![]()
Introduction
Oculofacial surgery is a unique specialty that combines aspects of ophthalmology, general plastic surgery, head and neck surgery, dermatology, neurological surgery, and craniofacial surgery. With advances in endoscopic and small incision techniques, many oculofacial procedures can now be performed safely and effectively with minimal scarring and excellent aesthetic results.
Evaluation
Oculofacial surgery encompasses both functional and aesthetic goals. As such, the evaluation of the oculofacial patient requires a complete history and physical examination with particular attention to medical, functional, aesthetic, and psychosocial details.
A complete medical history should be elicited, with particular attention to hypertension, diabetes, liver disease, immune status, current or prior cancer, and trauma. Surgical history should include any previous facial surgery, ophthalmic surgery (such as refractive surgery), use of neurotoxins and dermal fillers, and chemical- or energy-based skin treatments. Medications, including anticoagulants, tobacco, and alcohol, should be documented. A history of implanted cardiac devices should also be noted since this determines which types of cautery can be safely used. The use of medications, tobacco and alcohol should be documented.
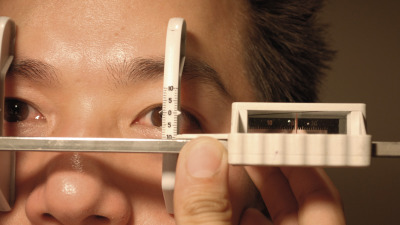
The physical examination should focus on the areas of patient concern and the proposed surgical procedure. The entire face should be examined and the patient can be allowed to point to areas of concern using a handheld mirror. For most eyelid, facial, and orbital procedures, documentation of visual acuity, pupillary function, color vision, slit-lamp examination, intraocular pressure, eyelid position and closure, and tear film are minimum requirements. Dilated fundoscopic examination may be required in select cases if there is any evidence of optic nerve compromise. Ocular motility in nine positions of gaze ( Figure 1.1 ) and globe position by exophthalmometry ( Figure 1.2 ) should be carefully documented for any orbital procedure. The Naugle exophthalmometer is useful for measuring proptosis or enophthalmos when prior surgery has been performed to remove the lateral orbital rim. Vertical and horizontal globe displacement should be noted as well. Evaluation of lacrimal diseases requires functional and anatomic testing. Both dye disappearance testing and lacrimal probing and irrigation are useful.

Ancillary testing for oculofacial surgery may include visual field testing for functional eyelid conditions, dacryoscintigraphy for lacrimal obstructions, and imaging studies for orbital diseases. Computed tomography (CT) is useful for evaluation of bony structures and general screening for orbital disease. Magnetic resonance imaging (MRI) is better suited for soft-tissue lesions and optic nerve diseases. Angiography is indispensable for evaluating vascular malformations.
Photography is an essential component of the oculofacial examination. Ideally, photographs should be taken during all aspects of patient care from the preoperative evaluation, intraoperatively when indicated, and at postoperative visits. Many third-party insurance carriers require photographic documentation prior to authorization of functional oculofacial surgeries. Additionally, photographs are important for the aesthetic patient to document changes after treatment and for medical legal protection. Photographs should be taken in the frontal, side, and three-quarter views. For orbital diseases, eye movements in the nine positions of gaze are taken. Additionally, a worm’s eye view ( Figure 1.3 ) is used to document globe position and closure of the lids to document the presence or absence of lagophthalmos ( Figure 1.4 ).


Modern digital single lens reflex (DSLR) cameras are ideal in the oculofacial setting. These DSLRs allow for rapid sequence photography with excellent resolution and dynamic range compared to pocket-sized cameras with smaller imaging sensors. Uniform lighting can be difficult and variable depending on the clinical situation. In general, flash photography is used to normalize lighting. A dedicated photo room with a blue backdrop and diffuse lighting is ideal, but for most surgeons, a DSLR using the pop-up or external flash will suffice. The use of a 50 mm macro lens is ideally suited for full-time use. Using the macro function, this lens allows close-up photography of small lesions on the face. Furthermore, with its fixed focal length, facial photographs will appear square and consistent, avoiding the barrel distortion seen when the camera is too close to the subject. Finally, to achieve uniform focus across the entire photograph, a small aperture (at least greater than f/10) should be set to allow for a deep depth of field.
