Introduction
The first forehead lift procedures were performed using an “open” technique in which long incisions on the scalp or along the frontal hairline were made, a forehead flap was turned inferiorly, and modifications were made to corrugator supercilii and other muscles under direct vision. These breakthrough procedures served several generations of patients well and, while still performed by many surgeons today, they have been rejected by many patients and abandoned by some surgeons who view them as too aggressive too time-consuming to perform, and/or too difficult to market.
As endoscopic techniques made inroads into esthetic surgery, one of the first procedures they were adapted to by plastic surgeons was the forehead lift. Although a decade or more of technical refinements had to pass before the “closed” forehead lift procedure finally came of age, it has since come to be widely accepted and continues to be a viable alternative to open procedures for many patients. Experience has since shown that a “closed” technique without an endoscope can be used to mobilize and release the forehead and modify the corrugator supercilii muscles if the anatomy is understood and the operation is appropriately planned. In addition, transpalpebral corrugator myectomy, when used in conjunction with closed mobilization and resuspension of the forehead, not only provides a scheme for the performance of closed foreheadplasty without the need for an endoscope, but a method by which medial brow elevation can be minimized or avoided. Unesthetic medial brow elevation as a result of releasing the central brow to access the corrugator supercili muscles has been the “Achilles heel” of the endoscopic procedure and at least part of the reason endoscopic forehead lifts have fallen in popularity, and may, indeed, be one of the nonendoscopic short-scar procedure’s most appealing and important merits.
Patient Options in Forehead Rejuvenation
Patients seeking improvement of their forehead appearance have four general categories of procedures available to them:
- 1.
Open procedures using a bicoronal incision
- 2.
Open “hairline-lowering” and “forehead-shortening”’ procedures using an incision or partial incision along the hairline
- 3.
Closed, “limited-incision” or “short-scar” endoscopic procedures
- 4.
Direct eyebrow lift using a supraciliary (upper edge of eyebrow) or forehead crease incision.
Selection of the “best” procedure depends on the patient’s specific characteristics, including quantity of hair, hairline position, the quality of tissues, the condition of the scalp, the amount of improvement sought, and the overall degree of the aging changes that are present.
Identifying the Patient in Need of a Forehead Lift
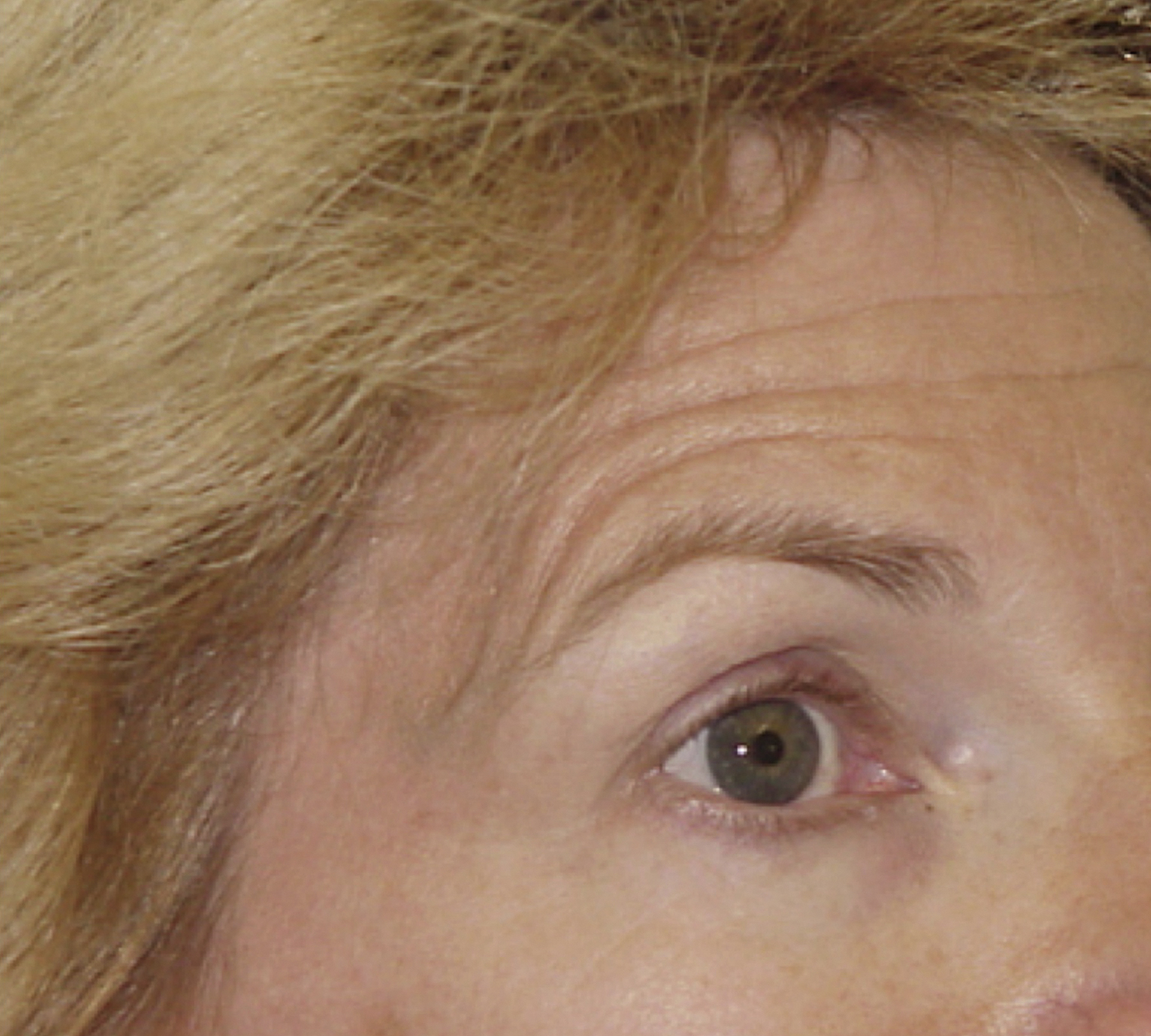
Recognizing the changes that occur in the aging upper face is fundamental to rejuvenation of the forehead, and a requirement to communicating the need for the procedure to the patient. More detail on facial aging is available in Chapter 62 . Typical changes seen in the aging forehead include eyebrow ptosis, lateral brow ptosis, pseudoblepharochalasis, glabellar “frown lines,” transverse forehead creases, corrugator muscle hypertrophy, transverse upper nasal creases, and hairline recession ( Fig. 63.1A ). Each of these problems can potentially be improved with a foreheadplasty ( Fig. 63.1B ).

The forehead, eyebrow, and the upper eyelid are functionally and esthetically linked and it is not possible to appropriately rejuvenate the upper eyelid without performing forehead surgery in many cases. The eyebrow is the key to an attractive and appealing upper orbital appearance. The assumption that forehead ptosis is not present because eyebrow position appears satisfactory is the most common error in evaluating and treating the upper orbit and forehead ptosis must be suspected in any patient who appears to have excess upper eyelid skin – even if eyebrow position appears normal. If forehead ptosis is not recognized and appropriately treated upper blepharoplasty will result in esthetic and functional problems.
Transverse forehead creases and chronic frontalis spasm are the hallmark of forehead ptosis ( Fig. 63.2 ). These are the result of the patient subconsciously trying to clear obstruction of their upper lateral fields of vision and to lift ptotic brow skin off their eyelids. Often these signs are not evident on initial examination, as patients learn to conceal them with their hairstyles. Chronic frontalis spasm gives the false impression that the eyebrow is in an appropriate position and this further diverts suspicion that forehead ptosis is present. Because the patient’s hairstyle can hide important signs of forehead aging, and that compensatory frontalis spasm can give the false impression that the eyebrows are in an appropriate position, it is imperative that the patient’s face be examined with their hair pushed well back off their forehead. In addition, because patients who wear forehead-concealing hairstyles often do not see the full extent of these problems, it is helpful, as it is during the rest of their evaluation, if they hold a hand mirror during this part of the examination. They can then be shown these important findings and counseled as to how they are the product of, and related to, forehead ptosis.

