CHAPTER 19 Fat Repositioning in Lower Blepharoplasty
The objective of facial rejuvenative surgery is to restore a youthful contour. With age, changes occur in the lower eyelid and cheek that involve descent of the cheek tissues as well as prolapse of orbital fat in the lower eyelid. Perhaps even more importantly, deflation occurs: there is loss of volume in the subcutaneous and deep fat pads in the periorbital region. Val Lambros1 (see Chapter 2) has articulated beautifully the concept that focal loss of volume, often in areas of cutaneous attachment of the skin to deep structures, can mimic descent of the soft tissue. In the periorbital area, focal loss of volume along the orbital rim can unveil the contours of the orbital fat bound by the arcus marginalis, and of the suborbicularis oculi fat (SOOF) limited by the orbitomalar ligament. This results in the formation of a tear trough groove at the level of the inferior orbital rim. Filling the areas of periorbital deflation can be a powerful rejuvenative technique. One useful option, when adequate orbital fat is available for transposition, is the transposition of fat over the orbital rim onto the superior face of the maxilla. In this chapter, I will describe the transconjunctival approach to orbital fat repositioning.
Lower eyelid fat transposition is a step in the evolution of blepharoplasty surgery. Thirty years ago, lower blepharoplasty was viewed as an operation to remove skin and fat in the lower eyelid. This often produced rounding of the lateral canthal angle, lower eyelid retraction with scleral show, and did not improve skin quality in the lower eyelid. The transconjunctival approach to fat excision was reintroduced 20 years ago, and over the last 10 years, we have been simultaneously treating skin quality with chemical peeling and ablative or non-ablative laser treatments. The newest stage of evolution of lower blepharoplasty is an understanding of the concept of fat preservation. Loss of fat in the face is an aging change. Although some young patients do have a true excess or atypically prolapsed orbital fat compartment with a substantial bulge in the lower eyelid that is treated with fat removal, many older patients who come in for rejuvenation of the lower eyelid and midface have contours that are characterized by hollows over orbital rim. This contour is related to the bony support of the underlying maxilla and is accentuated when the maxilla is relatively hypoplastic. A tear trough deformity is unveiled by deflation of the overlying tissues; it is located along the inferior orbital rim between the demarcation of the septal attachment above and the cheek fat pad and SOOF below. When deflation results in a tear trough depression or orbital rim hollow, removing orbital fat alone may accentuate the tear trough deformity. For these patients, who present with a double convexity contour of the lower eyelid and cheek, the orbital fat is better repositioned over the rim rather than excised.
Surgical technique
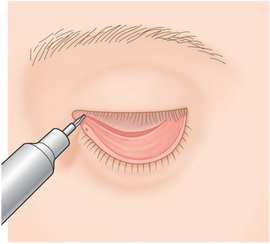
The tear trough is marked with a surgical marking pen on the skin surface before surgery begins, in order to guide the intraoperative placement of the fat pedicle. The initial portion of the surgery is identical to any other transconjunctival blepharoplasty, with a forniceal incision and wide open sky exposure of the individual fat pockets (Fig. 19-1). The lateral and central fat pockets may be debulked as determined preoperatively.
Next, the arcus marginalis is identified. The inferomedial orbital rim is palpated with the tips of a Stevens’ scissors and blunt dissection on the palpable bony orbital margin reveals the white tissue condensation representing the arcus marginalis (Fig. 19-2). Cutting cautery is useful to control bleeding from the small bony perforators that sometimes occupy this area, and to cut through the periosteum to reach the bony surface of the maxilla. Dissection is then carried out over the orbital rim by lifting the periosteum using a sharp elevator, taking care to keep the arcus marginalis and orbital septal attachment intact. The entire area of intended fat pedicle placement is undermined guided by the previously placed blue marks (Fig. 19-3). Some surgeons have suggested that the suborbicularis (supraperiosteal) plane is preferable. However, the subperiosteal plane has the advantage of being relatively blood free and straightforward. The periosteum in this area is fairly loose and the fat can be easily repositioned into the subperiosteal pocket.
Related posts:
 Upper Blepharoplasty Combined with Levator Aponeurosis Repair
Upper Blepharoplasty Combined with Levator Aponeurosis Repair
 Brow Lift Techniques
Brow Lift Techniques
 Transconjunctival Approach to Resection of Lower Eyelid Herniated Orbital Fat
Transconjunctival Approach to Resection of Lower Eyelid Herniated Orbital Fat
 Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
 Eyelid and Facial Laser Skin Resurfacing
Eyelid and Facial Laser Skin Resurfacing
 Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