Anesthesia
The choice of anesthesia depends on patient age, medical condition, as well as physician and patient preference. Patient safety and comfort are an absolute priority, and intraoperative patient cooperation may be needed during certain oculofacial procedures. A combination of various anesthetic modalities is frequently utilized to provide an optimal surgical experience.
Topical anesthesia
Topical anesthetic drops such as proparacaine or tetracaine are useful for conjunctival procedures and also to prevent ocular discomfort from prep solutions (e.g., Betadine solution). Topical anesthetic gels, such as lidocaine gel, with concentrations ranging from 1% to 4%, can be used in more involved procedures because of their longer-lasting effect. Also, topical anesthetic creams can be applied to the skin before injection procedures or minor cutaneous biopsies.
Local infiltration
In most oculofacial procedures, local infiltration of involved tissues is the preferred method of anesthesia. It entails minimal risks while allowing adequate patient comfort and cooperation. Local anesthetic agents include short-acting lidocaine and procaine, or long-acting bupivacaine. A mixture of short-acting and long-acting anesthetic agents is often used to have a rapid onset and long duration of action. The mixture of equal parts of 2% lidocaine with epinephrine at 1 : 100,000 and 0.75% bupivacaine is an effective combination. The vasoconstrictive effect of epinephrine improves hemostasis, reduces vascular absorption, and increases duration of action of the anesthetic. Other potential additions include hyaluronidase, which facilitates anesthetic dispersion through tissues, and bicarbonate, which buffers the pH, reducing the stinging sensation during infiltration. The surgeon should be vigilant for possible cardiac or neurologic side effects, particularly with inadvertent intravascular injections. By withdrawing the plunger and ensuring that there is no reflux of blood prior to injecting, the risk of intravascular injection can be further reduced. Local anesthetic should be injected sparingly during external levator advancement and eyelid retraction repairs, since infiltrating the levator with anesthetic can cause artificially reduced levator function. Other risks include tissue necrosis, although this is unlikely due to the abundant vascularity of the periorbital area.
When local anesthesia is administered in a clinic setting without oral or IV sedation, several maneuvers can be performed to minimize discomfort. Performing massage or vibratory distraction at or near the site of injection may decrease pain perception according to the gate control theory. Dilution of lidocaine/bupivacaine with sodium bicarbonate (in a 1 : 10 ratio) raises the pH to minimize injection site burning. Pre-cooling the target area with ice packs is another adjunct, as is use of topical lidocaine cream for the skin or 4% lidocaine on cotton tip applicators for mucous membranes. Finally, slow injection, handholding and talking “talkesthesia” are all useful in fully conscious patients. Minimizing pain during injection will go a long way towards maintaining the confidence of your patients and ensuring subsequent cooperation during the procedure.
Regional block
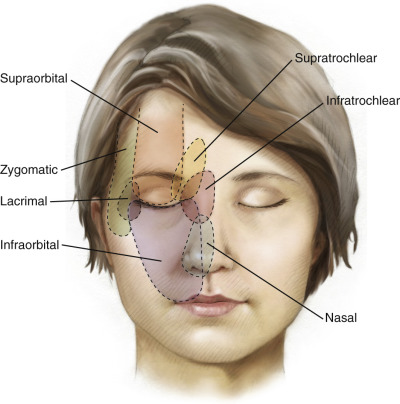
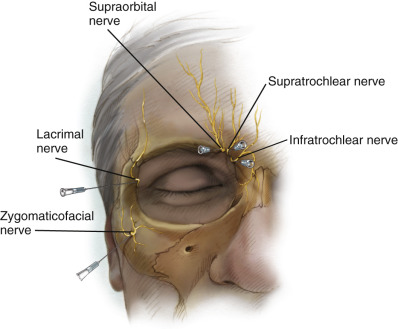
Regional blocks can be useful in oculofacial procedures but are rarely used as a standalone means of anesthesia due to redundant innervation in the facial region ( Figure 1.5 ). It allows the surgeon to minimize the volume of local infiltration needed, anesthetize broad regions of the face, and minimize tissue distortion from local infiltration. Regional blocks of the face must address one or more branches of the ophthalmic, maxillary, and mandibular divisions of the trigeminal nerve.