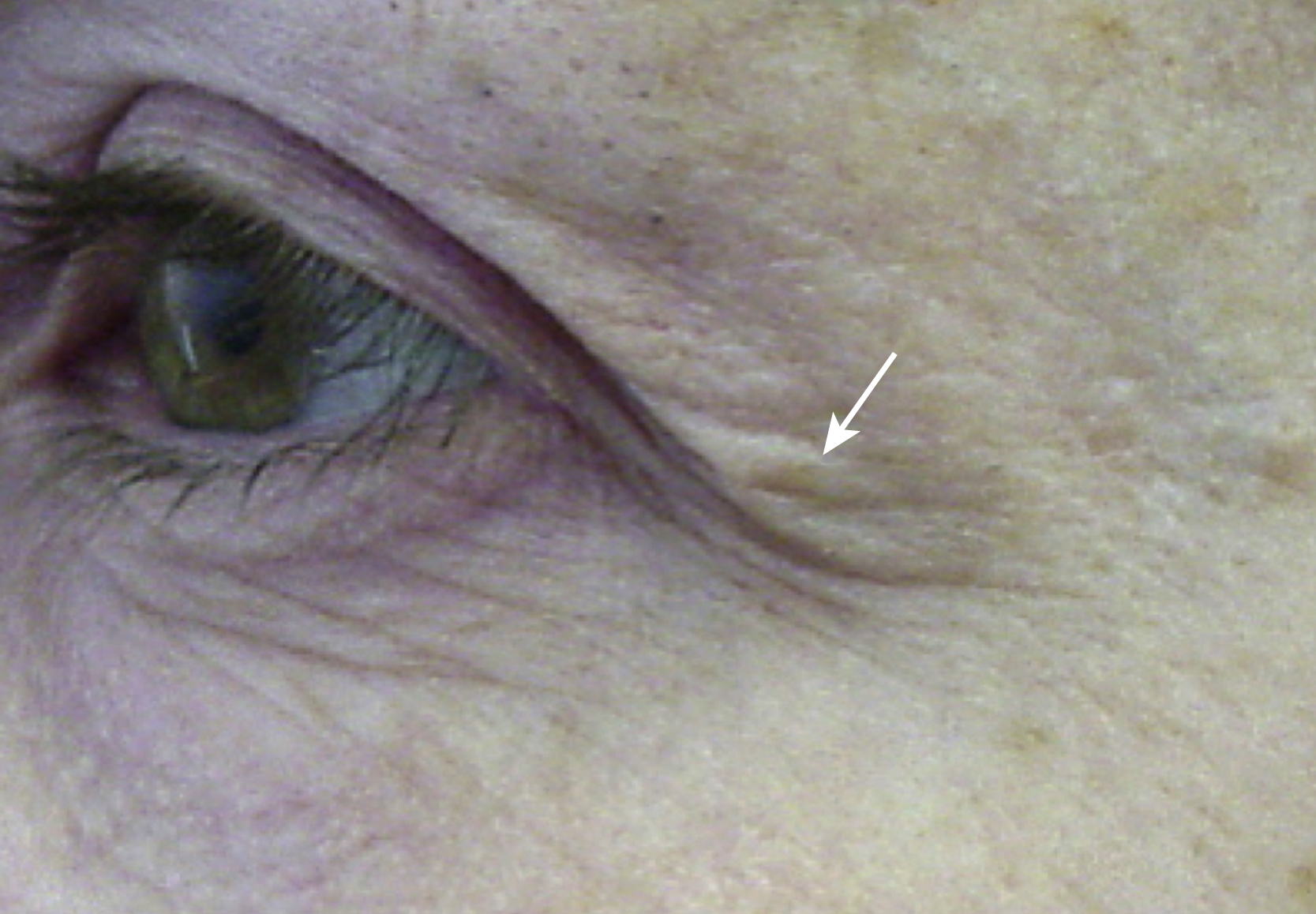
An upper lid skin fold that extends off the eyelid and onto the lateral periorbital area is a key sign of forehead ptosis and an important finding in differentiating forehead from eyelid problems (“Connell’s sign”) ( Fig. 63.3 ). In many cases this sign will be evident only after the patient’s forehead is relaxed and their brow descends to its “resting” position. For this reason it is important to examine the patient’s forehead in repose with the frontalis relaxed. Often this will take some coaxing, as patients with significant forehead ptosis commonly develop compensatory chronic frontalis spasm and unconsciously hold their eyebrows up in an elevated position. Lightly stroking the forehead until the frontalis relaxes well help uncover the full extent of these patients’ problems.
Frequently, patients seeking upper blepharoplasty will unknowingly signal the need for forehead surgery during their consultation by holding up their eyebrow with a fingertip while requesting eyelid surgery (“Flower’s sign”) ( Fig. 63.4 ). For patients who fail to provide this sign, the surgeon should reposition the patient’s brow and observe the effect produced while the patient watches holding a hand mirror. Often this simple maneuver will show that it is obvious that significant forehead ptosis is present and that little, if any, eyelid skin will need to be removed. In other cases it will be evident a combined problem is present and that both eyelid and forehead surgery is indicated. If eyebrow repositioning results in limited improvement of the upper eyelid and little improvement in the patient’s overall appearance, eyelid surgery alone may be appropriate.

The erroneous assumption that forehead ptosis is not present because the eyebrow appears to be in a normal position is the most common mistake in evaluating the forehead for patients and surgeons alike. Patients are accustomed to optimizing the appearance of their face when looking at their reflection by unconsciously raising their eyebrows ( Fig. 63.5 ). This is often further compounded by the fact that many women aggressive pluck the inferolateral portion of their eyebrow to give the illusion that it is higher and more arched. In many cases the entire outer half of the eyebrow is missing and has been drawn on in a higher position with an eyebrow pencil. The all too commonly observed circumstance is one in which the patient with marked frontalis spasm and marked transverse forehead wrinkling holds a hand mirror during their consultation and sees only that their eyebrows appear to be in a normal position. In these situations it is essential that the surgeon explain the dynamics at work ( Fig. 63.6 ).
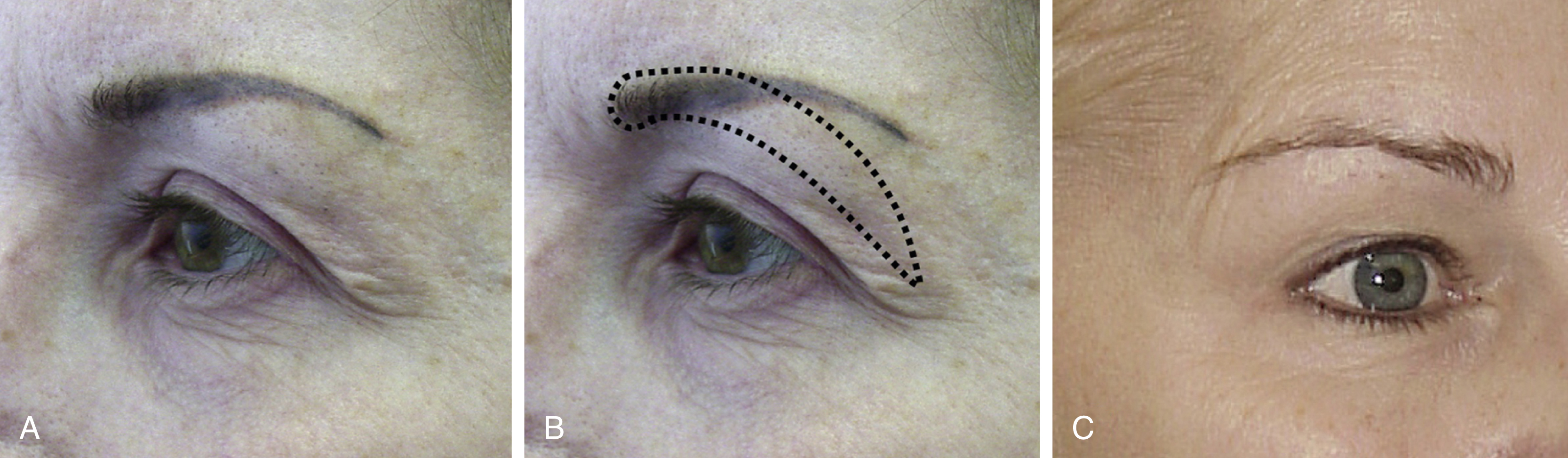
Many patients requesting upper blepharoplasty will have unrecognized forehead ptosis as a significant part of their “eyelid” problem, but compensatory frontalis spasm will make the eyebrow appear to be in a normal position. For these patients the goal of foreheadplasty will be to fix the eyebrow in the position the patient holds it preoperatively and to prevent the eyebrow from dropping when eyelid skin is removed. In many properly performed foreheadplasties, the eyebrow will be in the same position after surgery as it was before, compensatory frontalis spasm, however, will be eliminated, transverse forehead wrinkles will be reduced, and the eyebrow will not drop when upper eyelid skin is removed. These facts and the need for forehead surgery must be communicated to the patient if esthetically appropriate outcomes are to be obtained.
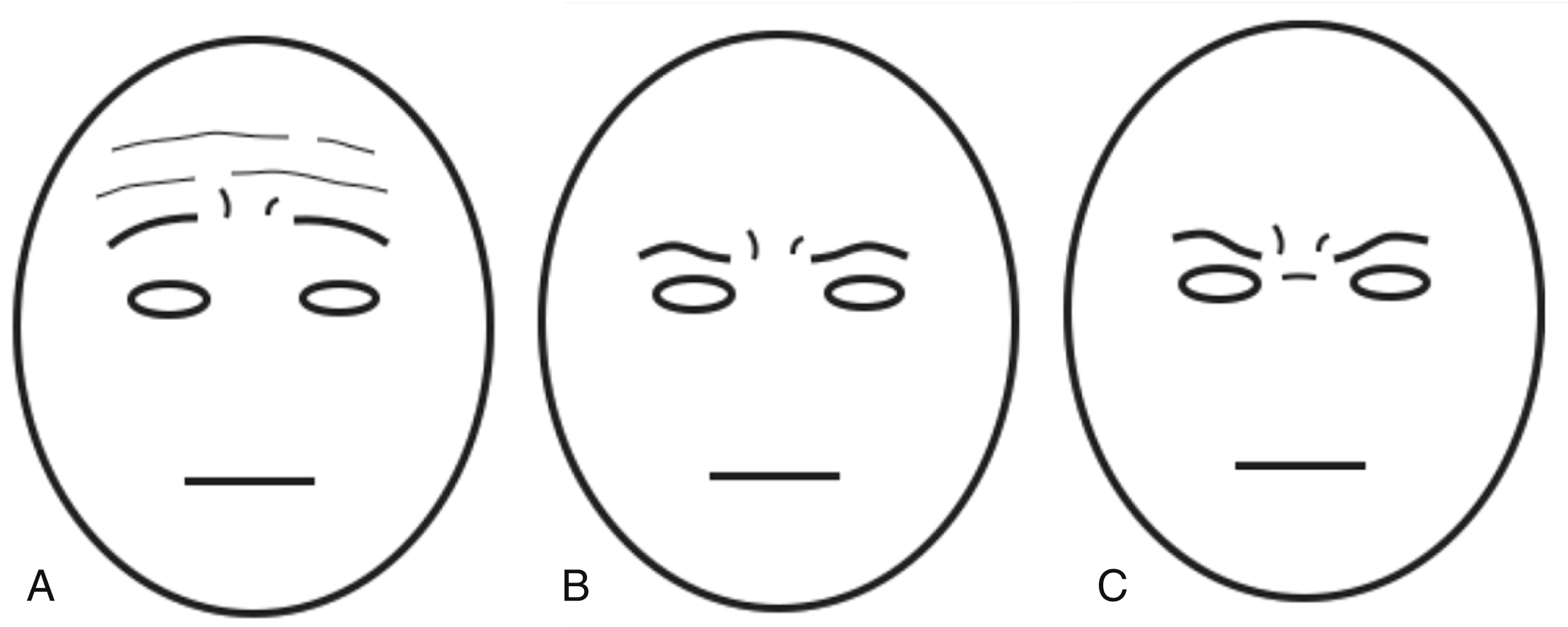
Glabellar creases (“frown lines”), usually the result of repeated squinting to aid failing eyesight or to shield the eyes from the glare of the sun, are yet another sign of the aging upper face. These creases falsely convey expressions of pain and sadness when present in conjunction with frontalis activation ( Fig. 63.7A ), or anger and disapproval when present in conjunction with procerus contraction ( Fig. 63.7B,C ).
