The superolateral cheek can have a tendency to develop festoons, which are a product of soft tissue laxity and fluid accumulation. Despite research in the field of oculofacial plastic surgery, festoons are challenging to treat. The ultimate goal is to effectively improve these with a method that is minimally invasive and with the least recovery time. Several surgical and nonsurgical treatments are available, although each has limitations. The clinician’s knowledge of the anatomy and clinical features of festoons will guide their management. This article aims to further enhance the clinician’s expertise by delving into the current evidence-based treatment of festoons.
Key points
- •
Festoons results from a combination of fluid accumulation and soft tissue laxity in the malar area; the exact clinicopathology is poorly understood.
- •
Nonsurgical management of festoons includes tetracycline injections, soft tissue fillers, hyaluronidase, and resurfacing lasers.
- •
Surgical management of festoons includes direct excision, extended lower eyelid blepharoplasty, liposuction, and cheek lift.
Terminology and etiology of festoons
Festoons are also referred to as malar mounds, fluid bags, lower lid bags, malar edema, and saddle bags. While distinctions between malar mounds, malar edema, and festoons have been suggested based on the presence or lack of fluid accumulation [ ], it is likely that all represent a spectrum of the same underlying process over the malar eminence.
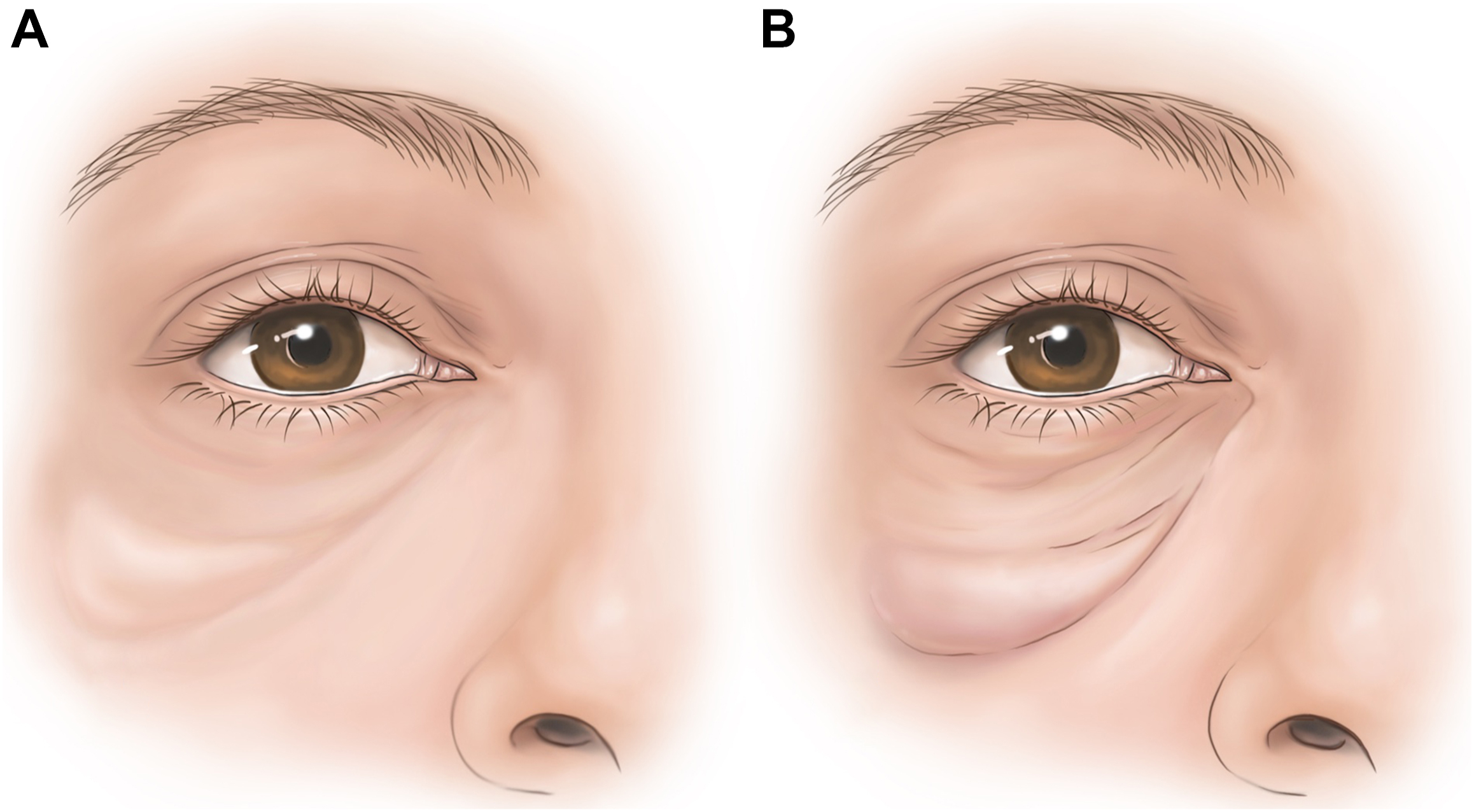
The varying definitions of festoons correspond to an equivalent lack of understanding of their etiology. In general, festoons are a result of laxity of the skin and orbicularis oculi over the prezygomatic region in addition to the orbitomalar ligament (OML) and zygomaticocutaneous ligament (ZCL) [ , ]. The resulting bulge of soft tissues can lead to fluid buildup in this area ( Fig. 1 ).
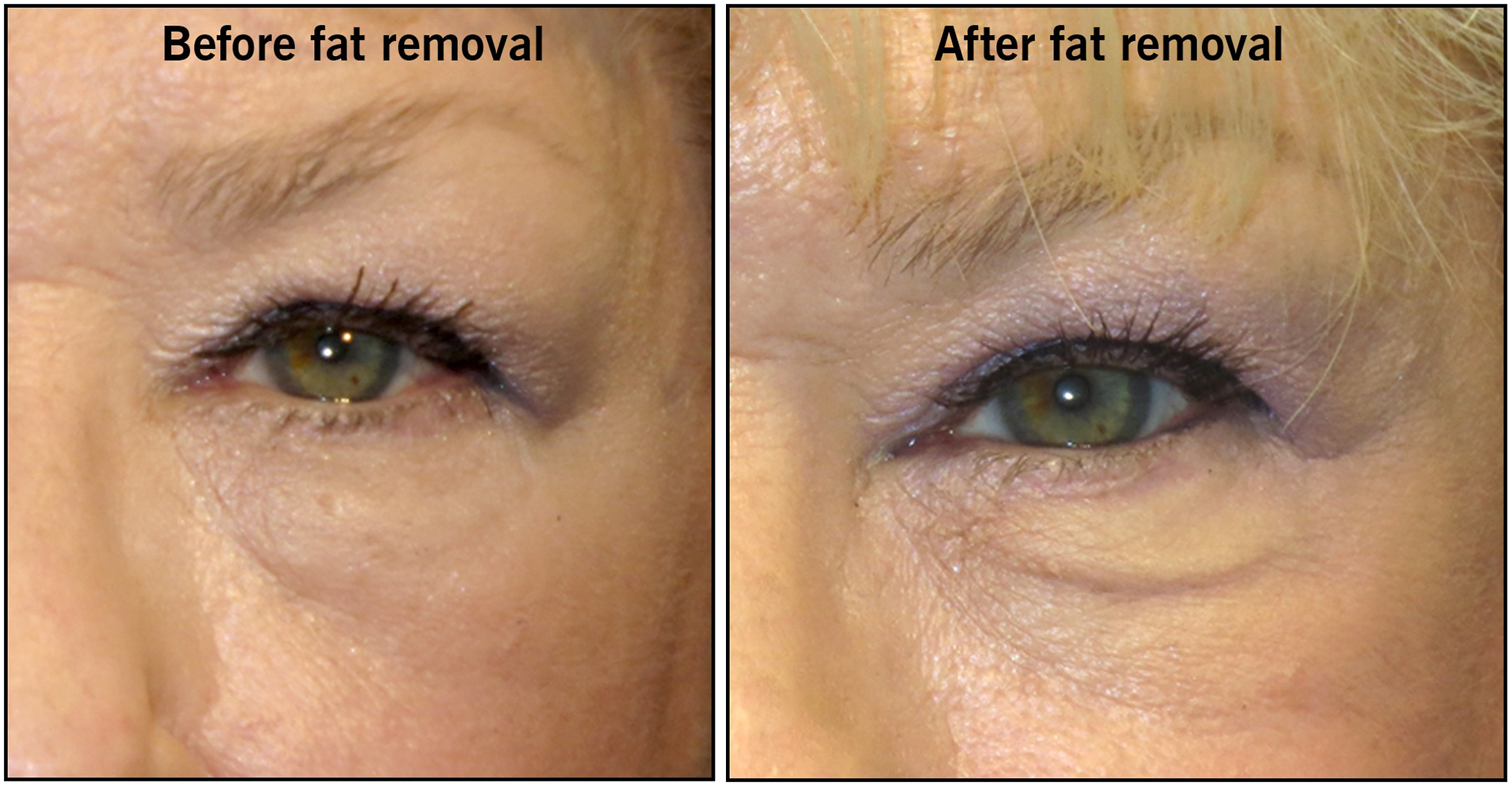
While the clinicopathology of festoons is not well understood, the changes are usually encountered in the aging population. In younger patients, the volume loss after lower eyelid blepharoplasty surgery can highlight the presence of festoons ( Fig. 2 ).
Festoon anatomy and pathophysiology
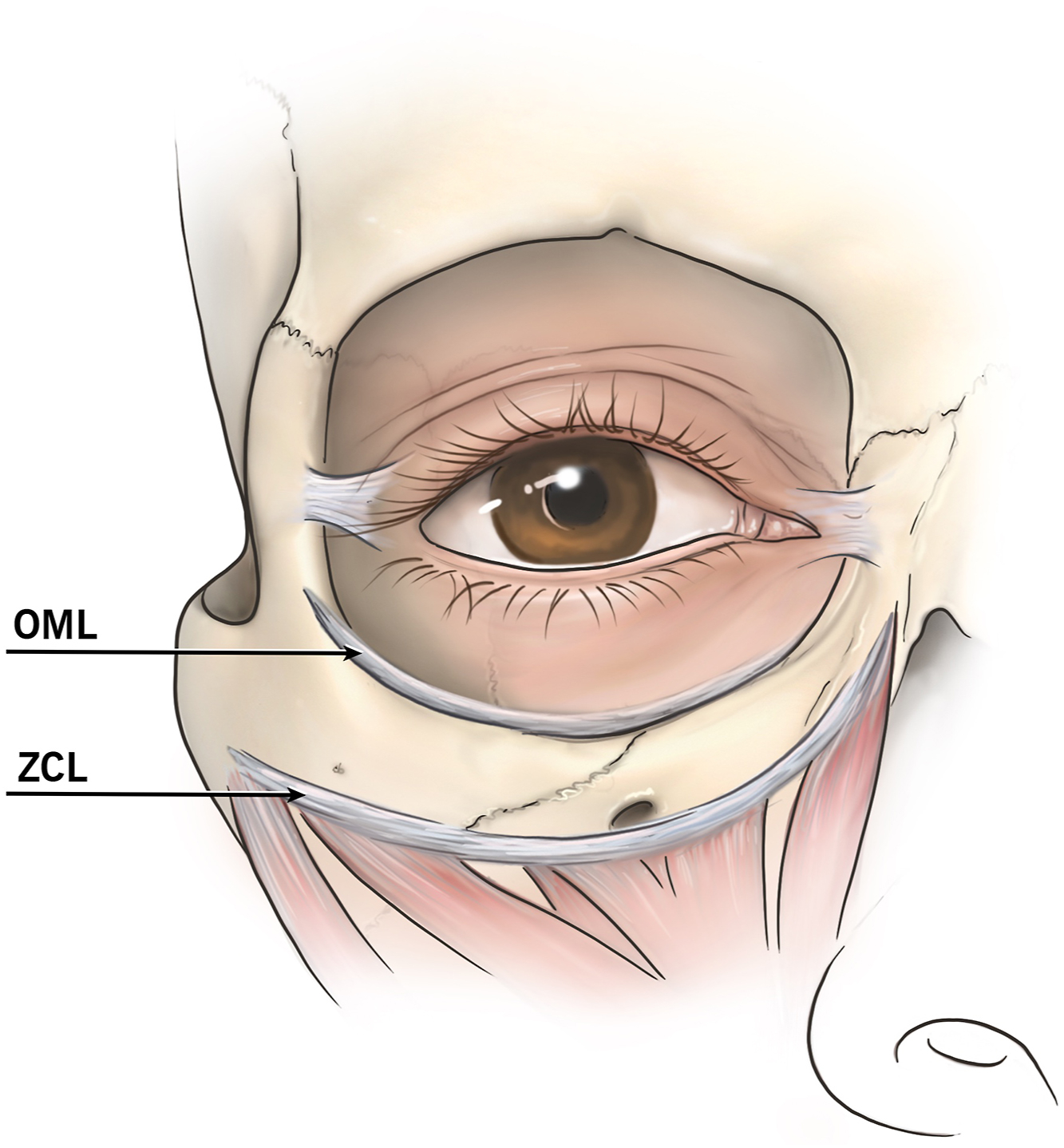
Understanding the anatomic landmarks of the prezygomatic space is important in the description of festoons. The superior limit of the prezygomatic space is marked by the lateral lid-cheek junction and the inferior limit is the midcheek [ ]. The OML, also known as the orbicularis retaining ligament, delineates the upper border and the lower border is marked by the ZCL ( Fig. 3 ). Anatomic studies have described that festoons are found between 2.5 and 3 cm below the lateral canthi [ ].