Lacrimal nerve
The lacrimal nerve branches off the ophthalmic division of the trigeminal nerve and supplies the lateral upper eyelid and lacrimal gland. It can be blocked by injecting the needle along the superolateral orbital rim behind the lacrimal gland. Potential risks include injury or injection into the lacrimal artery. This block is useful when performing lacrimal gland biopsies or resuspension procedures ( Chapter 70 ).
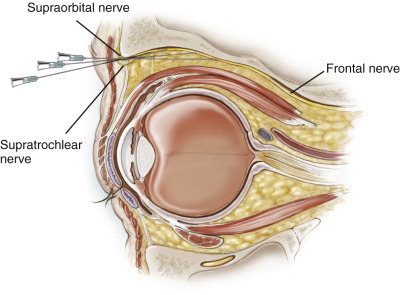
Frontal nerve
The frontal nerve is a branch of the ophthalmic division of the trigeminal nerve. It further divides into the supraorbital and supratrochlear nerves and supplies the medial and central upper eyelids and the forehead. It can be fully blocked by injecting anesthetic deep in the orbit along the central orbital roof. Alternatively, the supraorbital nerve can be selectively blocked by injecting near its exit from the orbit, at the supraorbital notch or foramen, around the medial third of the superior orbital rim. A supraorbital block anesthetizes the central eyelid, eyebrow, and forehead. Similarly, the supratrochlear nerve can be blocked by injecting anesthetic near the trochlea at the junction of the medial and superior orbital rim. A supratrochlear block anesthetizes the medial eyelid and eyebrow. Prior to injecting, the surgeon should withdraw the plunger on the syringe to ensure that inadvertent intravascular injection into the supraorbital or supratrochlear arteries does not occur. This block can be used for any upper eyelid procedure and is well suited for limited upper eyelid protractor myectomy ( Chapter 33 ).
Nasociliary nerve
The nasociliary nerve is the third branch of the ophthalmic division of the trigeminal nerve. It supplies the nasal mucosa and skin through the anterior and posterior ethmoidal nerves, as well as the medial canthus and lacrimal sac via the infratrochlear nerve. An infratrochlear block is achieved by injecting deeply under the trochlea above the level of the medial canthal tendon. A deeper injection at the same location would block the ethmoidal nerves, but possible injury to the corresponding ethmoidal arteries can cause orbital hemorrhage. Ethmoidal nerve blocks can be performed prior to dacryocystorhinostomy or medial-wall decompression ( Chapter 53 , Chapter 54 , Chapter 55 , Chapter 56 , Chapter 57 , Chapter 58 , Chapter 59 , Chapter 64 ).
Infraorbital nerve
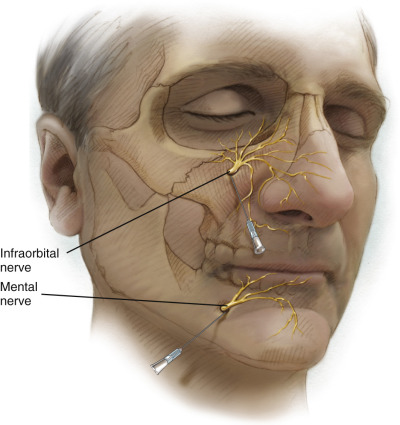
The infraorbital nerve branches off the maxillary division of the trigeminal nerve and supplies the lower eyelid skin and conjunctiva, in addition to the medial canthus, lacrimal sac, mid-face, and maxilla. It can be blocked where it exits the infraorbital foramen around 7–10 mm inferior to the infraorbital rim. Either the transconjunctival or sublabial routes can be used for administration. The foramen can be palpated where it intersects a line drawn from the nasal ala to the lateral canthal angle. Alternatively, deeper orbital injection along the orbital floor can block the nerve more proximally. This block is useful for nasolacrimal intubation in the clinic setting ( Chapter 60 ).
Zygomaticofacial nerve
The zygomaticofacial nerve is another branch of the maxillary division of the trigeminal nerve; it supplies the lateral canthus and lateral lower eyelid. It can be blocked where it exits the zygomatic bone through a foramen around 10 mm inferior to the lateral canthus. This block is useful for adjunctive anesthesia during a zygomaticomaxillary complex fracture repair.
Mental nerve block
The mental nerve is a branch of the mandibular nerve. Blocking this nerve can be useful in administering fillers in the lower lip and chin region. This block can be given through the lower gingival sulcus just as the mental nerve exits its foramen.