Upper Facial Aging and Inappropriate Expressions
In the late nineteenth century Duchenne conducted landmark electrophysiological studies of the human face and proposed that the contraction of certain muscles produced specific and characteristic facial appearances that were universally understood by others to represent the expressions of human emotion. His assertion was later embraced by Darwin and his identification of the particular muscles producing specific changes in facial appearance provided the groundwork for those who study facial behavior and perform esthetic facial surgery today. While some anthropologists reject the assertion that facial muscles exist solely as a dedicated system by which to communicate emotion, there appears to be a clear neurophysiological link between our emotional state, the activity of our facial muscles, and our facial expressions.
Artists, actors, illustrators, cartoonists, and others who draw or communicate with the face are all keenly aware of the key role the movements, lines, and creases produced by the muscles of facial expression on the forehead play in conveying feelings. It is also a fact that most people can instantly recognize expressions of fear, anger, sadness, disdain, surprise, and fatigue when shown only the emoting subject’s upper face. Unfortunately, many of the changes that occur naturally over time in the aging forehead closely resemble features of these expressions, and these changes may thus be misinterpreted by others who instinctively, but mistakenly, assume we feel the way we look. Because of this, the aging face may appear inappropriately tired, disinterested, angry, disapproving, distressed or sad, even if its wearer is not (see Fig. 63.1 and Fig. 63.8 ). The “pseudoexpressions” that appear on our faces as we age affect how others perceive us and impacts significantly upon our interactions with them. Business people may appear angry or disinterested to associates and/or potential clients. Their appearance can provoke comments such as “You look like you’re having a bad day” or “What’s wrong with you?” Parents and grandparents may appear inappropriately angry or disapproving to their children and grandchildren and their appearance may compel those around them to ask “Are you mad at me?” or “Did I do something wrong?” Others may appear tired, unhealthy or lacking in vitality and their friends and family may ask or comment “You look so tired all the time,” “I hope everything is OK,” or “You look like you need to get some rest.” It is not uncommon for patients to mention at the time of their consultation that they have heard these comments, or others like them. Although they may attribute these to be the result of changes in their eyelids, the discerning surgeon will recognize them as likely to be of forehead origin and will carefully evaluate the patient’s upper face and advise her or him accordingly.
To appreciate pseudoexpressions resulting from changes in the aging forehead, the surgeon must consider the way in which the patient’s appearance might make others feel . This is often best accomplished during the consultation by pushing one’s chair back, viewing the patient’s face in its entirely and, momentarily, deferring to intuition.
One of the most frequent errors made by plastic surgeons and other surgeons seeking to rejuvenate the aging upper face is performing upper blepharoplasty where a foreheadplasty is needed. This results in part from traditional emphasis on technique rather than analysis, and misconceptions as aging of the upper face ages. It is also, in part, the result of our own artistic failings when examining patients, planning procedures, and evaluating surgical outcomes.
As the forehead ages the brow descends and infra-brow skin moves into the upper orbit producing an illusion of upper eyelid skin redundancy. This occurrence is known as “pseudoblepharochalasis” and the term’s etymology emphasizes the deceptive origins of eyelid skin “excess” and draws attention to the need to consider forehead surgery.
Attempts to treat pseudoblepharochalasis with an isolated upper blepharoplasty alone will at best result in a sad, tired-appearing patient with smoother eyelids and a long scar extending off the eyelid onto the lateral periorbital skin. More likely, however, isolated upper blepharoplasty performed where significant forehead ptosis is present usually results in a loss of the stimulus for brow elevation, further descent of the eyebrow as the frontalis muscle relaxes, and the reappearance of a pseudo skin excess in the superolateral orbit and across the upper eyelid. This, in turn, results in an exacerbation of a falsely sad, tired or disinterested appearance ( Fig. 63.9 ).
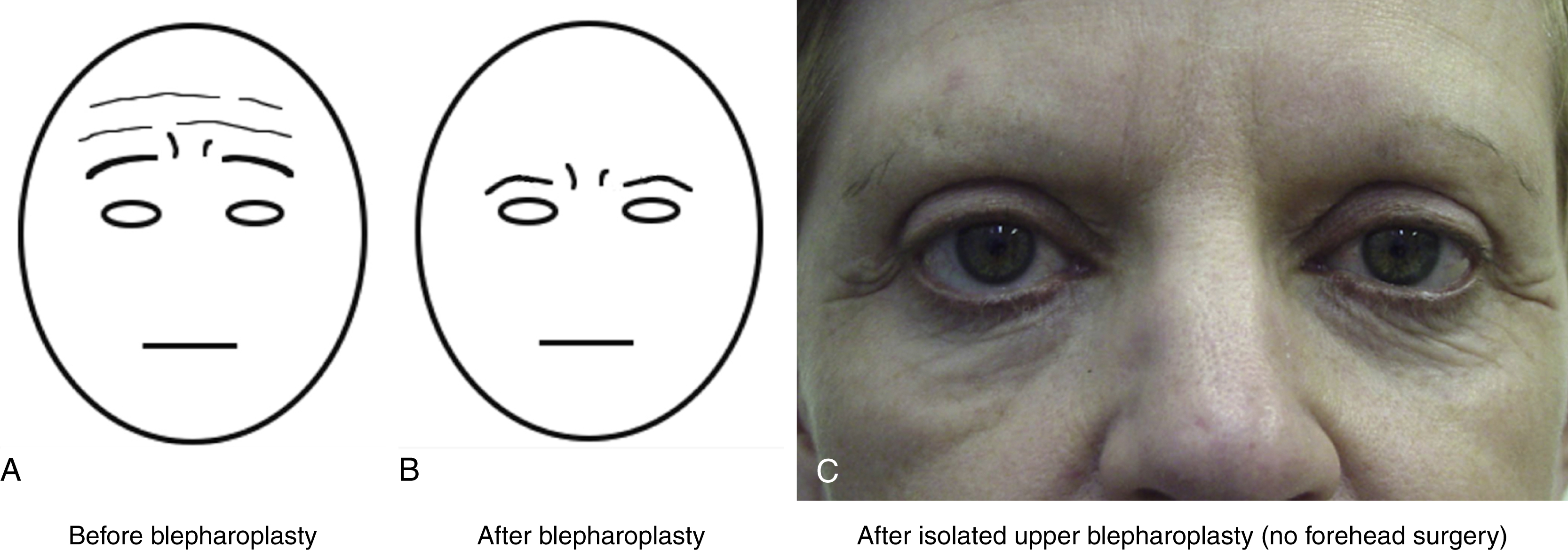
If glabellar frown lines are also present and/or a transverse wrinkle exists over the upper nose, this “pseudo-sad”/“pseudo-tired” appearance is accentuated and will take on an angry or menacing cast. This sequence of events explains why both patients and their surgeons may be disappointed with the patient’s overall appearance after upper blepharoplasty alone, despite technical proficiency in the excision of upper eyelid tissue (see Fig. 63.7 ).
Facial Asymmetry
Although it is true that facial beauty is correlated with symmetry of features and that most individuals regarded as attractive, fall within certain parameters in this regard, it is a fact that the attractive human face is inherently asymmetrical. Facial asymmetry should not, however, be regarded as an aberration, but as an inherent characteristic of beauty that makes the individual interesting, distinctive, and unique. In addition, it must be accepted by both patient and surgeon that precise right to left symmetry is not a realistic or desirable surgical goal and that forcing symmetry surgically on the face can result in esthetic imbalances and unusual, uninteresting, and unnatural appearances.
All patients undergoing surgery to rejuvenate their forehead will be found to have varying degrees of facial asymmetry and a careful examination will show each to have a “large” and a “small” eye, a “low” and a “high” orbit, and corresponding differences from right to left in hairline configuration, eyebrow position, pretarsal skin show, tarsal crease configuration, palpebral aperture opening, intercanthal tilt, and the like. These are the results, not only of subtle differences in the size of the ocular globe and adjacent structures, but differences in the position of the orbits and skeletal anatomy of the forehead and maxilla. Because of these differences, it will be artistically appropriate in many cases for the eyebrows to be at different heights after properly performed forehead lift surgery, if proper proportion and balance are to be maintained. Forcing the eyebrow situated over the smaller eye sitting in a lower, more deep-set orbit to the same height as the eyebrow situated over the larger eye often situated in a higher orbit, can make the smaller eye appear startled or surprised. In such cases it is arguably more appropriate to place the eyebrow over the smaller, lower eye in a lower position proportionate to it. Pointing out existing asymmetries and these facts preoperatively will prevent confusion on the part of the patient after surgery, when their face will inevitably be subject to closer scrutiny.
Eyebrow Esthetics and Planning Eyebrow Elevation
A traditional step in planning rejuvenation of the forehead is determining the desired position and configuration of the eyebrows. This decision should be made in conjunction with the patient and recorded on the preoperative record. Each patient should be informed, however, that these determinations represent a goal and a guideline, and not necessarily the outcome of their surgery.
Proper position and configuration of the eyebrow is ultimately a subjective judgment influenced by racial, cultural, and other factors that cannot be determined precisely by a fixed mathematical formula or arbitrary measurement. Marks, measurements, and published parameters should be regarded as guidelines only in planning surgery.
The amount of eyebrow elevation needed is usually neither the same at each point along the brow nor on each side of the face. In all but the unusual case, the majority of elevation will be needed laterally to restore attractive eyebrow configuration. The artistic imperative in most patients is to tilt up the lateral eyebrow, not to lift it and to achieve proportion and balance with other features, not precise right to left symmetry.
Accepting the fact that attractive eyebrow configuration and position are subjective and open somewhat to individual interpretation, the artist, illustrator or surgeon seeking to draw, restore or improve the appearance of the face can still benefit from guidelines as to how to proceed and a mathematical basis of beauty exists, and certain parameters can be used to assist in establishing esthetic goals.