The OML originates in the inferior orbital rim, courses through the orbicularis oculi and inserts into the dermis at the lower lid-cheek junction [ ]. The OML is a key anatomic landmark in orbital fat prolapse and festoons. It is important to distinguish orbital fat prolapse, which occurs above the OML, from festoons which originate below the OML. With aging, the OML elongates and loosens thereby contributing to the appearance of festoons. At the mid-pupillary axis, the medial boundaries of the festoon converge, namely the palpebromalar groove superiorly, the tear trough medially, and the nasojugal fold inferiorly [ ].
The malar septum is a structure that is thought to divide the eye from the lower face and it emerges from the inferior orbital rim traveling inferiorly through the sub-orbicularis oculi fat (SOOF) and then inserting into the dermis of the midcheek. The union of the SOOF’s fibrous septations with the malar septum creates a barrier between the orbital rim and the skin of the cheek.
Inferiorly, festoons are delineated by the ZCL [ ]. The ZCL originates from the periosteum of the zygomatic bone and extends anteriorly into the soft tissues and dermis of the cheek, forming the midcheek furrow [ ].
An association between prolonged postoperative edema and festoons has been made, suggesting that festoons might originate from the lymphatic system [ ]. Anatomic studies of the lymphatic drainage of the lower eyelid region have revealed that deep lymphatic vessels travel along the anterior aspect of the prezygomatic space, deep to the preseptal orbicularis oculi and within the SOOF to drain into the preauricular and submandibular lymph nodes [ ].
A myriad of systemic inflammatory conditions and allergic responses can cause periocular edema and aggravate festoons. Specifically, acne rosacea, systemic lupus erythematosus, sarcoidosis, dermatomyositis, and angioedema can all be associated with more prominent festoons [ ]. Allergies to ocular and periocular topical medications, namely glaucoma drops, topical ophthalmic antibiotics, and cosmetics can also be implicated.
Festoons and persistent eyelid edema can be commonly encountered in patients with ocular rosacea. The periocular skin becomes thickened, erythematous, and edematous with visible telangiectasias [ ]. The pathophysiological changes associated with rosacea can lead to fibrosis of the periocular lymphatic channels, further worsening festoons. Chronic lymphedema of the eyelids can also be seen in patients with Morbihan disease, a poorly understood disease process that is challenging to treat [ ].