Oral sedation
Oral sedation in conjunction with local anesthetic administration is preferred for most in-office procedures. Oral benzodiazepines such as diazepam are given at least 30–60 minutes prior to the procedure. Clonidine can be used for both its anxiolytic and anti-hypertensive properties. Oversedation is the most common risk, especially with benzodiazepines, in which case flumazenil (a benzodiazepine antagonist) can be administered.
Monitored anesthesia care
Monitored anesthesia care combined with local or regional block is preferred in more complex procedures. It is popular because of its ability to provide sedation, amnesia, and anxiolysis. Intravenous propofol may be given as a bolus at the time of local anesthetic injection, followed by a steady-state infusion supplemented with opioids (fentanyl) or benzodiazepines. Possible side effects include apnea, myocardial depression, and decreased vascular resistance. For this reason, close monitoring of vital signs, ECGs, and pulse oximetry is necessary.
General anesthesia
General anesthesia is reserved for more prolonged and stimulating procedures, when nasal bleeding is expected, or in children and other patients who may have difficulty following instructions. Local anesthesia with epinephrine is typically administered as an adjunct for hemostasis and postoperative pain. Risks involved include laryngospasm, malignant hyperthermia, myocardial infarction, and even death. A careful family history looking for unexplained anesthesia death or malignant hyperthermia should be obtained, since these life-threatening conditions are more commonly associated with musculoskeletal ocular conditions. All cases of surgery under general anesthesia should employ the use of sequential compression devices (SCDs) to minimize risk of deep venous thrombosis ( Figure 1.6 ).

Tumescent anesthesia
Tumescent anesthesia is a technique that provides effective pain control and hemostasis for larger regions of the face and body. It can be effectively used in liposuction/lipotransfer, face and neck lifting, and endoscopic or pretrichial brow lifting ( Chapter 22 , Chapter 23 , Chapter 24 , Chapter 47 ). Care should be taken to ensure the meticulous dilution and labeling of tumescent anesthetic solutions and to consider the total amount of anesthetic delivered in order to prevent anesthetic or epinephrine toxicity.
Hemostasis
Hemostasis in oculofacial surgery is of vital importance, since an orbital hemorrhage can cause compartment syndrome and possible blindness. Even for non-orbital surgeries, postoperative bleeds or hematomas can result in blood loss and patient anxiety, compromise of flaps or grafts, inflammation, and increased postoperative healing time. Prolonged epistaxis after lacrimal surgery can result in significant postoperative morbidity and discomfort.
Anticoagulants
Prior to surgery, patients on anticoagulants should be advised to discuss with their internist, cardiologist, or other prescribing physician the possibility of stopping them in the perioperative period. A decision must be made balancing the risks of intra- and postoperative bleeding versus the risk of potentially life-threatening thromboembolic events. Where appropriate, coagulation studies should be ordered preoperatively.
Aspirin and other non-steroidal anti-inflammatory drugs (NSAIDs) inhibit platelet function and ideally should be stopped at least 1–2 weeks prior to surgery. Clopidogrel (Plavix) should also be stopped at least 1 week prior to surgery.
Warfarin (Coumadin) should be stopped at least 5 days prior to surgery to allow the INR to normalize. It can be restarted the next day after surgery, given the lag time before the INR becomes therapeutic again. If anticoagulation is necessary within this time frame, patients can be bridged on IV unfractionated heparin or low-molecular-weight heparin injections, which are typically discontinued 4–5 hours (half-life of 45 minutes) and 24 hours (half-life 3–5 hours) prior to surgery, respectively. Of particular note, newer direct thrombin inhibitors (e.g., dabigatran) and factor Xa inhibitors (e.g., rivaroxaban, apixaban, edoxaban) are being utilized, which have shorter half-lives, which mean they can be discontinued and resumed rapidly. However, these agents lack a reversal strategy and cannot be tested for activity with PT/INR testing.
Finally, some over-the-counter vitamins and supplements can have anticoagulant effects and consideration should be given to discontinuing these prior to surgery. These include Ginkgo biloba , ginseng, ginger, garlic, fish oil, and vitamin E which are often overlooked by patients and surgeons as a source of significant anticoagulant activity.