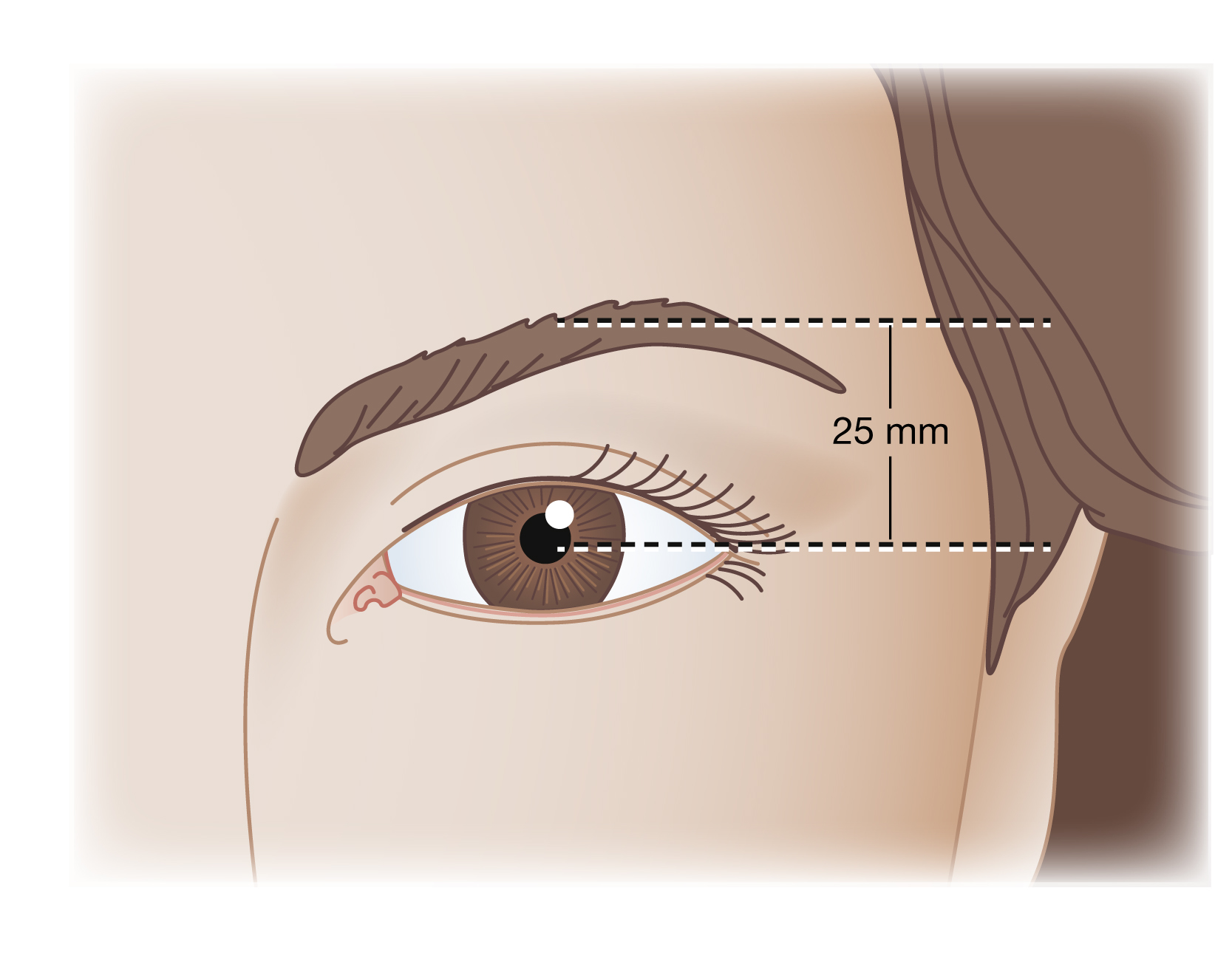
Traditionally, most surgeons have tried to define what is attractive and beautiful in simple linear and absolute terms. Often it is said that the eyebrow should sit 25 mm over the mid-pupil in relaxed forward gaze ( Fig. 63.10 ). While convenient, and useful to some extent, any such analysis is intrinsically flawed in that rigid linear measurements are ultimately inaccurate in that they assume each subject’s head and facial features to be the same size.
A more accurate and appropriate guide to what is attractive is a model based on proportion and the interrelationships of facial features. A useful system of analysis in this regard is the “divine proportion”. Also known as the “golden proportion” and sometimes referred to as the “golden cut” or “golden ratio,” this simple mathematical relationship defines a proportion that forms the foundation of what is considered to be beautiful and harmonious. As such, it can be used to establish guidelines for attractive eyebrow position and configuration.
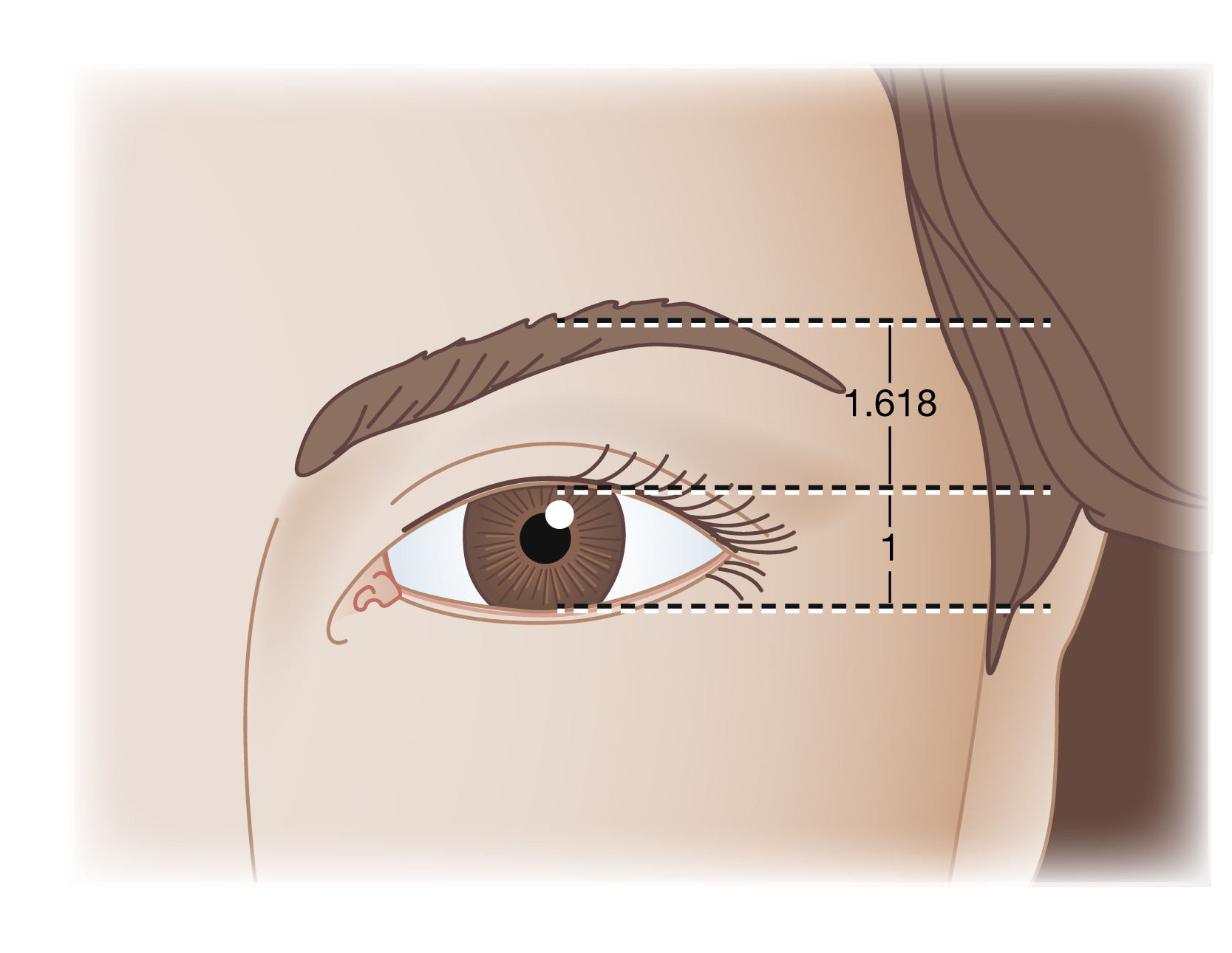
Simply stated, the golden proportion specifies that when the proportions of an object or facial feature, or relationship between two objects or facial features, can be described by a ratio of 1 to 1.618, they will appear attractive and pleasing to the eye.