The effect of gravity and positional changes on facial features has been studied, revealing that a supine position (compared to the upright position) reduces the appearance of cheek volume, steatoblepharon, tear trough, festoons, and nasolabial folds [ ]. This further supports that laxity of the eyelid and cheek tissues is directly implicated in the appearance of festoons. However, even in the absence of tissue laxity, festoons could be encountered as a congenital condition. Contrary to acquired festoons, which improve with lateral pulling of the eyelid and forceful eyelid closure and worsen after periocular botulinum toxin, congenital festoons do not resolve with these maneuvers and are unchanged after periocular botulinum toxin [ ]. The finding of festoons worsening after periocular botulinum toxin stems from a case study where injections were placed in the lateral canthus and infraorbital region. The resultant weakening of the orbicularis oculi decreases its ability to pump fluid and results in edema [ ].
Fillers, specifically hyaluronic acid gel (HAG)–based ones, have been shown to worsen and promote the formation of festoons in approximately 15% of patients [ ]. The hydrophilic properties of HAG fillers are thought to be implicated as a direct cause of worsening of festoons, which in some cases may be reversed by hyaluronidase injections [ ]. However, in some patients improvement may not be observed despite multiple hyaluronidase injections.
Clinical evaluation of festoons
Pertinent Medical History
Prior to considering treatment options, it is important to evaluate for treatable or modifiable contributing factors to eyelid edema. Oral medications such as hormonal supplements, prednisone, angiotensin-converting-enzyme inhibitors, nonsteroidal anti-inflammatory drugs, and topical ocular medications causing allergic reactions should be discontinued for at least 2 weeks to determine if there is improvement in the festoons [ ]. Systemic conditions such as hypoproteinemia, cardiac failure, lymphedema, and hypothyroidism should also be evaluated. Ophthalmologic disease processes like thyroid eye disease, floppy eyelid syndrome, blepharochalasis, and ocular rosacea should be addressed.
Clinical Examination
A systematic approach to the physical examination and knowledge of the anatomy of festoons will assist the clinician in the differentiation of festoons from other entities such as steatoblepharon (lower eyelid fat prolapse). Festoons assume a triangular shape below the prolapsed orbital fat. It should be noted that in aged individuals, the orbital fat may drape somewhat below the level of the inferior orbital rim but there will be a demarcation between the fat prolapse and the festoon by the OML.
The lower eyelids should be assessed for laxity via the snapback and/or the eyelid distraction tests. There are 2 main methods for evaluating festoons: the pinch test and the squint test [ ]. First, the skin overlying the festoon is pinched at various sites to determine how much of the festoon is occupied by the orbicularis oculi bulk, which assists in differentiating if the festoon is mainly fluid filled or mostly composed of soft tissue. For the squint test, the patient squeezes their eyes closed to assess the laxity of the orbicularis oculi. If there is significant laxity, the festoon will improve with squeezing but if fat is the main contributor, then the festoon will not improve.
We encourage supplementing the aforementioned examination with clinical photodocumentation as it provides the clinician and patient a framework for managing expectations and understanding patient-specific anatomic features.
Managing festoons
Nonsurgical Approaches
Nonsurgical treatments for festoons are off-label and have variable efficacy in improving festoons. Risks should be thoroughly discussed with the patient.
Dermal Fillers
As described earlier, HAG fillers can make festoons more prominent due to their hydrophilic properties. However, careful injection of HAG fillers into the surrounding volume-depleted areas can help mask the appearance of the festoons [ ]. Care must be taken to avoid overcorrection since it may stretch the ZCL and OML ligaments and worsen posttreatment edema [ ].
Hyaluronidase
Even in the absence of previous filler injections, hyaluronidase has been empirically used to treat festoons but, in our experience, does not produce lasting effects [ ]. Systemic diuresis with spironolactone 25 to 25 mg/day can be offered to select patients.
Lasers
Skin resurfacing lasers with CO 2 and Er:YAG may improve mild festoons in cases where there is mild skin laxity [ ]. Microneedling radiofrequency technology has been employed in the treatment of rhytids as the thermal energy combined with microscopic injury to the skin promotes collagen and elastin proliferation [ ].