Coagulation devices
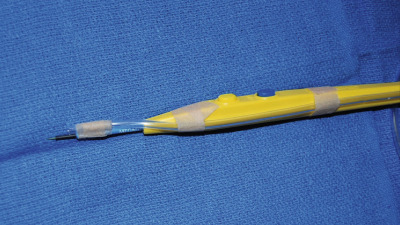
Thermal coagulation with a battery-powered high- or low-temperature cautery is one modality of coagulation that can be performed using a disposable handheld probe. This cost-effective and portable means of cautery can be used for dissection or coagulation but it is typically less effective in stopping brisk bleeding compared to electrocautery. The use of handheld thermal cautery may also cause less pain and startle movement compared to electrocautery. The use of handheld thermal cautery for clinic-based procedures is ideal because no bulky electrocautery unit or grounding pads are required.
Electrocautery can be performed using monopolar, bipolar, or wetfield cautery units. Bipolar cautery conducts current between the two prongs of the forceps and provides the most effective coagulation while minimizing thermal injury to surrounding tissues. Monopolar cautery can alternately cut and coagulate tissue but requires the use of a grounding pad and should be avoided in patients who have pacemakers and automatic implantable cardioverter defibrillators (AICDs), since transmitted currents can result in pace inhibition, damage to the pulse generator, or inappropriate antitachycardiac therapy. A smoke evacuator can be fashioned with monopolar cautery using standard IV tubing and connecting this to standard wall or portable suction ( Figure 1.7 ). Another device that can simultaneously cut and coagulate tissue is the carbon dioxide laser. Use of the CO 2 laser requires training, protective eyewear for OR staff and full-time use of metal corneal shields to prevent corneal damage. Care should also be taken to use the appropriate laser settings as excessive energy can lead to charred tissue edges and wound dehiscence postoperatively.
With all of these agents, it is important to communicate with the anesthesiologist to avoid excessive supplementary oxygen use and reduce the risk of fires. Even with lower oxygen use, surgical drapes covering the mouth and nose may result in oxygen pooling, increasing the incendiary risk.
Other hemostatic agents
The most frequently used vasoconstrictive agent in local anesthesia is epinephrine, which typically comes pre-mixed in a 1 : 100,000 concentration. This can be further diluted to 1 : 200,000 with similar vasoconstrictive properties and less cardiotoxity. Local anesthesia should be injected about 15 minutes prior to surgery for maximal effect. Topical 2.5% phenylephrine drops can similarly be applied to the ocular surface to minimize conjunctival bleeding.
Various other types of hemostatic agents can be used intraoperatively to assist with hemostasis. These include gelatin sponges (Gelfoam), absorbable hemostats (Surgicel, Avitene), hydrogen peroxide, topical thrombin, and fibrin sealant (Evicel). Direct pressure and the use of cold saline can also assist with hemostasis. For patients with platelet dysfunction or other bleeding diatheses, platelet transfusions and perioperative tranexamic acid can further help hemostasis. Tranexamic acid, an anti-fibrinolytic agent, must be used cautiously and with serial compression devices (SCD) to mitigate the risk of venous thromboses.
During lacrimal surgery, nasal mucosal bleeding can be reduced with preoperative oxymetazoline nasal sprays and nasal packing with 1 : 10,000 epinephrine-soaked cotton pledgets. Other strategies to reduce bleeding include permissive hypotension and placing the patient in reverse Trendelenburg position. Intranasal silver nitrate and suction cautery devices can assist with direct coagulation.
For bone bleeding, paraffin-based bone wax can be directly applied. In open, accessible areas, the bone wax can be directly applied by digital application while deeper in the orbit a small ball of wax can be applied on a cotton-tip applicator. In select cases, bone marrow space bleeding can be stopped using a high-speed diamond tip burr by thermal coagulation.
Postoperative bleeding prophylaxis
Postoperative bleeding occurs with greatest frequency within the first 48–72 hours after surgery but can occur as late as 1–2 weeks postoperatively as clot contraction occurs. Patients should be instructed to avoid heavy lifting, straining, and bending, which can result in a transient spike in blood pressure and subsequent bleeding.
Pressure patches, head wraps, and sutured foam bolsters can be used to apply direct pressure to the surgical site to help prevent postoperative bleeding and hematoma formation. Care should be taken to avoid pressure patching the eye after orbital surgery as this may mask symptoms of a retrobulbar hemorrhage. When large coronal and facial flaps are performed, drains such as a Jackson–Pratt drain can assist in evacuating early postoperative hemorrhage or serosanguineous drainage.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