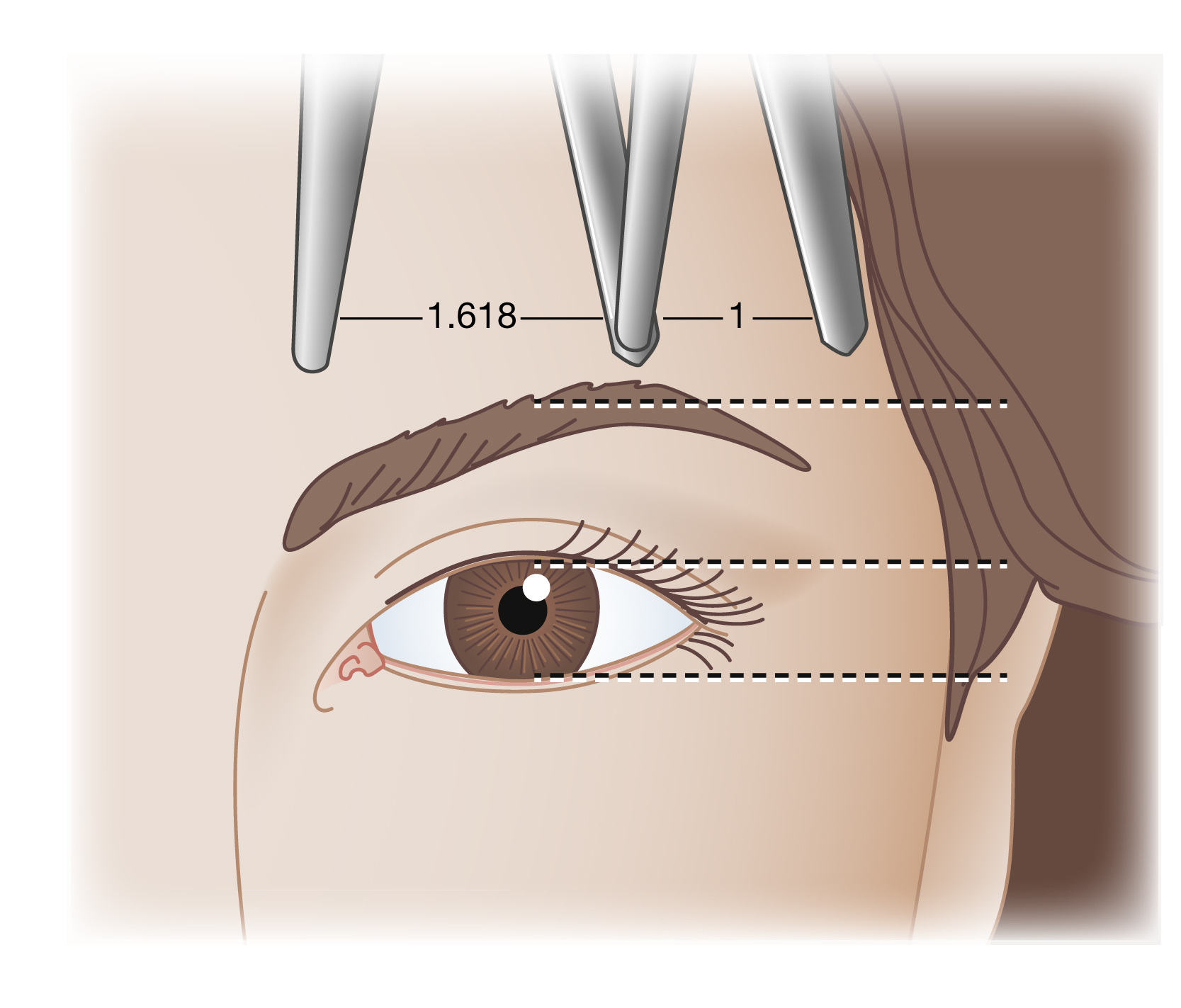
A careful analysis of the attractive upper face will show that the aperture of the eye (the vertical distance between the upper and lower eyelids in forward gaze) and the distance between the margin of the upper lid and arch of the eyebrow are related to one another by the golden proportion ( Fig. 63.11 ). Further study will show that the position of the arch of the attractive eyebrow is well described by this ratio as well ( Fig. 63.12 ).
Because the size of the globe and the height of the palpebral aperture will vary from patient to patient, so will the height of the attractively positioned eyebrow. As a practical matter, linear guidelines remain useful, if not entirely accurate, in that for the average face the height of the palpebral aperture will be approximately the same. And while calculating ideal eyebrow height from measurements of the patient’s facial features is useful and instructive in establishing surgical goals, in time the experienced and artistic surgeon will intuitively come to recognize when features fall into the golden proportion. For these surgeons, “seeing” becomes more important than measuring.
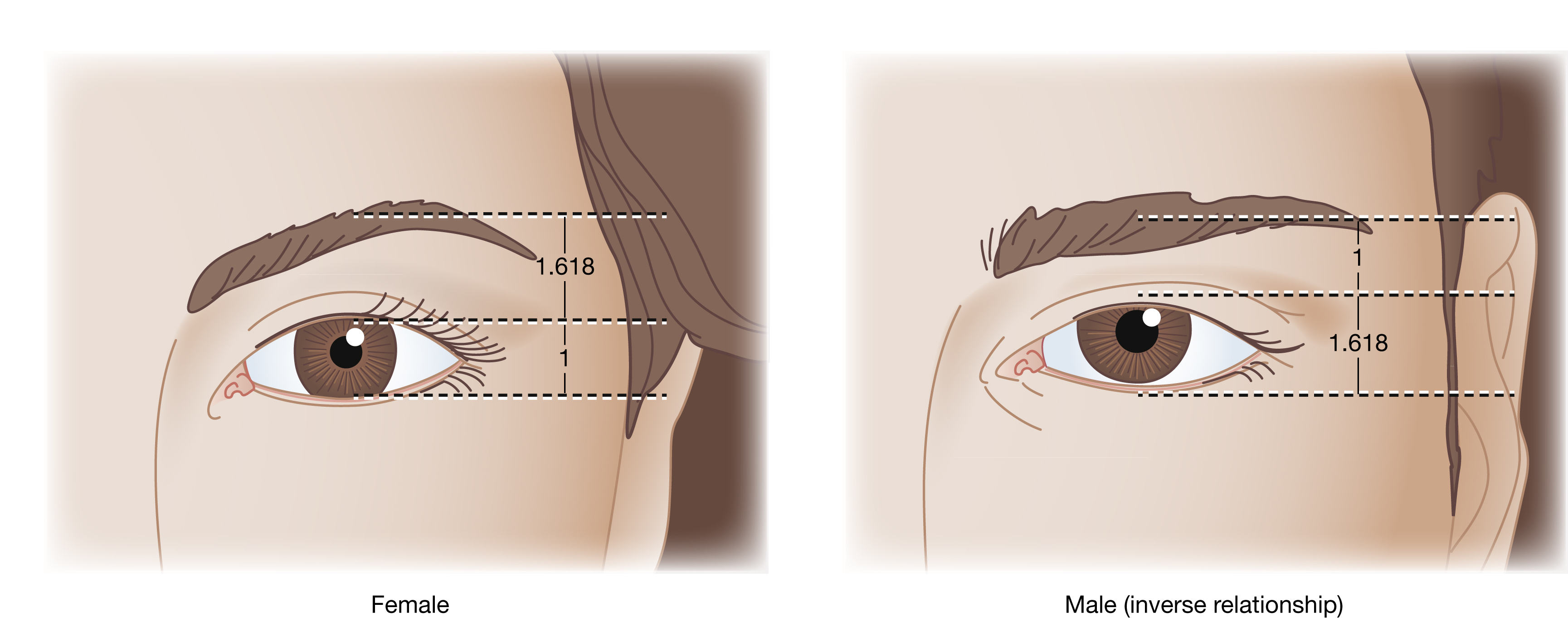
It is a commonly observed fact that male and female eyebrow positions are not the same, and intuitively obvious that eyebrow position connotes sex differences. Interestingly, for many men, the attractive eyebrow will fall in inverse relation to that of the female but remain in golden proportion to the palpebral aperture ( Fig. 63.13 ).
The golden proportion should be recognized as a guideline to eyebrow position and not an absolute ideal. Under certain circumstances a higher or lower position may be regarded as attractive. It should also be noted that the golden proportion defines classical standards of beauty. Models, actresses, celebrities and others in the public spotlight often seek to draw attention to themselves through exaggeration of what is traditionally thought of as attractive. While perhaps a professional imperative for them, the average plastic surgery patient is usually better served by setting goals more closely aligned with traditional definitions of beauty.
Eyebrow Position and Shape, and Influence on Expression
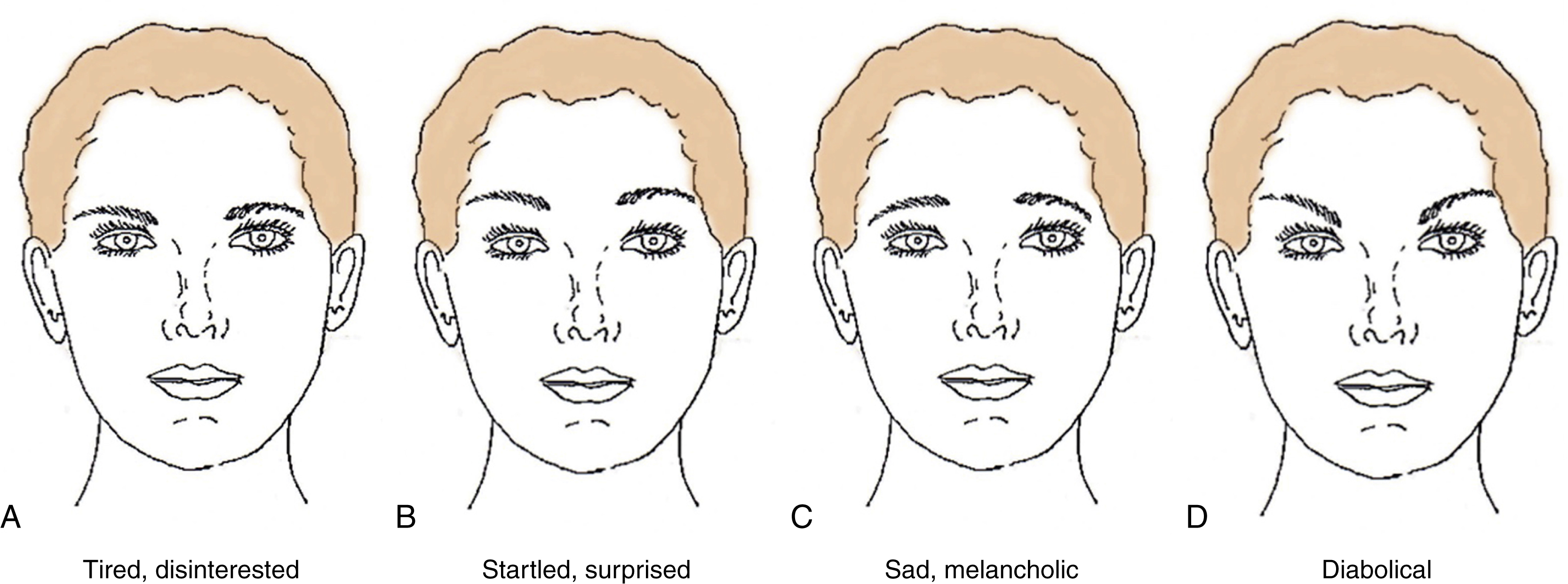
The position and shape of the eyebrow imparts the face with the appearance of certain emotions, even if the patient’s feelings are neutral (see Fig. 63.8 ). If the eyebrows are lowered, the face appears tired and disinterested. Conversely, if the eyebrows are raised, the face takes on a startled or surprised look. If the lateral brow is depressed the face appears sad and melancholic. If the lateral brow is raised, the face takes on a devilish or diabolical appearance. As such, understanding the effect of eyebrow position and shape on expression is vital to performing esthetically appropriate foreheadplasty procedures and avoiding the creation of inappropriate expressions.
What Is More Important – Eyebrow Height or Shape?
