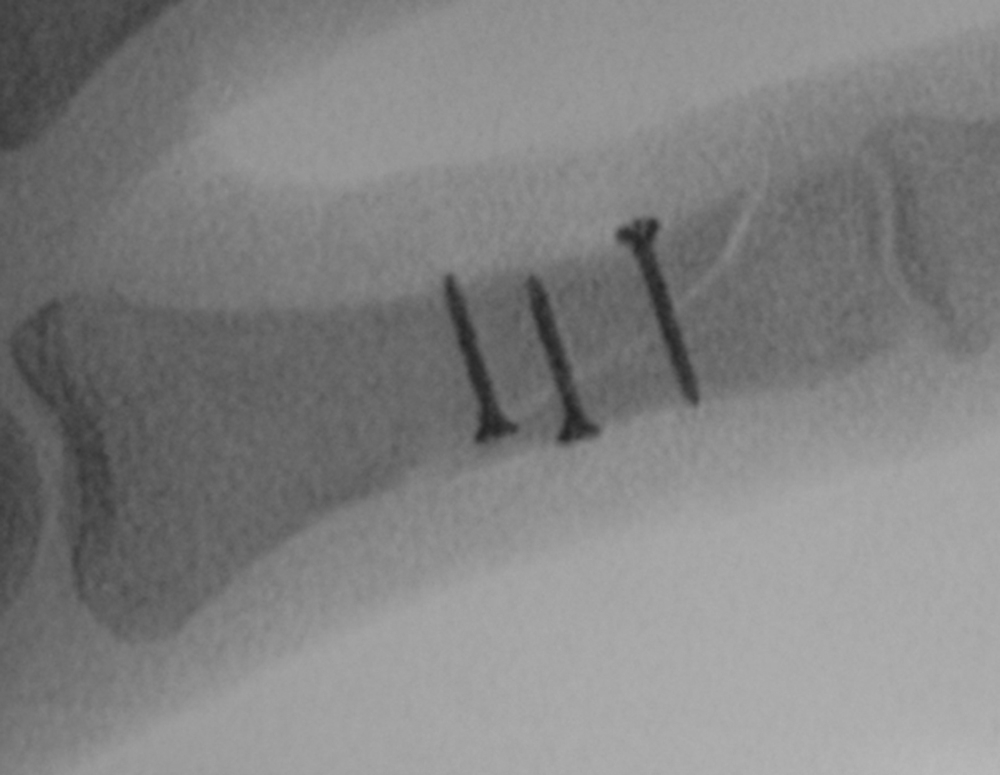
If the fracture can be held in position with one, or two bone-holding forceps, you can fix it with screws (which must be placed perpendicular to the fracture, not perpendicular to the bone) ( Fig. 56.4 ).
If you cannot maintain position with a bone-holding forceps, you must consider a fracture fixation which involves a plate (or even an external fixator for the first or fifth metacarpal). For a simple transverse fracture intramedullary K-wiring or an intramedullary screw is also a possibility. Be aware that crossed K-wires can distract the fragments rather than compressing the fracture. Moon et al compared intramedullary versus percutaneous K-wiring of distal third metacarpal fractures and found that the intramedullary group of patients returned to work 2 weeks earlier than the K-wire group, which was the only group to suffer any complications.