Sclerosing Agents
Sclerosing agents such as tetracycline and doxycycline have been used in the nonsurgical treatment of festoons [ , ]. The proposed mechanism of action of tetracyclines is inhibition of matrix metalloproteinases and promotion of fibroblast proliferation thereby inducing sclerosis in tissues. A study on the long-term experience with tetracycline injections for festoons demonstrated that there was improvement in 59% of treated patients, and the improvement was noted 2 months after treatment in most patients. The side effect profile includes discomfort, swelling, and bruising [ ]. A preliminary report on the use of doxycycline injections for festoons has been published but further studies are evaluating its safety and efficacy [ ].
Surgical approaches
Direct Festoon Excision
In patients with significant skin laxity, direct festoon excision is a surgical option [ , ]. The goal is to excise skin and subcutaneous tissue to eliminate the potential space for fluid collection. Direct festoon excision does not address orbicularis laxity, and thus an adequate preoperative evaluation of orbicularis laxity and lower eyelid laxity should be performed. Lateral canthal resuspension should be offered in patients with significant horizontal eyelid laxity to prevent postsurgical eyelid retraction. Patient selection is key as the intervention results in a visible scar and festoons can recur.
Skin-Muscle Flap
When both skin and orbicularis oculi laxity are significant, an extended lower eyelid blepharoplasty (skin-muscle flap) can be performed to tighten the tissues anterior to the festoon. A subciliary incision is performed and excess tissue is excised. The technique can be combined with suspension of the orbicularis to the periosteum of the orbital rim and/or lateral canthal resuspension to decrease the risk of eyelid retraction [ ]. While the skin-muscle flap can conceal festoons in some patients, recurrence and undercorrection are possible since this technique does not address the underlying ligaments.
Cheek Lift/Midface Lift
The purpose of a midface lift is to release the ligaments bordering the festoon and augment the vertical elevation of the superficial musculoaponeurotic system (SMAS) [ ]. The OML and the malar septum are released to treat malar descent, festoons, deep melojugal sulci, and tear trough deformity [ ]. The technique is based on a subperiosteal dissection either through a lower eyelid blepharoplasty or transconjunctival incision. The dissection is performed to the zygomatic buttress and the zygomatic mound is resuspended superotemporally to the deep temporal fascia.
A subperiosteal vertical upper-midface lift combines temporal and buccal incisions to mobilize the midface tissues and the SMAS fascia. Sutures are passed in the subperiosteal plane to reposition the midface soft tissues and suspend them to the deep temporalis fascia [ ]. After the midface is resuspended, an orbicularis muscle flap is performed laterally to address orbicularis laxity and remove excess lower eyelid skin.
A triple-layer midface lift has been described for the midface lift. In this technique, the postseptal fat, the SOOF, and the skin and orbicularis oculi are addressed thus redraping the orbital fat and providing a vertical lift to the SOOF and skin/orbicularis complex [ ]. Access via a subciliary incision is performed followed by a preperiosteal dissection. Release of the arcus marginalis allows the orbital (postseptal) fat to herniate and then it is sutured inferior to the inferior orbital rim. Then, the SOOF is lifted and suspended to the periosteum of the lateral orbital rim.
Liposuction
Liposuction of the subcutaneous fat by itself does not address skin, orbicularis oculi laxity, or the edema present in festoons. The technique entails an incision at the lateral canthus through which a cannula is inserted in the subdermal plane to remove the fat [ ]. An alternative technique combines liposuction with orbicularis suspension via a midface lift thereby mobilizing the OML and malar septum [ ].
Different to the treatment of acquired festoons, fat excision of the supraorbicularis fat in the prezygomatic area is key in the surgical approach to congenital festoons. A midface lift with release of the OML and ZCL is combined with subcutaneous fat removal [ ].
While treating festoons is a challenging topic in the field of oculofacial surgery, there are various surgical and nonsurgical treatment options that can be tailored to patient anatomy and expectations. Ongoing studies will help elucidate the underlying pathophysiology of festoons and guide newer and more effective treatments of festoons and aging of the midface.
Clinics care points
- •
The underlying pathophysiology of festoons is unclear.
- •
Hyaluronic acid based fillers can promote the formation of festoons.
- •
Tetracycline injections for treatment of festoons are effective in 59% of patients.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