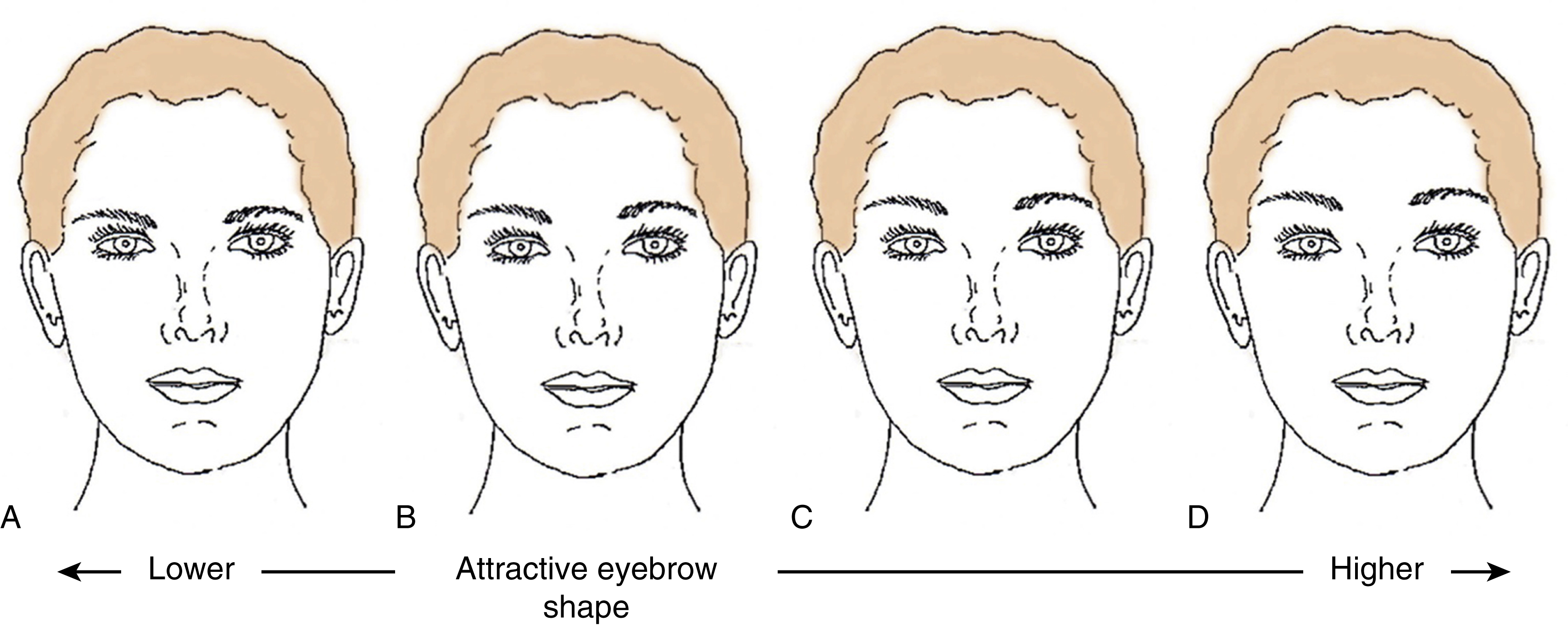
Careful consideration of the attractive eyebrow will reveal that both height and shape are important and that it is simply short sighted to define the ideal brow strictly in terms of height only. So which is more important – height or shape? This question can be answered by exploring the effect of eyebrow height in two scenarios: one in which eyebrow shape is good, and one in which eyebrow shape is poor ( Fig. 63.14 ). In Fig. 63.14 , (B) shows a schematic of a prototypical face with attractive eyebrow shape and position (eyebrow in golden proportion to the aperture of the eye). When the eyebrow is lowered, as seen in (A), an attractive appearance is still present. When the eyebrow is raised, as shown in (C), even when raised aggressively, as shown in (D), an attractive appearance is arguably still present. In fact, all faces throughout the spectrum in Fig. 63.14 arguably appear esthetic and consistent with an attractive appearance and one can conclude that if eyebrow shape is good, the face will appear attractive at a variety of eyebrow heights .
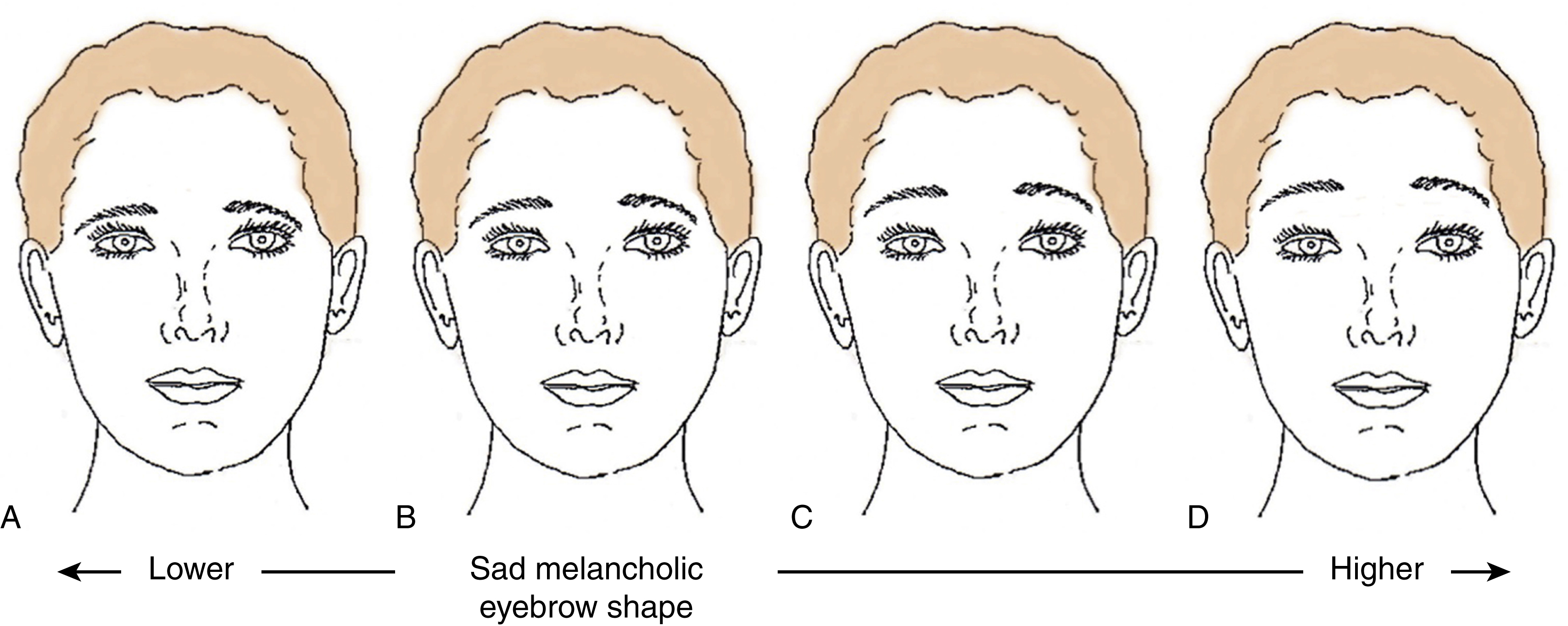
What about the effect of eyebrow height when eyebrow shape is poor? See Fig. 63.15 for details.
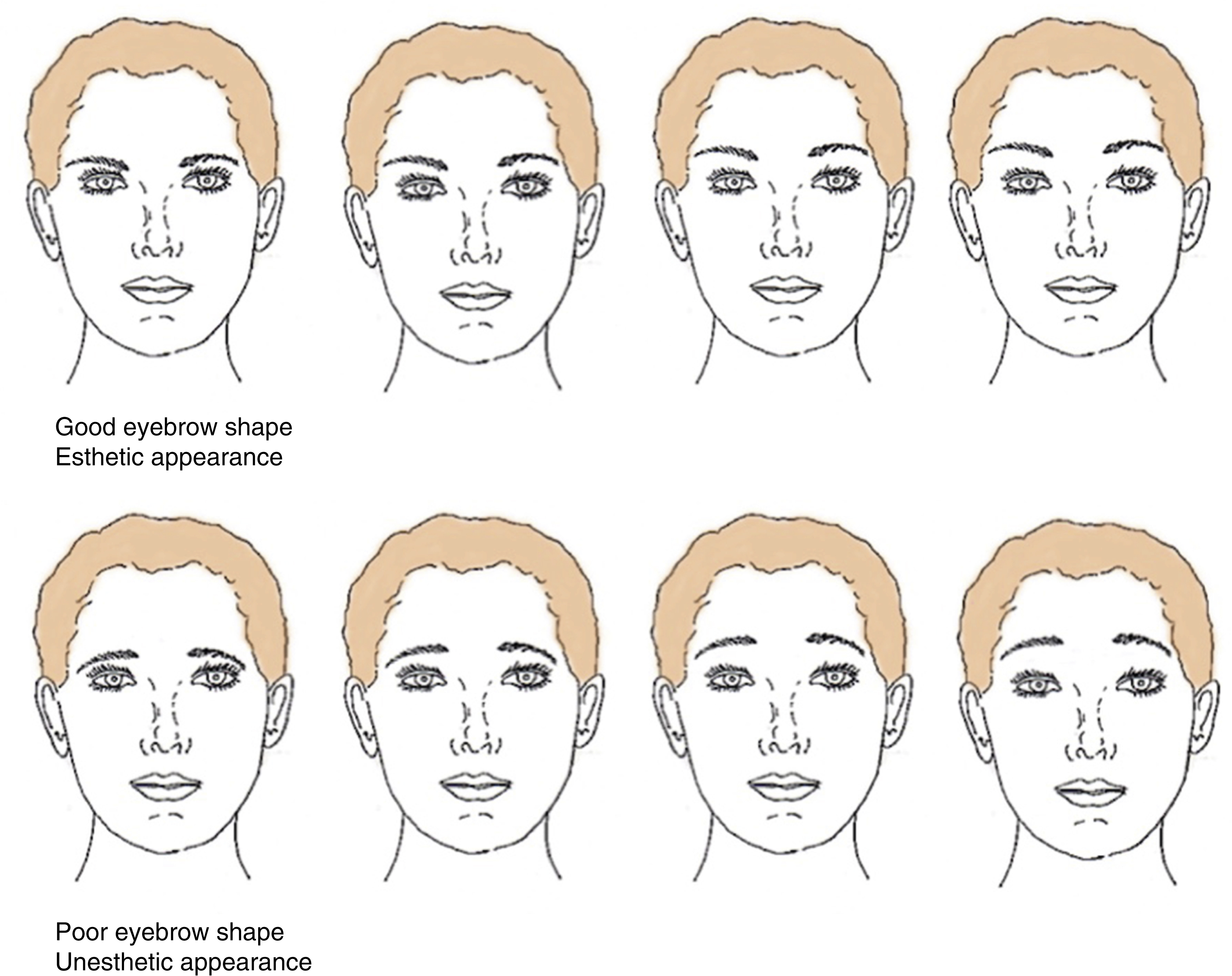
In summary, if eyebrow shape is good, esthetic appearance will be present – regardless of eyebrow height– but if eyebrow shape is poor, an unesthetic appearance will be present – regardless of eyebrow height ( Fig. 63.16 ). These observations, in turn, lead to the conclusion that eyebrow shape supersedes eyebrow height in importance in establishing an esthetic and attractive appearance, and that our surgical and artistic goal is to “tilt” the eyebrow – not “lift” it. If the foreheadplasty procedure does not produce good eyebrow shape , an attractive appearance will not be obtained.