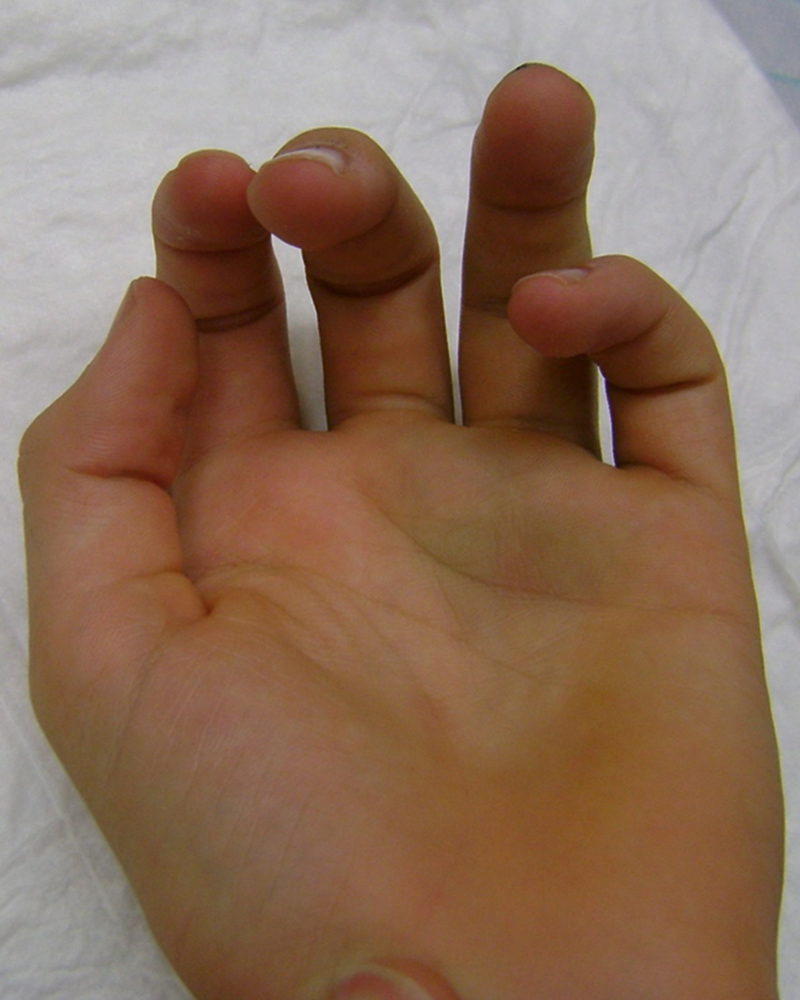
It is important to keep checking the position of the fingers, even when the fracture looks to be perfectly aligned when using plates, before drilling and inserting screws, to avoid rotation ( Fig. 56.5 ).
When applying plates to fractures it is important to understand the difference between locking and nonlocking plates. Conventional plates require precise adaptation of the plate to the aligned bone. The bone is pulled towards the plate when the screws are tightened and screw insertion can therefore alter the fracture position if everything is not precisely positioned. In locking plates the threaded screw head fits into the threaded plate hole and locks when tightened, thus providing a stable constellation of plate and screws. The bone is therefore not pulled towards the plate when the screws are tightened: the underlying cortical bone perfusion is not disrupted and the screws are unlikely to loosen from the plate, even if they have been inserted into a bone graft or fracture gap.
There are three plates to consider in metacarpal shaft fractures: a normal plate, a compression plate, and a bridging plate (= a locking plate). If the fracture is a simple short or long oblique, a normal plate can be used with or without a lag-screw, but must be bent appropriately to contour the bone. A compression plate is used for transverse fractures and must be slightly overbent to produce the compression of the fracture at the far cortex. A bridging plate is best viewed as an extramedullary splint, which “bridges” the part of the bone which is unsuitable for direct fixation, as in very comminuted or bone grafted fractures. With a dorsally placed locking plate, it is not necessary for the screws to reach the far cortex, so the fixation becomes unicortical and therefore quite quick as you do not have to measure the screw length.
Plates may be placed on the lateral cortex of the metacarpals, to avoid the adherence of the extensor mechanism, though this flies in the face of fracture fixation principles which are based on counteracting the forces exerted on the dorsal aspect of the fracture when the fist is clenched.
Intramedullary headless screw fixation of metacarpal fractures (and phalangeal fractures) is also possible and this method allows for very early mobilization, no periosteal stripping with dissection (and hence no potential subsequent tendon adhesion) or sticky-out metal work (K-wires), though it does violate the articular cartilage.
If unsure whether a fracture needs operative intervention, splint the fracture and re-X-ray after one week. If the position is not maintained, it needs to be surgically corrected, but remember to act on the X-ray no later than a week to 10 days post fracture.