In light of this analysis, it can be seen that the golden proportion, while a useful guideline in defining attractive eyebrow position, is not an absolute ideal. Under certain circumstances it will be seen that a higher or lower eyebrow position will be regarded as attractive. The golden proportion in particular does not explain the observation that a more highly placed eyebrow often appears attractive on the mature female face – or that young faces appear attractive with a more inferiorly situated eyebrow. Why does a high eyebrow appear more attractive on the older face? Why does a low eyebrow appear appropriate on the young face? Why does a low eyebrow appear less attractive on the mature face? The answer to these questions lies in the fact that the golden proportion system of analysis only positions the eyebrow in relation to the eye and it does not position it in relation to the orbit or take into account the characteristics of the adjacent midface or cheek. The characteristics of these structures contribute to a “young” or “old” appearance and thus are relevant in any method of analysis used to determine age-appropriate eyebrow position. The question can then be raised, is it possible that ideal eyebrow position is correlated with the overall appearance of the face and is influenced by orbital volume?
Is There a Relationship Between Lower Orbital Volume and Eyebrow Position?
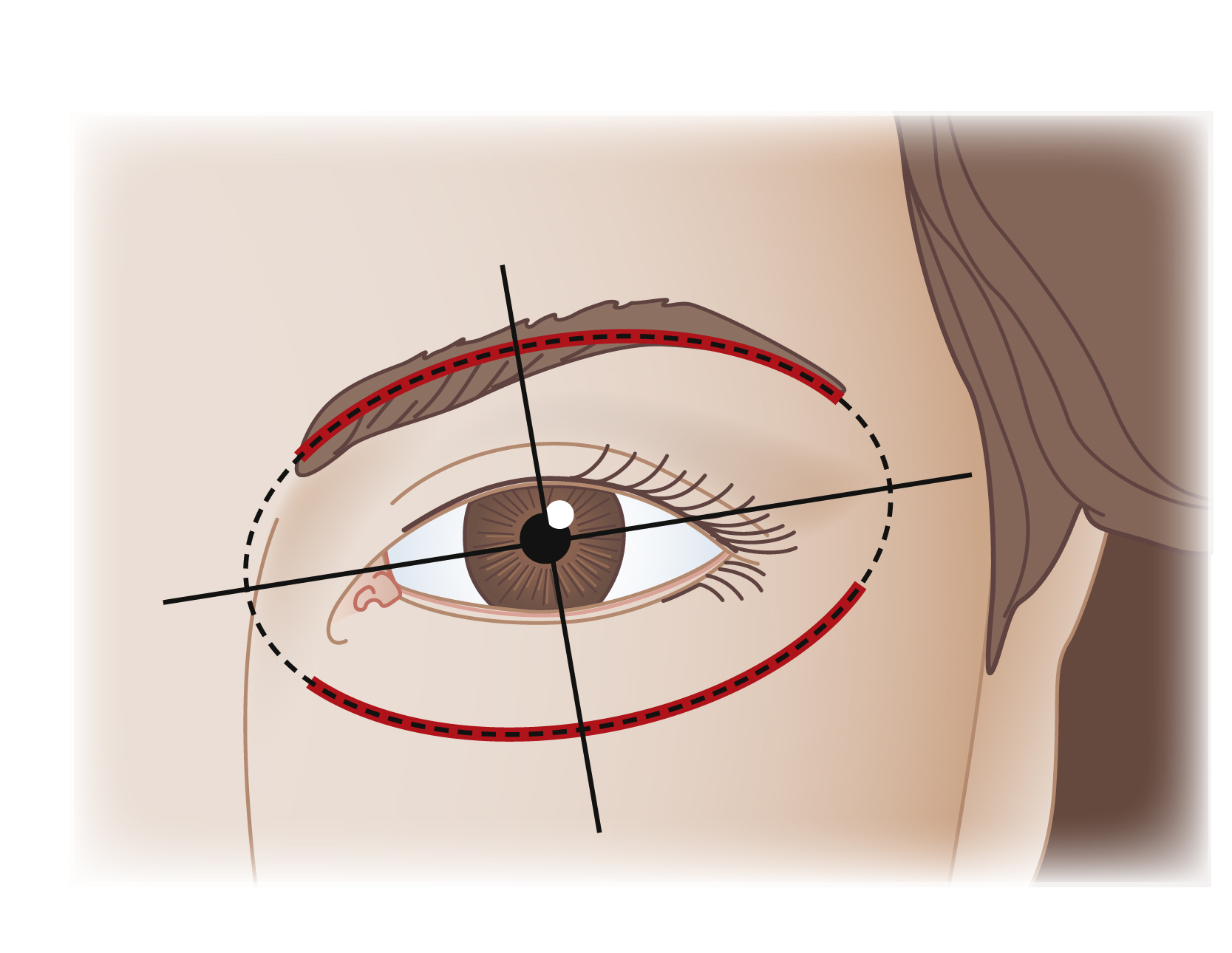
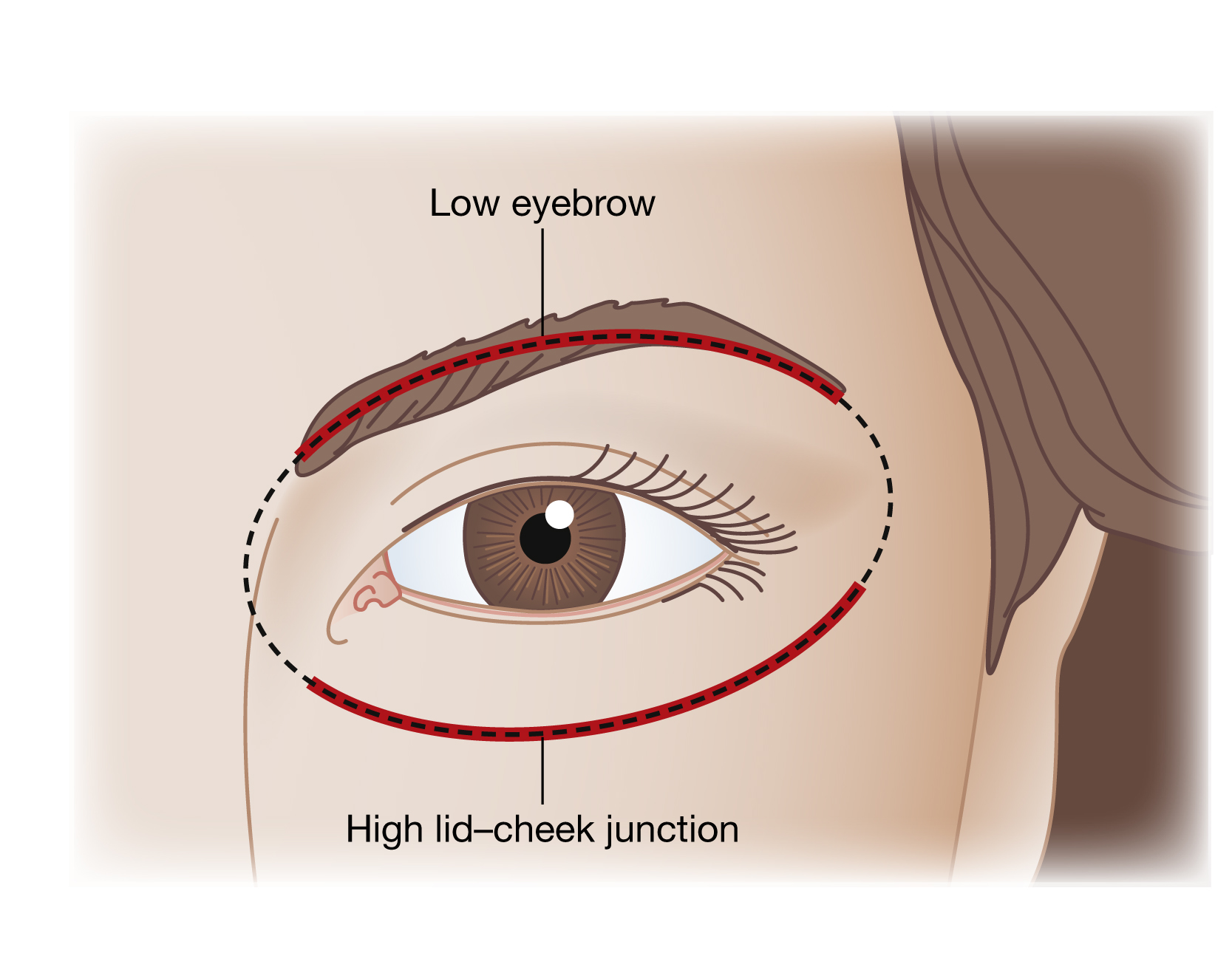
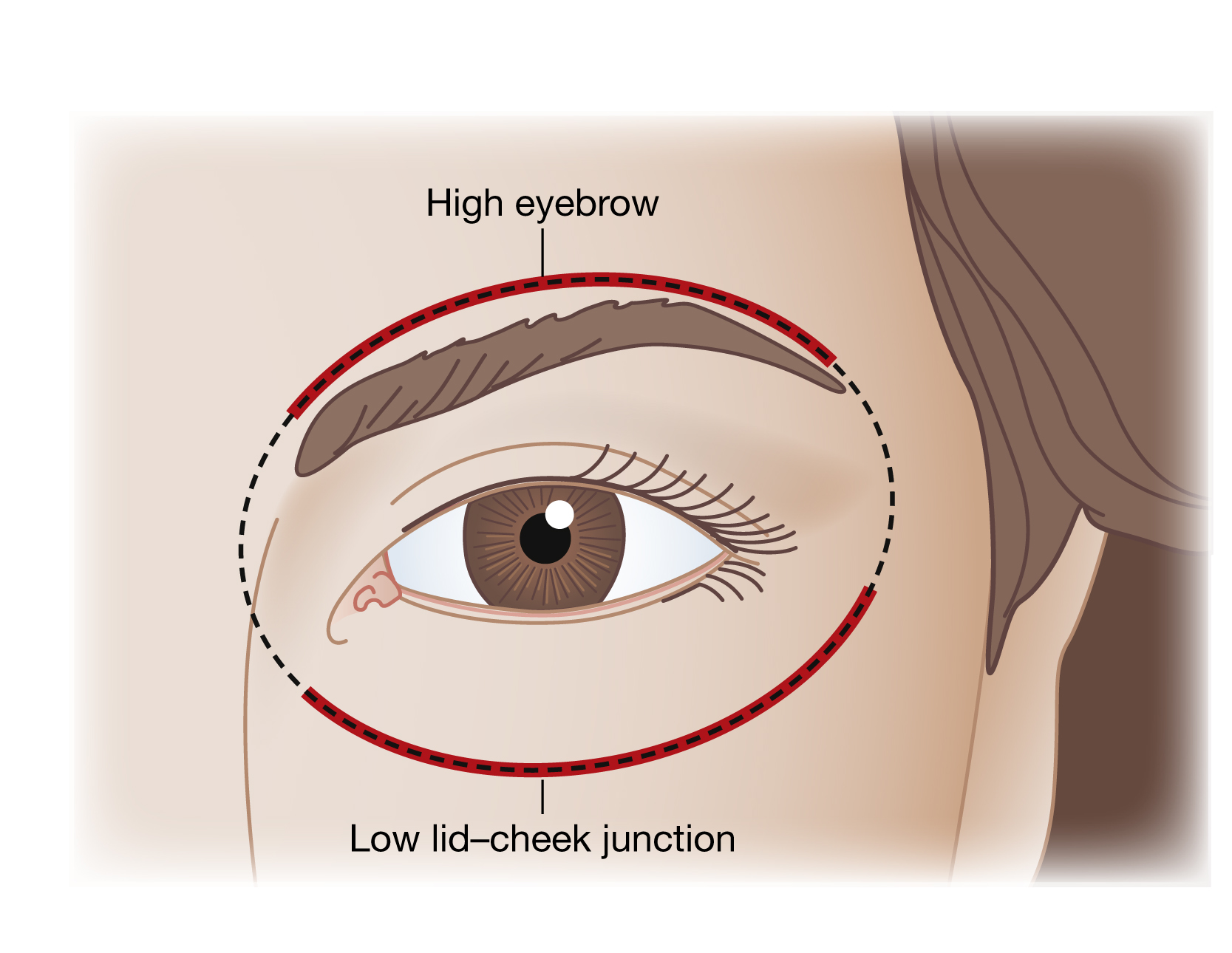
To explore this assertion we can use orbital oval analysis – a method used by estheticians and makeup artists to create attractive and esthetically pleasing eyebrows. Orbital oval analysis stipulates that the eyebrow should be situated so that the eye sits in the center of an oval defined by the brow and the lid–cheek junction ( Fig. 63.17 ).
When the lid–cheek junction is low a higher eyebrow will be necessary to maintain esthetic balance ( Fig. 63.18 ). This may explain why a high eyebrow looks better on a mature face. The mature face typically has a low lid–cheek junction as a result of midface atrophy and descent. And why a low eyebrow looks better on a young face – a young face typically has a high lid–cheek junction and when the lid–cheek junction is high a lower eyebrow may be artistically appropriate ( Fig. 63.19 ).