Base
A reversed oblique view is a useful additional view to a true lateral and three-quarter radiograph in demonstrating injury at the base of the fourth and fifth metacarpals (in addition to the adjacent carpal bones and CMC joints). Have a low threshold for requesting a CT scan of these fracture, especially the fifth metacarpal base fractures. It is often difficulty to see whether there also is an associated impacted hamate fracture with this injury. It must be disimpacted by pulling the metacarpal out to length (ligaments will ensure that the hamate follows suit so to speak) and this reduction held in place, easiest with K-wires.
Metacarpal base fractures, which cannot maintain position, are almost always fixed with percutaneous K-wires, rarely plates, as there is not enough proximal bone for a plate.
In general, stable simple metacarpal fractures can be treated with buddy strapping, compression bandage and reduced function for 3–4 weeks until the fracture is pain-free and stable. Patients must limit their function otherwise they will develop large amounts of callus as the fracture heals.
Many patients experience swelling and pain. Resting in a custom-made Thermoplastic volar or dorsal splint in the position of safe immobilization if possible ( Fig. 56.6 ) can help ease this and allow the patient some light hand-function using the unaffected digits whilst fracture healing occurs.

Feehan and Bassett discuss how custom-made splints reduce complications compared with off-the-shelf splints or plaster of Paris. Hand-based splints are made for head and neck metacarpal fractures and longer splints for shaft and base fractures. Unfortunately, despite the high incidence of these fractures the research on rehabilitation is still limited. Most therapists would recommend early motion (3–5 days post operation) of the hand, especially if open surgical intervention has occurred. A Cochrane review by Poolman et al showed there was no research consensus of which splint was most effective to protect a fifth metacarpal neck fracture.
Feehan discusses how experienced hand therapists can mobilize the adjacent joints around a potentially unstable fracture, as an alternative to immobilization, in the first 3 weeks post fracture to achieve good long-term function. Early referral is essential.
Midgely and Toeman illustrated an example of an evidence-based patient pathway which is often used within trauma centers. For example, hand therapists use tendon gliding exercises within a splint that stabilizes the fracture. These techniques prevent stiffness and allow good tendon glide. Passive exercises will be introduced once healing has occurred normally, around 6 weeks, and patients will have movement controlled until this time.
After surgical repair scar management is essential, to avoid adhesions of the extensor mechanism. Depending on the nature of the fracture, an extensor lag at the MCP joint may be evident and the therapist can work with the patient to resolve this.
After basal fractures of the little and ring finger metacarpal bones some patients complain of discomfort when shaking hands. This is due to intermetacarpal stiffness and the inability to arch the hand and oppose the little finger to the thumb utilizing the hypothenar muscles. This motion must always be restored with targeted exercises.
Thumb Metacarpal Fractures
Two base-of-thumb fracture patterns must be mentioned separately: Bennett’s and Rolando’s.
A Bennett’s fracture is an intraarticular fracture dislocation of the thumb metacarpal base, which has a fragment, attached to the palmar beak ligament, and is usually fixed with K-wires (remember no need to spear the actual bony fragment!). Do remember that Bennet’s fractures can also be treated in a plaster or scotch cast, though long-term studies suggest the rate of pain seems higher in conservatively treated Bennet’s, but obviously complications only occur in the surgically treated group.
A Rolando’s fracture is also an intraarticular fracture of the base of the thumb metacarpal, but consists of three fragments, with a T or Y, configuration and is usually fixed with a T or Y plate, but can be K-wired.
Thumb metacarpal fractures, which are treated conservatively, are usually put in a forearm-based thumb splint/cast immobilizing the fracture for 3–4 weeks and protecting the thumb for 6 weeks. This splint must maintain the first web space so patients do not develop adduction contracture. All finger joints are mobilized fully.
Phalanges
Distal Phalanx
Distal phalanx fractures are classified into tuft, shaft or intraarticular fractures. They account for about half of all digital fractures seen.
Tuft fractures rarely need treatment themselves, but are often associated with nail-bed injuries, which must be treated as open fractures and the nail-bed matrix meticulously apposed.
Shaft fractures can usually be treated conservatively, but a longitudinal K-wire for a transverse fracture or the occasional cerclage wire or even screw may be necessary for the longitudinal fracture.