It can be seen that filling the lower orbit makes the eyebrow appear higher, even when its position is unchanged, and thus we must take into consideration the characteristics of the lower orbit and midface when performing esthetically nuanced foreheadplasty procedures. And once this is understood we can see that as we treat the lower eyelid more conservatively in our blepharoplasty procedures by removing less fat, and as we improve our results in the midface and as we learn to better replenish lost lower orbital volume, we may be able to treat the brow more conservatively and more closely simulate a truly youthful appearance.
Is There a Relationship Between Upper Orbital Volume and Eyebrow Position?
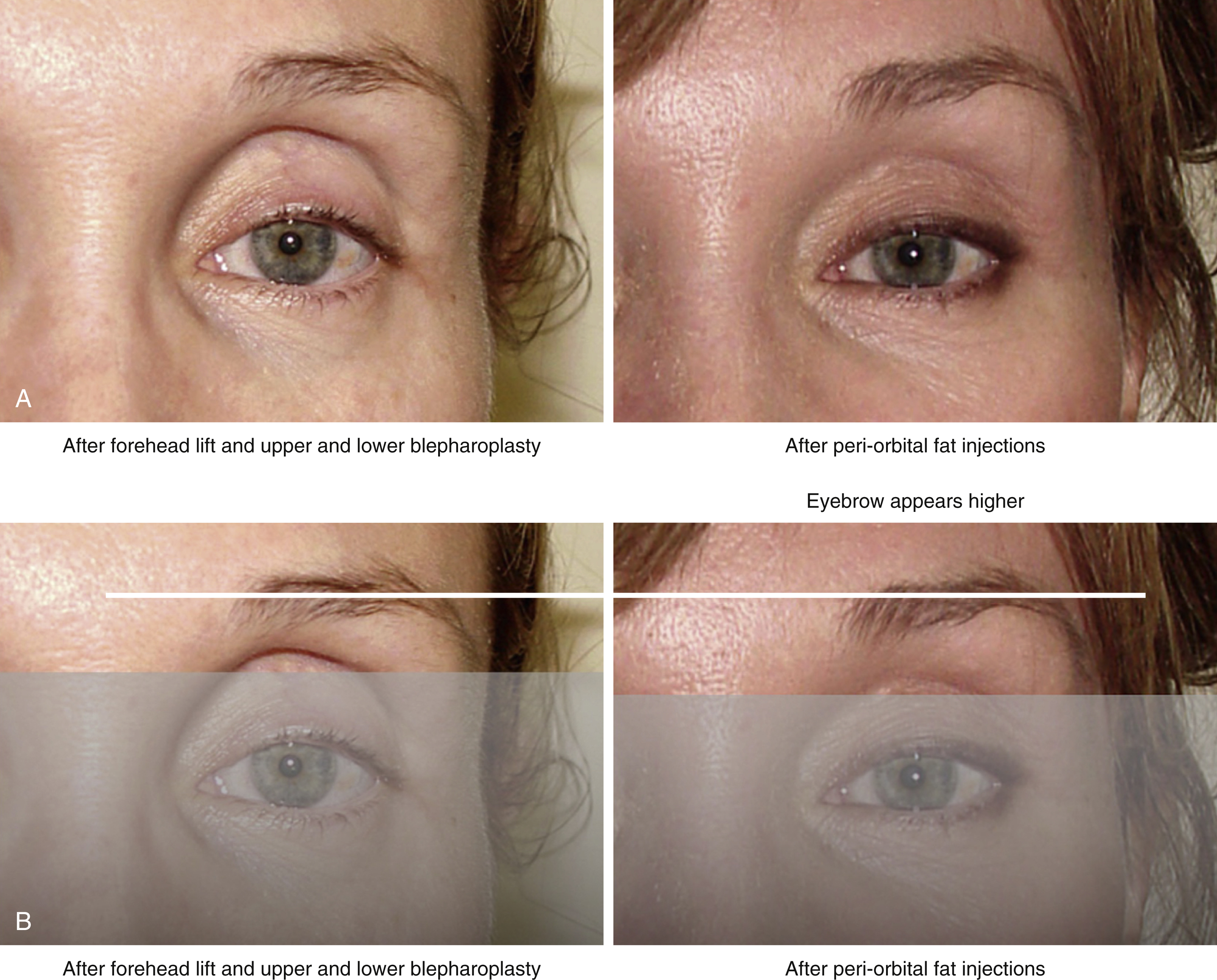
One is likely surprised to learn that there is a relationship between lower orbital volume and eyebrow position as described above, and this begs the question – is there a relationship between upper orbital volume and eyebrow position? To answer this question we can consider the effects of filling the upper orbit and the effect this has on observed eyebrow position. Fig. 63.20A (left) shows a patient after aggressive foreheadplasty and upper blepharoplasty that was performed by an unknown surgeon. The lid crease is high and the upper lid appears long – neither of which are features of a young attractive orbit. But when the lower face is masked as shown in Fig. 63.20B (left) the eyebrow appears to be in satisfactory position relative to the supraorbital rim – even though the eyebrow appears to be too high when considered relative to the pupil and not in golden proportion with the aperture of the eye. Fig. 63.20A (right) shows the same patient after periorbital fat grafting. The lid crease is now lower and the upper eyelid appears shorter (both good), but when the lower face is masked off, as shown in Fig. 63.20B (right) the eyebrow appears higher – too high – even though no foreheadplasty has been performed and the eyebrow position has not changed (white horizontal line). While the patient’s upper facial appearance has been improved by filling her upper orbit she now has a somewhat startled or surprised look. It can be seen that filling the upper orbit makes the eyebrow appear higher, even when its position is unchanged, and thus we must take upper orbital volume into consideration when performing esthetically nuanced foreheadplasty procedures. And once this is understood it can be seen that as we treat the upper eyelid more conservatively in our blepharoplasty procedures by removing less skin and fat, and as we learn to better replenish lost upper orbital volume, we may be able to treat the brow more conservatively and more closely simulate a truly youthful appearance.