The treatment of intraarticular fractures depends on the size of the fragment and therefore the potential degree of subluxation. Small fragments must be treated conservatively in a mallet splint immobilizing the joint for at least 6 weeks. The concern has always been that larger dorsal fragments will become unstable due to the pull of the attached collateral ligaments. The decisive size of the fragment used to be quoted as one-third of the distal phalanx joint surface, but more recently studies have established that even fragments up to 50% of the articular surface did not necessarily subluxate. , Effective splintage is required for a good prognosis. The degree of subluxation can be assessed by lateral extension radiograph, though it remains unclear what level of subluxation requires treatment.
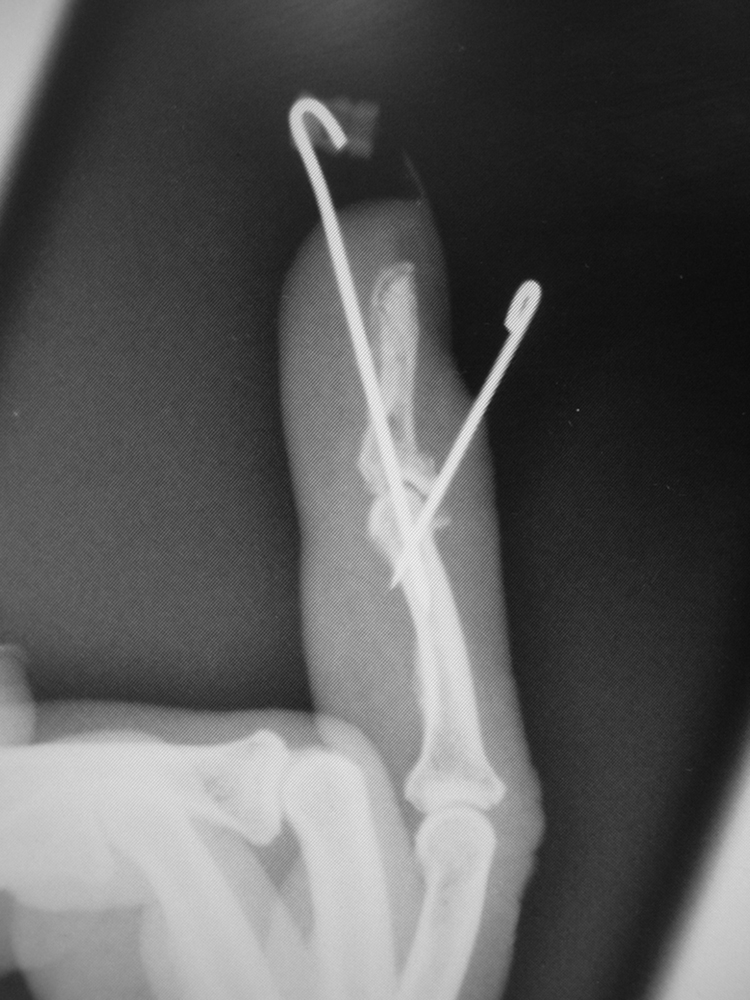
In volar fractures the flexor digitorum profundus (FDP) pulls the attached fragment away from the distal phalanx and will need surgical reattachment and a flexor tendon rehabilitation regimen. In dorsal fractures the fragment is held in place by the extensor tendon, whilst the FDP pulls the distal phalanx volarly, the latter resulting in a bony mallet or a mallet fracture. If surgery is required and the fragment is dorsal, Ishiguro’s method of fixation is a good solution. The dorsal wire supports the dorsal fragment and is placed first with the DIP joint in flexion; the fracture dislocation is then reduced and the longitudinal wire is placed under image-intensifier (II) guidance ( Fig. 56.7 ). In volar fractures the fragment, if large enough, can be secured with a screw. If, however it is too small to withstand instrumentation, then the FDP can be fixed to the distal phalanx by bony anchors, pull-out sutures, or by sutures passed through the distal phalanx transversely, using a white needle drilled through the bone. The DIPJ will become somewhat stiff whatever you do.